Você também pode gostar
- Letter of Author Is at IonDocumento1 páginaLetter of Author Is at IonmannymansorAinda não há avaliações
- LetterAuthHealthRecordsDocumento1 páginaLetterAuthHealthRecordsAngelito Motas PobleteAinda não há avaliações
- Cancellation of Removal for Lawful Permanent ResidentsNo EverandCancellation of Removal for Lawful Permanent ResidentsAinda não há avaliações
- Letter of AuthorizationDocumento1 páginaLetter of Authorizationtwinkle123456Ainda não há avaliações
- A Guide to District Court Civil Forms in the State of HawaiiNo EverandA Guide to District Court Civil Forms in the State of HawaiiAinda não há avaliações
- HAAD Letter of AuthorizationDocumento1 páginaHAAD Letter of AuthorizationRenny M PAinda não há avaliações
- California Notary Public Study Guide with 7 Practice Exams: 280 Practice Questions and 100+ Bonus Questions IncludedNo EverandCalifornia Notary Public Study Guide with 7 Practice Exams: 280 Practice Questions and 100+ Bonus Questions IncludedAinda não há avaliações
- Letter of Authorization: - Signature Date (Dd/mm/yyyy)Documento1 páginaLetter of Authorization: - Signature Date (Dd/mm/yyyy)Alyssa Bella DugayAinda não há avaliações
- November 20, 2016 To Whom It May ConcernDocumento1 páginaNovember 20, 2016 To Whom It May ConcernGayLah MomblancoAinda não há avaliações
- Motions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsNo EverandMotions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsNota: 4.5 de 5 estrelas4.5/5 (13)
- Overseas Post GraduateDocumento9 páginasOverseas Post GraduateKashif AzizAinda não há avaliações
- Letter Authorization for Background CheckDocumento1 páginaLetter Authorization for Background CheckMrunal DoiphodeAinda não há avaliações
- Data Flow Application Form 2020Documento5 páginasData Flow Application Form 2020Chelsa RetutaAinda não há avaliações
- DataFlow Application PackDocumento8 páginasDataFlow Application PackvaranasidineshAinda não há avaliações
- Letter of Authorization اﻟ ﺗ ﻔ و ﯾ ض ﺧ ط ﺎ بDocumento1 páginaLetter of Authorization اﻟ ﺗ ﻔ و ﯾ ض ﺧ ط ﺎ بBALAJI VENKITESANAinda não há avaliações
- Candidate Declaration FormDocumento2 páginasCandidate Declaration Formaslam810Ainda não há avaliações
- Letter Authorization ConfirmationDocumento1 páginaLetter Authorization Confirmationjoni_joanAinda não há avaliações
- Letter Authorization ConfirmationDocumento1 páginaLetter Authorization ConfirmationJojo LuceroAinda não há avaliações
- Verify credentials program Saudi CommissionDocumento1 páginaVerify credentials program Saudi CommissionMildred Cinense BurlazaAinda não há avaliações
- Letter of Authorization ﺾﻳﻮﻔﺘﻟا بﺎﻄﺧDocumento1 páginaLetter of Authorization ﺾﻳﻮﻔﺘﻟا بﺎﻄﺧCopy World - Work Al NasarAinda não há avaliações
- Schs Loa UpdatedDocumento1 páginaSchs Loa UpdatedV.VAinda não há avaliações
- To Whom So Ever It May Concern': Authorization NoteDocumento1 páginaTo Whom So Ever It May Concern': Authorization NoteAbhishek ShuklaAinda não há avaliações
- DataFlow Application PackDocumento8 páginasDataFlow Application PackMichelle TolentinoAinda não há avaliações
- Authorization Letterity IntelligenceDocumento1 páginaAuthorization Letterity Intelligencekancil121Ainda não há avaliações
- Academic and Employment Verifications - GeneralDocumento4 páginasAcademic and Employment Verifications - GeneralGeorge WangAinda não há avaliações
- BGV Authorization Letter PDFDocumento1 páginaBGV Authorization Letter PDFDevaraj kashyap0% (2)
- General Global Consent FormDocumento2 páginasGeneral Global Consent Formbc210411250 BISMA BIBIAinda não há avaliações
