Você também pode gostar
- Neurological Assessment in the First Two Years of LifeNo EverandNeurological Assessment in the First Two Years of LifeGiovanni CioniAinda não há avaliações
- Occupation Analysis in PracticeNo EverandOccupation Analysis in PracticeLynette MackenzieAinda não há avaliações
- Chapter 8Documento30 páginasChapter 8Karla CarazoAinda não há avaliações
- The Sensory Integration and Praxis Tests: Illuminating Struggles and Strengths in Participation at SchoolDocumento7 páginasThe Sensory Integration and Praxis Tests: Illuminating Struggles and Strengths in Participation at SchoolChristofer Josue Muñoz ArancibiaAinda não há avaliações
- Peabody y Movent ABCDocumento11 páginasPeabody y Movent ABCIngrid BarkoAinda não há avaliações
- Activity Monitoring WorksheetDocumento2 páginasActivity Monitoring WorksheetRoberto SzenczukAinda não há avaliações
- General Self-Efficacy Scale (GSE)Documento2 páginasGeneral Self-Efficacy Scale (GSE)Angelus MoreAinda não há avaliações
- BOTMP2Documento31 páginasBOTMP2蘇永泓Ainda não há avaliações
- Uniform Terminology AOTA PDFDocumento8 páginasUniform Terminology AOTA PDFLaura GuevaraAinda não há avaliações
- Occupational Therapy and Life Course Development: A Work Book for Professional PracticeNo EverandOccupational Therapy and Life Course Development: A Work Book for Professional PracticeAinda não há avaliações
- Otor & Visual Motor AssessDocumento4 páginasOtor & Visual Motor AssessBea FloresAinda não há avaliações
- OT Practice August 6 IssueDocumento19 páginasOT Practice August 6 IssueThe American Occupational Therapy AssociationAinda não há avaliações
- OT Appendix Tables-Mar.2006Documento12 páginasOT Appendix Tables-Mar.2006Yas DGAinda não há avaliações
- Sfa Scool Function AssementDocumento18 páginasSfa Scool Function AssementAnielle OliveiraAinda não há avaliações
- Dyssemia Rating ScaleDocumento8 páginasDyssemia Rating ScaleHazardous7Ainda não há avaliações
- OT and Eating DysfunctionDocumento1 páginaOT and Eating DysfunctionMCris EsSemAinda não há avaliações
- PT GoalsDocumento13 páginasPT Goalsnaomi harowAinda não há avaliações
- SP Recommendation and StrategiesDocumento18 páginasSP Recommendation and StrategiesFerrisAinda não há avaliações
- GmfmscoresheetDocumento6 páginasGmfmscoresheetapi-260049180Ainda não há avaliações
- Ot Guidelines Child SpecificDocumento34 páginasOt Guidelines Child Specific健康生活園Healthy Life Garden100% (1)
- Yerxa - Health and The Human Spirit For Occupation.Documento7 páginasYerxa - Health and The Human Spirit For Occupation.Shant KhatchikAinda não há avaliações
- Rheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementNo EverandRheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementLynne GoodacreAinda não há avaliações
- Occupational Therapy Assessment ToolsDocumento19 páginasOccupational Therapy Assessment ToolsThirdy BullerAinda não há avaliações
- Evaluation ReportDocumento3 páginasEvaluation Reportapi-547360536Ainda não há avaliações
- Occupation Centred Practice with Children: A Practical Guide for Occupational TherapistsNo EverandOccupation Centred Practice with Children: A Practical Guide for Occupational TherapistsAinda não há avaliações
- MFUNDocumento22 páginasMFUNRachelle RoseAinda não há avaliações
- Occupational Therapy: Sarah NewellDocumento14 páginasOccupational Therapy: Sarah NewellGabriella ALeAinda não há avaliações
- School BasedOccupationalTherapyduringCOVID 19Documento12 páginasSchool BasedOccupationalTherapyduringCOVID 19Ligia SendreaAinda não há avaliações
- The Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionNo EverandThe Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionAinda não há avaliações
- Pedi Cat ManualDocumento163 páginasPedi Cat ManualJosh Provlin100% (1)
- Fine Motor Precision CompressDocumento17 páginasFine Motor Precision CompressVictor Bravo OlivaresAinda não há avaliações
