Você também pode gostar
- Safety Bulletin Vol 1 Issue 02 Draftl 2Documento4 páginasSafety Bulletin Vol 1 Issue 02 Draftl 2api-185453632Ainda não há avaliações
- Near Miss - OCIMF Definition: Working AloftDocumento10 páginasNear Miss - OCIMF Definition: Working AloftНина РыбкинаAinda não há avaliações
- IMCASF- Aug 19 (2)Documento6 páginasIMCASF- Aug 19 (2)Shivkumar JadhavAinda não há avaliações
- MARS 230 December 2011Documento4 páginasMARS 230 December 2011captkcAinda não há avaliações
- Lesson Learnt - Rev-New2022Documento64 páginasLesson Learnt - Rev-New2022Jan Raver SevaAinda não há avaliações
- Mock Drill - EMERGENCY TOWINGDocumento4 páginasMock Drill - EMERGENCY TOWINGsaurav naskarAinda não há avaliações
- Anchor Loss in Heavy Weather: Learn from IncidentsDocumento4 páginasAnchor Loss in Heavy Weather: Learn from IncidentsJivanJyotiRout100% (1)
- CompleteDocumento35 páginasCompleteJay JayAinda não há avaliações
- SF-16-22Documento6 páginasSF-16-22Shivkumar JadhavAinda não há avaliações
- Imcasf 10 18Documento6 páginasImcasf 10 18Shola EshoAinda não há avaliações
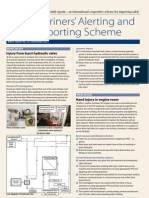
- Mariners' Alerting and Reporting Scheme: Injury From Burst Hydraulic ValveDocumento4 páginasMariners' Alerting and Reporting Scheme: Injury From Burst Hydraulic ValveCostasKAinda não há avaliações
- A Master's Guide To Berthing 2nd EditionDocumento40 páginasA Master's Guide To Berthing 2nd Editionanil.rai67% (3)
- Jhon Raniel Acosta. Bsmt-Port Iii Marlaw Final Exam - : Human FactorDocumento7 páginasJhon Raniel Acosta. Bsmt-Port Iii Marlaw Final Exam - : Human FactorRnl AcstAinda não há avaliações
- Imcasf21 18Documento6 páginasImcasf21 18Era ErmerraAinda não há avaliações
- Avoiding Death on ShipsDocumento9 páginasAvoiding Death on ShipsSubbu JsrAinda não há avaliações
- SF-07-22Documento6 páginasSF-07-22Shivkumar JadhavAinda não há avaliações
- How to Prevent Your Ship from Dragging AnchorDocumento9 páginasHow to Prevent Your Ship from Dragging AnchorGAMMA FACULTY100% (1)
- A Master's Guide To Berthing (2ndedition)Documento40 páginasA Master's Guide To Berthing (2ndedition)ldaels50% (2)
- Ship To Ship (STS) Transfer of Cargo: Latest Developments and Operational Risk AssessmentDocumento24 páginasShip To Ship (STS) Transfer of Cargo: Latest Developments and Operational Risk AssessmentAnjaana PrashantAinda não há avaliações
- IMCASF- Mar 18 (2)Documento5 páginasIMCASF- Mar 18 (2)Shivkumar JadhavAinda não há avaliações
- Ship To Ship (STS) Transfer of Cargo: Latest Developments and Operational Risk AssessmentDocumento24 páginasShip To Ship (STS) Transfer of Cargo: Latest Developments and Operational Risk Assessmentqualiman1100% (1)
- Ship Collision ResponseDocumento14 páginasShip Collision ResponseMukhlis Nugraha100% (1)
- SPL Ebook 021010Documento113 páginasSPL Ebook 021010Mehmet KaptanAinda não há avaliações
- Part 6 TowageDocumento2 páginasPart 6 Towageaungthein_sanAinda não há avaliações
- Risk Watch - Vol 19 No 2 - Jun 2012 PDFDocumento8 páginasRisk Watch - Vol 19 No 2 - Jun 2012 PDFkahl983100% (1)
- IMCA Safety Flash 09/19Documento4 páginasIMCA Safety Flash 09/19Harman SandhuAinda não há avaliações
- MARS209 - Freewater in CargoDocumento4 páginasMARS209 - Freewater in Cargoc rkAinda não há avaliações
- Risk Watch Vol 09 2 PDFDocumento4 páginasRisk Watch Vol 09 2 PDFkahl983Ainda não há avaliações
- Master's Guide to Safe BerthingDocumento42 páginasMaster's Guide to Safe BerthingErsin SaltAinda não há avaliações
- SF-08-22Documento6 páginasSF-08-22Shivkumar JadhavAinda não há avaliações
- IMCA Safety Flash 19/20: 1 Fall From A Height Into A Ballast TankDocumento6 páginasIMCA Safety Flash 19/20: 1 Fall From A Height Into A Ballast TankGianluca PiccinettiAinda não há avaliações
