Você também pode gostar
- Pathophysiology of NSVDDocumento2 páginasPathophysiology of NSVDLenjun83% (6)
- Pathophysiology of NSDDocumento2 páginasPathophysiology of NSDJNDNNSBM50610% (1)
- Abruptio Placenta PathophysiologyDocumento4 páginasAbruptio Placenta Pathophysiologyjamie carpioAinda não há avaliações
- Pathophysiology For HELLP SyndromeDocumento2 páginasPathophysiology For HELLP SyndromeRosemarie CarpioAinda não há avaliações
- ABORTION PathophysiologyDocumento3 páginasABORTION PathophysiologyChiara FajardoAinda não há avaliações
- Case Study On Intrauterine Fetal Demise (Final Draft)Documento11 páginasCase Study On Intrauterine Fetal Demise (Final Draft)Anne Mosquite82% (11)
- Chapter 24: Nursing Care of A Family During A Surgical Intervention For BirthDocumento22 páginasChapter 24: Nursing Care of A Family During A Surgical Intervention For BirthAlyssaGrandeMontimorAinda não há avaliações
- Iii. Textbook Discussion A. Definition: Predisposing Factors Precipitating FactorsDocumento3 páginasIii. Textbook Discussion A. Definition: Predisposing Factors Precipitating FactorsVianne ArcenioAinda não há avaliações
- Nursing Care of Hydatidiform MoleDocumento23 páginasNursing Care of Hydatidiform MoleKristel Rivamonte100% (1)
- Abnormal Uterine BleedingDocumento19 páginasAbnormal Uterine BleedingDelphy Varghese100% (1)
- REFERAT - Ppt.pathophysiology of PROM-noviDocumento16 páginasREFERAT - Ppt.pathophysiology of PROM-noviFrisma Indah Permatasari100% (1)
- Discharge PlanningDocumento3 páginasDischarge PlanningAlex Marie100% (2)
- Pathophysiology of Ectopic PregnancyDocumento1 páginaPathophysiology of Ectopic PregnancyLiza MinonaAinda não há avaliações
- Anatomy Pathophysiology PreeclampsiaDocumento4 páginasAnatomy Pathophysiology PreeclampsiaKeith Wesley YbutAinda não há avaliações
- Pathophysiology of Hyperemesis Gravidarum DiagramDocumento1 páginaPathophysiology of Hyperemesis Gravidarum DiagramQuintin MangaoangAinda não há avaliações
- Concept of unitive and procreative healthDocumento5 páginasConcept of unitive and procreative healthDONITA DALUMPINESAinda não há avaliações
- Nursing Care Plan AbortionDocumento4 páginasNursing Care Plan AbortionJane Casiquin100% (1)
- Nursing Crib Com NURSING CARE PLAN Spontaneous AbortionDocumento2 páginasNursing Crib Com NURSING CARE PLAN Spontaneous AbortionJustin PasaronAinda não há avaliações
- GENERIC NAME: Co-Amoxiclav (Amoxicillin & Clavulanic Acid) BRAND NAMES: Natravox, AddexDocumento4 páginasGENERIC NAME: Co-Amoxiclav (Amoxicillin & Clavulanic Acid) BRAND NAMES: Natravox, AddexDRAAinda não há avaliações
- Nursing Care of The Client With High-Risk Labor & DeliveryDocumento10 páginasNursing Care of The Client With High-Risk Labor & DeliveryWilbert CabanbanAinda não há avaliações
- PATHOPHYSIOLOGY of ECTOPIC PREGNANCYDocumento2 páginasPATHOPHYSIOLOGY of ECTOPIC PREGNANCYryeAinda não há avaliações
- Nursing Care PlanDocumento3 páginasNursing Care PlanArvan James Cabugayan TalboAinda não há avaliações
- Ectopic Pregnancy Nursing Care PlanDocumento2 páginasEctopic Pregnancy Nursing Care PlanKim GalamgamAinda não há avaliações
- NSVD Case Study FinalDocumento60 páginasNSVD Case Study Finaljints poterAinda não há avaliações
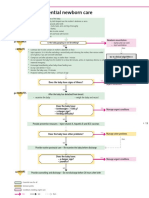