- Letter of Authorization for Background CheckDocumento1 páginaLetter of Authorization for Background Checkshashank pandeyAinda não há avaliações
- CTOS Consent LettersDocumento1 páginaCTOS Consent LettersKAR ENG QUAHAinda não há avaliações
- To Whom So Ever It May Concern': Authorization NoteDocumento1 páginaTo Whom So Ever It May Concern': Authorization NoteAbhishek SharmaAinda não há avaliações
- Letter of AuthorizationDocumento1 páginaLetter of Authorizationshreya arunAinda não há avaliações
- Consent FormDocumento3 páginasConsent FormMarilou AgustinAinda não há avaliações
- Consent FormDocumento3 páginasConsent FormMarilou AgustinAinda não há avaliações
- ECFMG Certification Identification FormDocumento2 páginasECFMG Certification Identification FormUsama BilalAinda não há avaliações
- Cissp Release FormDocumento1 páginaCissp Release FormAnonymous 9d1jFvAinda não há avaliações
- Client and Applicant Instructions CanadaDocumento4 páginasClient and Applicant Instructions CanadaGeorge WangAinda não há avaliações
- Sher Singh 703763 AuthorizationLetterforBackgroundVerification 20221010 130828 A6343cbf490882Documento2 páginasSher Singh 703763 AuthorizationLetterforBackgroundVerification 20221010 130828 A6343cbf490882Sher Singh ThakurAinda não há avaliações
- LOA - Pre - Employment VerificationDocumento1 páginaLOA - Pre - Employment VerificationlakshAinda não há avaliações
- Verification Form - Health Authority Abu DhabiDocumento6 páginasVerification Form - Health Authority Abu DhabiElaine Iris AbastaAinda não há avaliações
- 03.1a WQ BRAIN Personal Statement & Dislosure Authorization (RU-IN-IL-MY-ID-TH-TW-SK-VN)Documento2 páginas03.1a WQ BRAIN Personal Statement & Dislosure Authorization (RU-IN-IL-MY-ID-TH-TW-SK-VN)Trương Thành ThảoAinda não há avaliações
- Instructions - Please Follow Carefully! Affidavit & Release Form and Certification of Identification Form 1. Affidavit and ReleaseDocumento4 páginasInstructions - Please Follow Carefully! Affidavit & Release Form and Certification of Identification Form 1. Affidavit and ReleaseJohnnyLarsonAinda não há avaliações
- Background Check Disclosure and AuthorizationDocumento1 páginaBackground Check Disclosure and Authorizationaravind manneAinda não há avaliações
- KPMGDocumento1 páginaKPMGlaxmank5534Ainda não há avaliações
- Out-of-State Credential VerificationDocumento1 páginaOut-of-State Credential VerificationChristopher VũAinda não há avaliações
- Letter of AuthorisationDocumento2 páginasLetter of Authorisationharishr2494Ainda não há avaliações
- Fm-Ro-88-00 - Proof of Residency UnvaccinationDocumento1 páginaFm-Ro-88-00 - Proof of Residency UnvaccinationJc AustriaAinda não há avaliações
- Pharmacist Application EvaluationDocumento0 páginaPharmacist Application EvaluationDr-Usman KhanAinda não há avaliações
- Articles Checklist Duration of Service Under ArticlesDocumento17 páginasArticles Checklist Duration of Service Under ArticlesSizweAinda não há avaliações
- DownloadDocumento2 páginasDownloadEsteban TorresAinda não há avaliações
- PEBC Application Pharmacist Document EvaluationDocumento2 páginasPEBC Application Pharmacist Document EvaluationmcarthooAinda não há avaliações
- Authorization FormDocumento1 páginaAuthorization FormVishnu VardhanAinda não há avaliações
- Authorization FormDocumento1 páginaAuthorization FormakashAinda não há avaliações
- Attestation Form For Educational Credentials Review or Type 1 Review ServiceDocumento1 páginaAttestation Form For Educational Credentials Review or Type 1 Review ServiceAudrey BoAinda não há avaliações
