Você também pode gostar
- TMJ Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandTMJ Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- TMDDocumento170 páginasTMDVinaya Srinivasan100% (2)
- TMJDocumento66 páginasTMJmounika50% (2)
- Interactions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionNo EverandInteractions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionAinda não há avaliações
- TMJ DisordersDocumento30 páginasTMJ DisordersDua'a Ma'an100% (3)
- TMJ CompleteDocumento54 páginasTMJ CompleteNeal Torwane100% (3)
- Temporomandibular Disorders: DR Teo Ying YiDocumento19 páginasTemporomandibular Disorders: DR Teo Ying YiYing Yi TeoAinda não há avaliações
- TMJ DislocationDocumento56 páginasTMJ DislocationAlok BhardwajAinda não há avaliações
- Temporomandibular Joint: Aditi PGT 1 YearDocumento27 páginasTemporomandibular Joint: Aditi PGT 1 Yearsachin mishraAinda não há avaliações
- Temporomandibular Joint Disorders: Presented by D.Ramya Priya CRIDocumento55 páginasTemporomandibular Joint Disorders: Presented by D.Ramya Priya CRIRamya PriyaAinda não há avaliações
- Muscles of MasticationDocumento114 páginasMuscles of MasticationVasundhra MittalAinda não há avaliações
- Temporomandibular DisordersDocumento45 páginasTemporomandibular DisordersMohsin HabibAinda não há avaliações
- Diagnostic Imaging of The Temporomandibular Joint 2008Documento62 páginasDiagnostic Imaging of The Temporomandibular Joint 2008Heba S RadaidehAinda não há avaliações
- TMJ ExaminationDocumento17 páginasTMJ Examinationsamhita100% (1)
- Anatomy of Temporomandibular Joint: Presented byDocumento124 páginasAnatomy of Temporomandibular Joint: Presented bylkjhgfdsalkAinda não há avaliações
- Seminar 12 Management of TMD WordDocumento18 páginasSeminar 12 Management of TMD WordAlka Rose JamesAinda não há avaliações
- TMJ DisordersDocumento20 páginasTMJ DisordersDr. Hesham Zaatar100% (2)
- Temporomandibular Joint DisorderDocumento9 páginasTemporomandibular Joint DisorderTannels100% (1)
- Occlusal Splints in TMJ RXDocumento14 páginasOcclusal Splints in TMJ RXspu123Ainda não há avaliações
- TMJ and Temporomandibular Joint Disorder: Dr. Soukaina RyalatDocumento47 páginasTMJ and Temporomandibular Joint Disorder: Dr. Soukaina RyalatJohan Edward Franklin MarpaungAinda não há avaliações
- Stomatognathic SystemDocumento71 páginasStomatognathic SystemRaj Singh83% (6)
- Muscles of MasticationDocumento200 páginasMuscles of MasticationzinniaAinda não há avaliações
- TMJ PPT 130516130311 Phpapp02Documento120 páginasTMJ PPT 130516130311 Phpapp02Hoang NhanAinda não há avaliações
- Growth and Development of Mandible KiranDocumento92 páginasGrowth and Development of Mandible Kirannavjotsinghjassal100% (1)
- Basic Concepts of OcclusionDocumento107 páginasBasic Concepts of Occlusionaparna mohananithaAinda não há avaliações
- Functional Anatomy of Temporomandibular JointDocumento46 páginasFunctional Anatomy of Temporomandibular JointSiddharth Sharma100% (2)
- Mandibular MovementsDocumento114 páginasMandibular Movementsvinayak shukla67% (3)
- TMJ Postgraduate ProgramDocumento8 páginasTMJ Postgraduate ProgramsorcAinda não há avaliações
- TMJ Part 2Documento85 páginasTMJ Part 2Gaurav SharmaAinda não há avaliações
- Functional Anatomy and TMJ PathologyDocumento15 páginasFunctional Anatomy and TMJ PathologyJASPREETKAUR0410100% (1)
- Criteria Optimum Functional OcclusionDocumento48 páginasCriteria Optimum Functional OcclusionMako J CanadianoAinda não há avaliações
- Temporomandibular JointDocumento86 páginasTemporomandibular Jointdrpankajaapaliya100% (2)
- Final PPT Stomatognathic SysDocumento110 páginasFinal PPT Stomatognathic SysDevangana Das100% (2)