- CO-OP PediatriaDocumento17 páginasCO-OP PediatriaCarol Alvarado100% (2)
- Allen Cognitive Level ScreenDocumento9 páginasAllen Cognitive Level ScreenIntan Indah Sari100% (2)
- Evaluation and Intervention PlanningDocumento13 páginasEvaluation and Intervention PlanningAnup Pednekar100% (1)
- The Movment ABC Template For Evaluations AB-2 7-10 YearsDocumento2 páginasThe Movment ABC Template For Evaluations AB-2 7-10 YearsFerris100% (1)
- School Function AssessmentDocumento8 páginasSchool Function AssessmentPaulina Vergara67% (3)
- Sensory ReactivityDocumento19 páginasSensory ReactivitySebastian Pinto ReyesAinda não há avaliações
- Ampsmanual Chapters1-4Documento52 páginasAmpsmanual Chapters1-4Aymen DabboussiAinda não há avaliações
- SI Theory and PracticeDocumento57 páginasSI Theory and PracticeMaria Laura Soria100% (1)
- Perkins Activity and Resource Guide Chapter 2 - Foundations of Learning Language, Cognition, and Social Relationships: Second Edition: Revised and UpdatedNo EverandPerkins Activity and Resource Guide Chapter 2 - Foundations of Learning Language, Cognition, and Social Relationships: Second Edition: Revised and UpdatedAinda não há avaliações
- How To Create A Successful, No-Stress Sensory Diet For Kids WorkbookDocumento4 páginasHow To Create A Successful, No-Stress Sensory Diet For Kids WorkbookAdriana NegrescuAinda não há avaliações
- CLASI Intervention Course NotesDocumento241 páginasCLASI Intervention Course Notessaskia.bouwer100% (1)
- Mohost v2 0 Uk Multiple SummariesDocumento2 páginasMohost v2 0 Uk Multiple SummariesAngela EnacheAinda não há avaliações
- Canadian Occupational Performance Measure (COPM) : 4 EditionDocumento3 páginasCanadian Occupational Performance Measure (COPM) : 4 EditionDulcea LoredanaAinda não há avaliações
- Model of Human Occupation Parts 1-4Documento36 páginasModel of Human Occupation Parts 1-4Alice GiffordAinda não há avaliações
- Spinal Cord Assesment Form PTDocumento8 páginasSpinal Cord Assesment Form PTSureaka PonnusamyAinda não há avaliações
- Sensory Integration Inventory ItemiDocumento4 páginasSensory Integration Inventory Itemidragomir_emilia92Ainda não há avaliações
- Satco Clinical WorkbookDocumento6 páginasSatco Clinical WorkbookKidz to Adultz Exhibitions100% (1)
- Work and Occupational TherapyDocumento31 páginasWork and Occupational Therapysmith197077Ainda não há avaliações
- Sensory DietDocumento4 páginasSensory Dietapi-571361183Ainda não há avaliações
- Visual Motor Integration WebinarDocumento5 páginasVisual Motor Integration WebinarAnonymous QqyLDoW1100% (1)
- A Review of Pediatric Assessment Tools For Sensory Integration AOTADocumento3 páginasA Review of Pediatric Assessment Tools For Sensory Integration AOTAhelenzhang888Ainda não há avaliações
- The Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityDocumento7 páginasThe Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityIJAR JOURNALAinda não há avaliações
- Guidelines Down Syndrome Assessment and Intervention PDFDocumento292 páginasGuidelines Down Syndrome Assessment and Intervention PDFZenithaMeidaAinda não há avaliações
- 102 Occupational Therapy For Physical DysfunctionDocumento61 páginas102 Occupational Therapy For Physical DysfunctionPatricia MiglesAinda não há avaliações
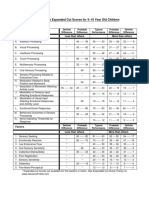
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDocumento1 páginaSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliAinda não há avaliações
- Sensory Processing Measure (SPM) - Pearson Clinical Australia & New ZealandDocumento1 páginaSensory Processing Measure (SPM) - Pearson Clinical Australia & New ZealandVINEET GAIROLA0% (1)
- Chan v. ChanDocumento2 páginasChan v. ChanjdpajarilloAinda não há avaliações
- ODocumento11 páginasOMihaela CherejiAinda não há avaliações