- NTM 158 Fujairah SPM TerminalsDocumento62 páginasNTM 158 Fujairah SPM TerminalsJohn Green100% (1)
- Risk Assessment No 01 ANCHOR HANDLING IN GENERAL Rev 03Documento5 páginasRisk Assessment No 01 ANCHOR HANDLING IN GENERAL Rev 03Devi Ratna Pratiwi78% (9)
- Bridge WatchKeeping EmergenciesDocumento15 páginasBridge WatchKeeping EmergenciesBehendu PereraAinda não há avaliações
- Capt Swaroop Final Notes MergedDocumento77 páginasCapt Swaroop Final Notes Mergedaman kumar100% (1)
- Oral 3Documento38 páginasOral 3Mandy Conquers100% (8)
- IMCASF- Dec 17 (2)Documento6 páginasIMCASF- Dec 17 (2)Shivkumar JadhavAinda não há avaliações
- Lessons Learned Towing AccedentDocumento2 páginasLessons Learned Towing AccedenthgmAinda não há avaliações
- 152 Lesson To Be Learnt 20-2017Documento3 páginas152 Lesson To Be Learnt 20-2017Stevian RakkaAinda não há avaliações
- IMCASF- July 19 (1)Documento5 páginasIMCASF- July 19 (1)Shivkumar JadhavAinda não há avaliações
- Guidance Mooring Safe Way PDFDocumento88 páginasGuidance Mooring Safe Way PDFdivan semestaAinda não há avaliações
- IMCASF- Oct 20 (2)Documento6 páginasIMCASF- Oct 20 (2)Shivkumar JadhavAinda não há avaliações
- Major Accidents On ShipsDocumento61 páginasMajor Accidents On ShipsGonçalo Cruzeiro100% (1)
- RONDocumento7 páginasRONRonnel Ganuelas100% (1)
- Actions To Be Taken Following A CollisionDocumento37 páginasActions To Be Taken Following A CollisionSalvador Jr. Besares100% (5)
- Safety and Hazardous MaterialsDocumento34 páginasSafety and Hazardous MaterialsSATISH PAWARAinda não há avaliações
- INSTRUCTIONAL MATERIALS-PPT- DL.pptx.pdf-1687309099.INSTRUCTIONAL MATERIALS-PPT- DL.pptxDocumento220 páginasINSTRUCTIONAL MATERIALS-PPT- DL.pptx.pdf-1687309099.INSTRUCTIONAL MATERIALS-PPT- DL.pptxKervs LegaspiAinda não há avaliações
- As-2019-021 Collision While Drifting at AnchorageDocumento4 páginasAs-2019-021 Collision While Drifting at Anchoragejude pereiraAinda não há avaliações
- SF-16-23Documento6 páginasSF-16-23Shivkumar JadhavAinda não há avaliações
- DokumenDocumento9 páginasDokumenEdo kurniafenAinda não há avaliações
- Questions for the Rank of Officer of the WatchDocumento57 páginasQuestions for the Rank of Officer of the WatchHoài Thanh100% (4)
- Gard Heavy Weather GuidanceDocumento2 páginasGard Heavy Weather GuidanceGAMMA FACULTYAinda não há avaliações
- Crisis ManagementDocumento14 páginasCrisis ManagementJayesh SolaskarAinda não há avaliações
- Fatal Accident Involving A Flexible HoseDocumento1 páginaFatal Accident Involving A Flexible HoseMohammedAinda não há avaliações
- What Makes Mooring Operation Dangerous?Documento4 páginasWhat Makes Mooring Operation Dangerous?Mayura RanatungaAinda não há avaliações
- Piloting, Seamanship and Small Boat Handling - Vol. VNo EverandPiloting, Seamanship and Small Boat Handling - Vol. VNota: 5 de 5 estrelas5/5 (2)
- Confident Powerboating: Mastering Skills and Avoiding Troubles AfloatNo EverandConfident Powerboating: Mastering Skills and Avoiding Troubles AfloatAinda não há avaliações
- Human ElementDocumento66 páginasHuman Elementapi-185453632100% (1)
- Safety Bulletin Vol 1 Issue 05Documento6 páginasSafety Bulletin Vol 1 Issue 05api-185453632Ainda não há avaliações
- Safety Bulletin Vol 1 Issue 04Documento4 páginasSafety Bulletin Vol 1 Issue 04api-185453632Ainda não há avaliações
- Maritime Safety Conference SummaryDocumento5 páginasMaritime Safety Conference Summaryapi-185453632Ainda não há avaliações
- Safety Bulletin Vol 1 Issue 01 FinalDocumento4 páginasSafety Bulletin Vol 1 Issue 01 Finalapi-185453632Ainda não há avaliações
- Nu-Calgon Product Bulletin: Emkarate RL LubricantsDocumento4 páginasNu-Calgon Product Bulletin: Emkarate RL Lubricantsusna1970Ainda não há avaliações