- Muscles of Mastication Saurav 2Documento79 páginasMuscles of Mastication Saurav 2FourthMolar.comAinda não há avaliações
- Growth of MaxillaDocumento110 páginasGrowth of Maxillaprincygarg008Ainda não há avaliações
- Determinants of OcclusionDocumento67 páginasDeterminants of Occlusiondrsmriti100% (4)
- Presented By:-Shalini Thakur Guided By: - Dr. T. RamakrishnaDocumento41 páginasPresented By:-Shalini Thakur Guided By: - Dr. T. RamakrishnaShalini Thakur DubeyAinda não há avaliações
- Biology of Orthodontic Tooth MovementsDocumento17 páginasBiology of Orthodontic Tooth MovementsDler RaufAinda não há avaliações
- Occlusal SplintsDocumento101 páginasOcclusal SplintszpatelcapetownAinda não há avaliações
- MRI TMJ TUTORIAL - PpsDocumento22 páginasMRI TMJ TUTORIAL - Ppsguhander100% (1)
- Tempro-Mandibular Joint: - Can Be Classified Anatomically and Functionally A-AnatomicallyDocumento25 páginasTempro-Mandibular Joint: - Can Be Classified Anatomically and Functionally A-AnatomicallySamwel Emad100% (1)
- Management of Open-Bite in Orthodontics: Dr. T.R. Chandrasekaran PG in Orthodontics MadcDocumento92 páginasManagement of Open-Bite in Orthodontics: Dr. T.R. Chandrasekaran PG in Orthodontics MadcAnirban Sarkar100% (3)
- Growth and Development of Maxilla / Orthodontic Courses by Indian Dental AcademyDocumento63 páginasGrowth and Development of Maxilla / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- TM JointDocumento22 páginasTM Jointapi-19916399Ainda não há avaliações
- Muscles of MasticationDocumento50 páginasMuscles of MasticationKaran AroraAinda não há avaliações
- Temporomandibular Joint (TMJ)Documento32 páginasTemporomandibular Joint (TMJ)shubham royalAinda não há avaliações
- Mandibular Movements FinalDocumento111 páginasMandibular Movements FinalVishal Reddy100% (4)
- TMJ Part 4Documento27 páginasTMJ Part 4api-324160601Ainda não há avaliações
- Muscle Physiology / Orthodontic Courses by Indian Dental AcademyDocumento93 páginasMuscle Physiology / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Temporomandibular Disorders and Physical Therapy InterventionsDocumento33 páginasTemporomandibular Disorders and Physical Therapy InterventionsMelinda Anzani Putri100% (2)
- Muscles of Mastication 2Documento80 páginasMuscles of Mastication 2DENTALORG.COMAinda não há avaliações
- Residual Ridge ResorptionDocumento57 páginasResidual Ridge ResorptionPhoebe DavidAinda não há avaliações
- Biomechanics of Temporomandibular JointDocumento87 páginasBiomechanics of Temporomandibular JointseemaAinda não há avaliações
- Enlow's PrincipleDocumento69 páginasEnlow's Principleankita sethi0% (2)
- TMJ DisordersDocumento20 páginasTMJ DisordersREZVANI FARHADAinda não há avaliações
- Occlusion TextbookDocumento45 páginasOcclusion Textbookوا إسلاماه100% (1)
- THE POSTURE-OCCLUSION RELATIONSHIP AND POSTURAL ASSESSEMENT IN DENTAL TREATMENT - Pocket DentistryDocumento29 páginasTHE POSTURE-OCCLUSION RELATIONSHIP AND POSTURAL ASSESSEMENT IN DENTAL TREATMENT - Pocket DentistryPadmini ReddyAinda não há avaliações
- The A Etiology, Diagnosis and Management of Mandibular AsymmetryDocumento9 páginasThe A Etiology, Diagnosis and Management of Mandibular AsymmetryLeonardo LamimAinda não há avaliações
- Gnath OlogyDocumento41 páginasGnath Ologypushpavalli22100% (1)
- Ear Infections: These Include Otitis Externa, Otitis Media, MastoiditisDocumento32 páginasEar Infections: These Include Otitis Externa, Otitis Media, Mastoiditiseugene ugayAinda não há avaliações
- Bahasa Inggris: Taking Vital Sign (Injection)Documento7 páginasBahasa Inggris: Taking Vital Sign (Injection)iyal09Ainda não há avaliações
- Aswathi Haridas 3 YearDocumento24 páginasAswathi Haridas 3 YearLakshmi MuraleedharanAinda não há avaliações