- Rediscovering Alginate Wound DressingsDocumento4 páginasRediscovering Alginate Wound DressingstanveerhusseinAinda não há avaliações
- Compensation ManagementDocumento2 páginasCompensation Managementshreekumar_scdlAinda não há avaliações
- Ammonia Synthesis ConverterDocumento26 páginasAmmonia Synthesis ConverterKvspavan Kumar100% (1)
- PTS 18.52.08Documento60 páginasPTS 18.52.08azrai danialAinda não há avaliações
- Fomula Spreadsheet (WACC and NPV)Documento7 páginasFomula Spreadsheet (WACC and NPV)vaishusonu90Ainda não há avaliações
- Citizen's 8651 Manual PDFDocumento16 páginasCitizen's 8651 Manual PDFtfriebusAinda não há avaliações
- Calculation Condensation StudentDocumento7 páginasCalculation Condensation StudentHans PeterAinda não há avaliações
- Signage Method of Statement and Risk AssessmentDocumento3 páginasSignage Method of Statement and Risk AssessmentNajmal AmanAinda não há avaliações
- Fittings: Fitting Buying GuideDocumento2 páginasFittings: Fitting Buying GuideAaron FonsecaAinda não há avaliações
- Lesson 2 Basic Osah, General Provisions, Safety Rules..Documento30 páginasLesson 2 Basic Osah, General Provisions, Safety Rules..GM VispoAinda não há avaliações
- Group 7 Worksheet No. 1 2Documento24 páginasGroup 7 Worksheet No. 1 2calliemozartAinda não há avaliações
- Mobil Delvac 1 ESP 5W-40Documento3 páginasMobil Delvac 1 ESP 5W-40RachitAinda não há avaliações
- ICSE Class 10 HRJUDSK/Question Paper 2020: (Two Hours)Documento9 páginasICSE Class 10 HRJUDSK/Question Paper 2020: (Two Hours)Harshu KAinda não há avaliações
- To 33B-1-1 01jan2013Documento856 páginasTo 33B-1-1 01jan2013izmitlimonAinda não há avaliações
- #1 - The World'S Oldest First GraderDocumento6 páginas#1 - The World'S Oldest First GraderTran Van ThanhAinda não há avaliações
- The Chemical Composition and Organoleptic Attributes of Lesser-Known Vegetables As Consumed in Njikoka Local Government Area, Anambra State, NigeriaDocumento4 páginasThe Chemical Composition and Organoleptic Attributes of Lesser-Known Vegetables As Consumed in Njikoka Local Government Area, Anambra State, NigeriaEmri CynthiaAinda não há avaliações
- Analyzing Activity and Injury: Lessons Learned From The Acute:Chronic Workload RatioDocumento12 páginasAnalyzing Activity and Injury: Lessons Learned From The Acute:Chronic Workload RatioLukas ArenasAinda não há avaliações
- Just Another RantDocumento6 páginasJust Another RantJuan Manuel VargasAinda não há avaliações
- Product Sheet - Parsys Cloud - Parsys TelemedicineDocumento10 páginasProduct Sheet - Parsys Cloud - Parsys TelemedicineChristian Lezama Cuellar100% (1)
- II092 - Horiz & Vert ULSs With Serial InputsDocumento4 páginasII092 - Horiz & Vert ULSs With Serial InputsJibjab7Ainda não há avaliações
- Select Event Venue and SiteDocumento11 páginasSelect Event Venue and SiteLloyd Arnold Catabona100% (1)
- Harmonized Household Profiling ToolDocumento2 páginasHarmonized Household Profiling ToolJessa Mae89% (9)
- Drug Development: New Chemical Entity DevelopmentDocumento6 páginasDrug Development: New Chemical Entity DevelopmentDeenAinda não há avaliações
- Drug AbuseDocumento33 páginasDrug AbuseharshulnmimsAinda não há avaliações
- The Ego and Analysis of Defense-Jason Aronson, Inc. (2005) Paul GrayDocumento356 páginasThe Ego and Analysis of Defense-Jason Aronson, Inc. (2005) Paul GrayClinica MonserratAinda não há avaliações
- EDC MS5 In-Line Injection Pump: Issue 2Documento57 páginasEDC MS5 In-Line Injection Pump: Issue 2Musharraf KhanAinda não há avaliações
- SSN Melaka SMK Seri Kota 2021 Annual Training Plan: Athletes Name Training ObjectivesDocumento2 páginasSSN Melaka SMK Seri Kota 2021 Annual Training Plan: Athletes Name Training Objectivessiapa kahAinda não há avaliações
- Mapeh 9 Aho Q2W1Documento8 páginasMapeh 9 Aho Q2W1Trisha Joy Paine TabucolAinda não há avaliações