- Essential newborn care steps in first 90 minutesDocumento1 páginaEssential newborn care steps in first 90 minutesGabriel Anthony ArtizaAinda não há avaliações
- Unang Yakap: Essential Newborn Care (ENC) ProtocolDocumento13 páginasUnang Yakap: Essential Newborn Care (ENC) ProtocolJan Oliver YaresAinda não há avaliações
- CPD: Cephalo-Pelvic Disproportion PathophysiologyDocumento3 páginasCPD: Cephalo-Pelvic Disproportion PathophysiologyTeanne Bathan100% (1)
- NCM 109N: Frameworks For Maternal & Child Health NursingDocumento37 páginasNCM 109N: Frameworks For Maternal & Child Health NursingZudotaAinda não há avaliações
- Ectopic Pregnancy PathophysiologyDocumento5 páginasEctopic Pregnancy Pathophysiologyjoyrena ochondraAinda não há avaliações
- Normal Spontaneous Vaginal DeliveryDocumento35 páginasNormal Spontaneous Vaginal DeliveryJohn Edward EscoteAinda não há avaliações
- Placenta Previa PhatoDocumento2 páginasPlacenta Previa PhatoMarl Jarl E BayanesAinda não há avaliações
- Pathophysiology EclampsiaDocumento5 páginasPathophysiology EclampsiaYael EzraAinda não há avaliações
- Maternal Risk AssessmentDocumento3 páginasMaternal Risk AssessmentMark FernandezAinda não há avaliações
- 1 and 11.1 ABDOMINAL LAYERS AND CESAREAN SECTIONDocumento14 páginas1 and 11.1 ABDOMINAL LAYERS AND CESAREAN SECTIONKim Sunoo100% (1)
- Care of Pregnant FamilyDocumento17 páginasCare of Pregnant FamilyKaryll RomeroAinda não há avaliações
- I. Pathophysiology: Fetal Swallowing Renal Disorder of Fetus Premature Rupture of MembraneDocumento3 páginasI. Pathophysiology: Fetal Swallowing Renal Disorder of Fetus Premature Rupture of MembraneSTEFFI GRACE TANAinda não há avaliações
- Case Study On NSVDDocumento50 páginasCase Study On NSVDNyj Quiño100% (2)
- PATHOPHYSIOLOGY - Placenta PreviaDocumento5 páginasPATHOPHYSIOLOGY - Placenta PreviaFretzgine Lou Manuel100% (2)
- Incompetent Cervix Case Analysis Subgroup 2Documento44 páginasIncompetent Cervix Case Analysis Subgroup 2bunso padillaAinda não há avaliações
- Gestational AgeDocumento6 páginasGestational AgemhuniswellAinda não há avaliações
- Retained Placental FragmentsDocumento9 páginasRetained Placental FragmentsHannah Laput100% (2)
- NURSING CARE PLAN ON FOUL-SMELLING LOCHIADocumento3 páginasNURSING CARE PLAN ON FOUL-SMELLING LOCHIANE Tdr100% (1)
- Pathophysiology of Incomplete Abortion: Risk Factors and ManagementDocumento3 páginasPathophysiology of Incomplete Abortion: Risk Factors and ManagementClaire Nimor Ventulan50% (4)
- I. Framework For Maternal and Child Health Nursing (MCN) Focusing On At-Risk, High Risk, and Sick ClientsDocumento5 páginasI. Framework For Maternal and Child Health Nursing (MCN) Focusing On At-Risk, High Risk, and Sick ClientsSophia Loraine Dorone Jesura100% (1)
- Nursing Care Plans: Ineffective (Uteroplacental) Tissue PerfusionDocumento2 páginasNursing Care Plans: Ineffective (Uteroplacental) Tissue PerfusionVincent Paul SantosAinda não há avaliações
- Postpartum Hemorrhage: A.Personal DataDocumento55 páginasPostpartum Hemorrhage: A.Personal DataEmmanuel Recodo100% (1)
- Pathophysiology NSD FinalDocumento2 páginasPathophysiology NSD FinalDaniel Tan Galindez80% (5)
- Case Study (Preeclampsia)Documento6 páginasCase Study (Preeclampsia)Jobelle AcenaAinda não há avaliações