- Acd175 SeriesDocumento8 páginasAcd175 SeriesRobertoSoaresAinda não há avaliações
- Amm - 12 12 29 611 001 ADocumento7 páginasAmm - 12 12 29 611 001 Araiday84100% (1)
- XM Overspeed Dectictio SolutionDocumento3 páginasXM Overspeed Dectictio SolutionrahmansetiawanAinda não há avaliações
- Introduction To DrillingDocumento25 páginasIntroduction To Drillingrobin2806100% (1)
- Manual Centrifuga UniversalDocumento35 páginasManual Centrifuga Universallebiatan89Ainda não há avaliações
- Gas SystemDocumento6 páginasGas SystemMohammed SayeeduddinAinda não há avaliações
- 2005 Air Emission Inventory for Puget Sound CountiesDocumento223 páginas2005 Air Emission Inventory for Puget Sound Countieswicca9brAinda não há avaliações
- Understanding the Futtsu LNG Thermal Power StationDocumento49 páginasUnderstanding the Futtsu LNG Thermal Power StationJericho CruzAinda não há avaliações
- MIS Lab Practice ExercisesDocumento5 páginasMIS Lab Practice ExercisesKushal DeyAinda não há avaliações
- Detailed Project Report For Pollution 26-12-17Documento11 páginasDetailed Project Report For Pollution 26-12-17NAVKAR PUNEAinda não há avaliações
- Drilling Rig Components and OperationsDocumento67 páginasDrilling Rig Components and OperationsMohamed Kamal100% (1)
- Batteries and Fuel CellsDocumento15 páginasBatteries and Fuel CellsZulvana Anggraeni HarvianAinda não há avaliações
- M1 - Djonrae N. GalvezDocumento5 páginasM1 - Djonrae N. GalvezDjonraeNarioGalvezAinda não há avaliações
- TX842 PDFDocumento2 páginasTX842 PDFDian SikumbangAinda não há avaliações
- 368kW (500mhp) : First Class Power - The Yanmar 6HYDocumento2 páginas368kW (500mhp) : First Class Power - The Yanmar 6HYRudy PriatnaAinda não há avaliações
- Do Lower Speed Limits On Motorways Reduce Fuel Consumption and Pollutant Emissions - European Environment Agency (EEA)Documento8 páginasDo Lower Speed Limits On Motorways Reduce Fuel Consumption and Pollutant Emissions - European Environment Agency (EEA)saospieAinda não há avaliações
- TM2500 BrochureDocumento8 páginasTM2500 BrochuregustiramadaniAinda não há avaliações
- EPS Employment Application FormDocumento10 páginasEPS Employment Application FormLiviu Crăciun50% (2)
- Fired Heater LectureDocumento28 páginasFired Heater LectureDylanAdams100% (1)
- Paper 1 - Set B Solutions: General InstructionsDocumento16 páginasPaper 1 - Set B Solutions: General InstructionsMukesh KumarAinda não há avaliações
- 2010 - Desulfurization of Diesel Fuels by Selective Adsorption On Activated CarbonsDocumento11 páginas2010 - Desulfurization of Diesel Fuels by Selective Adsorption On Activated CarbonsloremncAinda não há avaliações
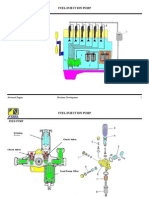
- Fuel Injection Pump Guide: Types, Components & Working PrinciplesDocumento9 páginasFuel Injection Pump Guide: Types, Components & Working PrinciplesJoko Sukariono100% (2)
- KICK ToleranceDocumento16 páginasKICK ToleranceIshtiaq Khalid100% (1)
- Wärtsilä 50DF dual-fuel engines promise big benefits for LNG carriersDocumento2 páginasWärtsilä 50DF dual-fuel engines promise big benefits for LNG carriersbernardinodinoAinda não há avaliações
- Hydraulic Fracturing Fluid DisclosureDocumento17 páginasHydraulic Fracturing Fluid Disclosurejangri1098Ainda não há avaliações
- 750-208 OM Profire-S1 Jan09Documento72 páginas750-208 OM Profire-S1 Jan09fauzi endraAinda não há avaliações
- Piping Design PresentationDocumento40 páginasPiping Design PresentationArun Zac100% (2)
- EFI-SystemDocumento35 páginasEFI-SystemShrvan Hirde100% (2)
- Fundamentals of Refining and Petrochemicals ProcessesDocumento263 páginasFundamentals of Refining and Petrochemicals ProcessesneocentricgeniusAinda não há avaliações