- Sewage Treatment PlantDocumento12 páginasSewage Treatment Plantanuj dhavanAinda não há avaliações
- FACTS: There Is No Cure & Complete: Sustained Remissions Are Rare. Principles of TherapyDocumento12 páginasFACTS: There Is No Cure & Complete: Sustained Remissions Are Rare. Principles of TherapyAzizan HannyAinda não há avaliações
- Morton's NeuromaDocumento8 páginasMorton's Neuromagreencrystal81Ainda não há avaliações
- PsaDocumento4 páginasPsaEddy TubónAinda não há avaliações
- Consort ChecklistDocumento2 páginasConsort ChecklistAyuAnatrieraAinda não há avaliações
- First Aid Cdrrmo 2019Documento373 páginasFirst Aid Cdrrmo 2019fenan sollanoAinda não há avaliações
- Devarajan, Dss DGN ArdsDocumento4 páginasDevarajan, Dss DGN ArdsrantiadrianiAinda não há avaliações
- Anaphylactic ShockDocumento29 páginasAnaphylactic ShockHIND100% (7)
- Essential Fatty Acid Flax EPA ALADocumento7 páginasEssential Fatty Acid Flax EPA ALAlakshmibava100% (1)
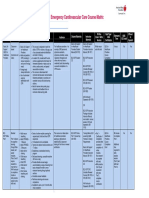
- Emergency Cardiovascular Care Course MatrixDocumento15 páginasEmergency Cardiovascular Care Course MatrixJesus M. Espinosa EchavarriaAinda não há avaliações
- Santos, Ivan Jamil S. NCM 112-Or Rle Fear (Pre-Op) Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocumento1 páginaSantos, Ivan Jamil S. NCM 112-Or Rle Fear (Pre-Op) Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveIvan SantosAinda não há avaliações
- A 3 Table of Surgical Procedures TOSP With Minor Surgical Procedures MSPs 1Documento94 páginasA 3 Table of Surgical Procedures TOSP With Minor Surgical Procedures MSPs 1Chee Yung NgAinda não há avaliações
- The Autism Spectrum Information Booklet: A Guide For Victorian FamiliesDocumento24 páginasThe Autism Spectrum Information Booklet: A Guide For Victorian FamiliesAdriana KincsesAinda não há avaliações
- Dialysis Centre: Assignment - 3Documento12 páginasDialysis Centre: Assignment - 3grvoneandonlyAinda não há avaliações
- Bsn-Stem1a - M7 Post TaskDocumento12 páginasBsn-Stem1a - M7 Post TaskPhoemela Reign GregorioAinda não há avaliações
- Eltroxin (New) TabDocumento8 páginasEltroxin (New) TabhpradeepAinda não há avaliações
- Liangong in 18 Forms PDFDocumento7 páginasLiangong in 18 Forms PDFEzizAinda não há avaliações
- An Assessment of The Breastfeeding Practices and Knowledge Among Mothers in Barangay Camp One, Maramag, BukidnonDocumento35 páginasAn Assessment of The Breastfeeding Practices and Knowledge Among Mothers in Barangay Camp One, Maramag, BukidnonKristine Baldoman CoquillaAinda não há avaliações
- Therapy - Case Study 2Documento7 páginasTherapy - Case Study 2api-239581082100% (1)
- EntDocumento6 páginasEntibrahimAinda não há avaliações
- Adulthood & Geriatric PsychiatryDocumento13 páginasAdulthood & Geriatric PsychiatryPernel Jose Alam MicuboAinda não há avaliações
- Rehydration, Hangover and Vitamin TherapyDocumento2 páginasRehydration, Hangover and Vitamin TherapyKadek SeptiawanAinda não há avaliações
- Self Efficacy Theory - Case StudiesDocumento13 páginasSelf Efficacy Theory - Case StudiesPetros Akin-Nibosun0% (1)
- Hemophilic ArthropathyDocumento2 páginasHemophilic ArthropathyKimmybee GarciaAinda não há avaliações
- BMJ j3887 FullDocumento10 páginasBMJ j3887 FullRiri Maisytoh PutriAinda não há avaliações
- Bioremediation of Environmental PollutantsDocumento21 páginasBioremediation of Environmental PollutantsaziskfAinda não há avaliações
- Skin Diseases in Pregnancy: by by Ahmed Elbohoty MD, MRCOG Lecturer of Obstetrics and Gynecology Ain Shams UniversityDocumento63 páginasSkin Diseases in Pregnancy: by by Ahmed Elbohoty MD, MRCOG Lecturer of Obstetrics and Gynecology Ain Shams UniversityAhmed Bassett100% (1)