- Drug Study: I Loilo Doctors' College College of NursingDocumento6 páginasDrug Study: I Loilo Doctors' College College of NursingAudrie Allyson GabalesAinda não há avaliações
- Dysfunctional Uterine Bleeding (DUB)Documento1 páginaDysfunctional Uterine Bleeding (DUB)Bheru LalAinda não há avaliações
- Multivitamin with iron relieves deficienciesDocumento3 páginasMultivitamin with iron relieves deficienciesAngelique Ramos PascuaAinda não há avaliações
- Incomplete AbortionDocumento22 páginasIncomplete AbortionAJ Dalawampu100% (2)
- OB - Abortion (NER)Documento6 páginasOB - Abortion (NER)gellie gellesAinda não há avaliações
- 6 PathophysiologyDocumento2 páginas6 PathophysiologyAJ SnowhiAinda não há avaliações
- Last-minute Biology revision guide for Class XII students in Jaipur regionDocumento18 páginasLast-minute Biology revision guide for Class XII students in Jaipur regionghjAinda não há avaliações
- Pathophysiology (Normal Spontaneous Vaginal Delivery)Documento2 páginasPathophysiology (Normal Spontaneous Vaginal Delivery)Jose Bryan NacillaAinda não há avaliações
- Pathophysiology (Normal Spontaneous Vaginal Delivery)Documento2 páginasPathophysiology (Normal Spontaneous Vaginal Delivery)Jose Bryan NacillaAinda não há avaliações
- Blastocyst Development and Implantation (ANA 205Documento27 páginasBlastocyst Development and Implantation (ANA 205Ogundipe olorunfemiAinda não há avaliações
- MCHN 3RD LectDocumento9 páginasMCHN 3RD LectZahAinda não há avaliações
- Maternal Health: Pregnancy Signs and StagesDocumento9 páginasMaternal Health: Pregnancy Signs and StagesjisooAinda não há avaliações
- Malaria PathophysiologyDocumento1 páginaMalaria Pathophysiologykaye040375% (4)
- NCP Normal Spontaneous Delivery Disturbed Sleeping PatternDocumento2 páginasNCP Normal Spontaneous Delivery Disturbed Sleeping Patternkaye040389% (27)
- Pa Tho Irritable Bowel SyndromeDocumento1 páginaPa Tho Irritable Bowel Syndromekaye0403Ainda não há avaliações
- Learning DisabilitiesDocumento40 páginasLearning Disabilitieskaye0403Ainda não há avaliações
- Temenoff BiomaterialsDocumento0 páginaTemenoff BiomaterialsJason Chou0% (9)
- Syllabus of BS English (Language & Literature) Implemented From 1 Semester Fall 2021Documento95 páginasSyllabus of BS English (Language & Literature) Implemented From 1 Semester Fall 2021Lahore PunjabAinda não há avaliações
- Case Study For Engineering ProblemDocumento37 páginasCase Study For Engineering ProblemAfiq AfifeAinda não há avaliações
- Specific Gravity by Pycnometer MethodDocumento4 páginasSpecific Gravity by Pycnometer Methodأحمد جاسم محمدAinda não há avaliações
- Physiotherapy's Role in Rehabilitation and Health Promotion Across the LifespanDocumento3 páginasPhysiotherapy's Role in Rehabilitation and Health Promotion Across the LifespanMariana OspinaAinda não há avaliações
- Shukr Thankfulness To Allah Grade 12Documento21 páginasShukr Thankfulness To Allah Grade 12Salman Mohammed AbdullahAinda não há avaliações
- Customer Satisfaction and Firm Performance: Insights From Over A Quarter Century of Empirical ResearchDocumento22 páginasCustomer Satisfaction and Firm Performance: Insights From Over A Quarter Century of Empirical ResearchMohamedAliBenAmorAinda não há avaliações