- VSSI LOA-Consent Fom (2020)Documento1 páginaVSSI LOA-Consent Fom (2020)Ponching OriosteAinda não há avaliações
- Consent FormDocumento2 páginasConsent FormManish KumarAinda não há avaliações
- Background Check DisclosureDocumento1 páginaBackground Check DisclosureAccurate Public Records, LLCAinda não há avaliações
- Consent To Background CheckDocumento1 páginaConsent To Background CheckYsabel JavierAinda não há avaliações
- STUDENT LINKING WORDS AND PHRASESDocumento6 páginasSTUDENT LINKING WORDS AND PHRASESEdward YooAinda não há avaliações
- IELTS Writing Answer SheetDocumento4 páginasIELTS Writing Answer SheetHighPoint IELTS Preparation Services, Inc.Ainda não há avaliações
- Essay Question 1 - Outsourcing Labour Related Work To Poorer Nations - Corrected by RyanDocumento5 páginasEssay Question 1 - Outsourcing Labour Related Work To Poorer Nations - Corrected by RyanDr-Usman Khan0% (1)
- TransitionsDocumento3 páginasTransitionsDr-Usman KhanAinda não há avaliações
- IELTS Speaking Part 1 VocabularyDocumento24 páginasIELTS Speaking Part 1 VocabularyDr-Usman Khan100% (1)
- Nol 7zone Eng PDFDocumento1 páginaNol 7zone Eng PDFneedzinAinda não há avaliações
- YES-IELTS - Decoding The IELTS Band Descriptors - Writing Task 2 - Task Response - Bands 6, 7, 8, 9Documento6 páginasYES-IELTS - Decoding The IELTS Band Descriptors - Writing Task 2 - Task Response - Bands 6, 7, 8, 9YES IELTS100% (2)
- IELTS True False Not GivenDocumento5 páginasIELTS True False Not GivenDr-Usman Khan100% (2)
- Difference BTW False, No, NGDocumento1 páginaDifference BTW False, No, NGDr-Usman KhanAinda não há avaliações
- Speaking Tips by RyanDocumento2 páginasSpeaking Tips by RyanDr-Usman Khan100% (3)
- Connectors For IELTSDocumento24 páginasConnectors For IELTSDr-Usman KhanAinda não há avaliações
- Difference BTW False, No, NGDocumento1 páginaDifference BTW False, No, NGDr-Usman KhanAinda não há avaliações
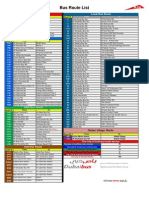
- Bus Route List EnglishDocumento1 páginaBus Route List EnglishDr-Usman KhanAinda não há avaliações
- Bus Route List EnglishDocumento1 páginaBus Route List EnglishDr-Usman KhanAinda não há avaliações
- Exam MaterialsDocumento4 páginasExam MaterialsDr-Usman KhanAinda não há avaliações
- PharmaciesDocumento18 páginasPharmaciesDr-Usman KhanAinda não há avaliações
- 32 Ielts Essay Samples Band 9Documento34 páginas32 Ielts Essay Samples Band 9mh73% (26)
- Delcaration Form by The Sponsoring FacilityDocumento1 páginaDelcaration Form by The Sponsoring FacilityDr-Usman Khan100% (1)
- 06 MarchDocumento3 páginas06 MarchDr-Usman Khan0% (1)
- 23 QsDocumento8 páginas23 QsDr-Usman Khan0% (1)
- 5 2 2014 - 2Documento2 páginas5 2 2014 - 2Dr-Usman Khan100% (1)
- 5 2 2014 - 2Documento2 páginas5 2 2014 - 2Dr-Usman Khan100% (1)
- 570 Academic Word List For IELTSDocumento26 páginas570 Academic Word List For IELTSXanh Lè100% (1)
- 30-01-2014 Test Malik Asif Javaid AwanDocumento4 páginas30-01-2014 Test Malik Asif Javaid AwanDr-Usman Khan67% (3)
- Dha Prometric Feb-3 ShabeerDocumento2 páginasDha Prometric Feb-3 ShabeerDr-Usman KhanAinda não há avaliações
- Writing Task 1 1-8Documento28 páginasWriting Task 1 1-8Dr-Usman KhanAinda não há avaliações
- Dha Prometric Feb-3 ShabeerDocumento2 páginasDha Prometric Feb-3 ShabeerDr-Usman KhanAinda não há avaliações
- DHA Prometric Exam 02-01-2014 Role of Carbidopa in ParkinsonismDocumento4 páginasDHA Prometric Exam 02-01-2014 Role of Carbidopa in ParkinsonismDr-Usman Khan79% (14)
- Good CommunicationDocumento6 páginasGood CommunicationKranthi KumarAinda não há avaliações
- The Drugs Act, 1976Documento32 páginasThe Drugs Act, 1976Dr-Usman KhanAinda não há avaliações