- Sector:: Automotive/Land Transport SectorDocumento20 páginasSector:: Automotive/Land Transport SectorVedin Padilla Pedroso92% (12)
- Magic Writ: Textual Amulets Worn On The Body For Protection: Don C. SkemerDocumento24 páginasMagic Writ: Textual Amulets Worn On The Body For Protection: Don C. SkemerAsim HaseljicAinda não há avaliações
- Advanced Management Accounting: ConceptsDocumento47 páginasAdvanced Management Accounting: ConceptsGEDDIGI BHASKARREDDYAinda não há avaliações
- Case 3:09 CV 01494 MODocumento13 páginasCase 3:09 CV 01494 MOAnonymous HiNeTxLMAinda não há avaliações
- Syllabus Mac1105 M 530 - 8 PM 203080Documento6 páginasSyllabus Mac1105 M 530 - 8 PM 203080api-261843361Ainda não há avaliações
- ALL INDIA NURSING TEST REVIEWDocumento102 páginasALL INDIA NURSING TEST REVIEWDr-Sanjay SinghaniaAinda não há avaliações
- AC413 Operations Auditing Outline & ContentDocumento29 páginasAC413 Operations Auditing Outline & ContentErlie CabralAinda não há avaliações
- Maternal and Perinatal Outcome in Jaundice Complicating PregnancyDocumento10 páginasMaternal and Perinatal Outcome in Jaundice Complicating PregnancymanognaaaaAinda não há avaliações
- Chapter-1 of F.mensurationDocumento8 páginasChapter-1 of F.mensurationpradeeppoddarAinda não há avaliações
- Why Men Are The Submissive SexDocumento8 páginasWhy Men Are The Submissive SexWilliam Bond89% (9)
- ESL S9 W3 P14-15 Project Challenge Part 2Documento27 páginasESL S9 W3 P14-15 Project Challenge Part 2Emma Catherine BurkeAinda não há avaliações
- Terese LiteDocumento211 páginasTerese Liteoguruma100% (1)
- ME8513 & Metrology and Measurements LaboratoryDocumento3 páginasME8513 & Metrology and Measurements LaboratorySakthivel KarunakaranAinda não há avaliações
- Environmental Sanitation LessonDocumento4 páginasEnvironmental Sanitation LessonMARIS GRACE CARVAJALAinda não há avaliações
- Chap 006Documento50 páginasChap 006Martin TrịnhAinda não há avaliações
- Teresa R. Ignacio, Represented by Her Attorney-In-fact, Roberto R. Ignacio, Petitioner, V. Office of The City Treasurer of Quezon City, Et. Al.Documento2 páginasTeresa R. Ignacio, Represented by Her Attorney-In-fact, Roberto R. Ignacio, Petitioner, V. Office of The City Treasurer of Quezon City, Et. Al.Pam Otic-ReyesAinda não há avaliações
- DIASS - Quarter3 - Module1 - Week1 - Pure and Applied Social Sciences - V2Documento18 páginasDIASS - Quarter3 - Module1 - Week1 - Pure and Applied Social Sciences - V2Stephanie Tamayao Lumbo100% (1)
- Objective/Multiple Type QuestionDocumento14 páginasObjective/Multiple Type QuestionMITALI TAKIAR100% (1)
- Definitions - Estoppel PDFDocumento4 páginasDefinitions - Estoppel PDFsrrockygAinda não há avaliações
- Chronic Laryngitis in CHU Yalgado Ouedraogo: Epidemiological and Diagnostic AspectsDocumento4 páginasChronic Laryngitis in CHU Yalgado Ouedraogo: Epidemiological and Diagnostic AspectsMarlina ElvianaAinda não há avaliações
- HDPS 1303 - 930425105424Documento6 páginasHDPS 1303 - 930425105424Cheryl LimAinda não há avaliações
- QDEGNSWDocumento2 páginasQDEGNSWSnehin PoddarAinda não há avaliações
- Summary of Verb TensesDocumento4 páginasSummary of Verb TensesRamir Y. LiamusAinda não há avaliações