Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Laporan Kasus Kegawatdaruratan Intoksikasi Metanol: Oleh: Edah HumaidahDocumento1 páginaLaporan Kasus Kegawatdaruratan Intoksikasi Metanol: Oleh: Edah HumaidahEdah HumaidahAinda não há avaliações
- 1 - 10 - 209case Report-Methanol Intoxication Complicated With Acute Pancreatitis Alcoholic Ketoacidosis and Intracranial HemorrhageDocumento3 páginas1 - 10 - 209case Report-Methanol Intoxication Complicated With Acute Pancreatitis Alcoholic Ketoacidosis and Intracranial HemorrhageEdah HumaidahAinda não há avaliações
- Prevalens 2014 FranceDocumento9 páginasPrevalens 2014 FranceEdah HumaidahAinda não há avaliações
- Angela Aki TegamiDocumento5 páginasAngela Aki TegamiEdah HumaidahAinda não há avaliações
- Angela Aki TegamiDocumento5 páginasAngela Aki TegamiEdah HumaidahAinda não há avaliações
- SympathiDocumento2 páginasSympathiEdah HumaidahAinda não há avaliações
- Immune Thrombocitopeni PurpuraDocumento8 páginasImmune Thrombocitopeni PurpuraEdah HumaidahAinda não há avaliações
- International Headache Classification III ICHD III 2013 Beta 1Documento180 páginasInternational Headache Classification III ICHD III 2013 Beta 1Fityan Aulia RahmanAinda não há avaliações
- Hellp Syndr, SibaiDocumento21 páginasHellp Syndr, SibaiMohamed MukhrizAinda não há avaliações
- 2011 ITP Pocket GuideDocumento8 páginas2011 ITP Pocket GuidevtAinda não há avaliações
- Jurnal Karies Gigi Pada AnakDocumento11 páginasJurnal Karies Gigi Pada AnakYock HeadShooter0% (1)
- Lynne Graham Damiano S Return by Lynne Graham PDFDocumento90 páginasLynne Graham Damiano S Return by Lynne Graham PDFEdah Humaidah88% (16)
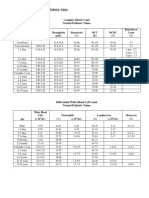
- 30a2131 Complete Blood Count Normal Pediatric Values PDFDocumento1 página30a2131 Complete Blood Count Normal Pediatric Values PDFReziel Basilan Manalo100% (2)
- Vascular Trauma and Its ManagementDocumento5 páginasVascular Trauma and Its ManagementEdah HumaidahAinda não há avaliações
- International Headache Classification III ICHD III 2013 Beta 1Documento180 páginasInternational Headache Classification III ICHD III 2013 Beta 1Fityan Aulia RahmanAinda não há avaliações
- Epidemiology and Outcome of Vascular Trauma at A British Major Trauma CentreDocumento7 páginasEpidemiology and Outcome of Vascular Trauma at A British Major Trauma CentreEdah HumaidahAinda não há avaliações
- Existing Trauma and Critical Care Scoring SystemsDocumento8 páginasExisting Trauma and Critical Care Scoring SystemsEdah HumaidahAinda não há avaliações
- Anesthesia For LaparosDocumento12 páginasAnesthesia For LaparosEdah HumaidahAinda não há avaliações
- F.3 Ocd 072012Documento17 páginasF.3 Ocd 072012Edah Humaidah100% (1)
- WhenDocumento3 páginasWhenEdah HumaidahAinda não há avaliações
- Steroid LepraDocumento20 páginasSteroid LepraEdah HumaidahAinda não há avaliações
- Penelitian LepraDocumento13 páginasPenelitian LepraEdah HumaidahAinda não há avaliações
- Informed Consent 1Documento11 páginasInformed Consent 1Edah HumaidahAinda não há avaliações
- Acute Diare WHO 2005Documento50 páginasAcute Diare WHO 2005Boby Abdul RahmanAinda não há avaliações
- Acute Diare WHO 2005Documento50 páginasAcute Diare WHO 2005Boby Abdul RahmanAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Gerdes Segal Lietz 2010Documento19 páginasGerdes Segal Lietz 2010Miguel Córdova RamirezAinda não há avaliações
- 1-2-5 - Assignment - UPLOADDocumento6 páginas1-2-5 - Assignment - UPLOADmdzvi86% (14)
- Report On BGTDocumento5 páginasReport On BGTaneela khan100% (2)
- The Self From The Perspective of PsychologyDocumento16 páginasThe Self From The Perspective of PsychologyTimothy Lontok100% (2)
- Organizational CultureDocumento25 páginasOrganizational CultureArcee Ardiente Mondragon100% (3)
- PNL PolacoDocumento11 páginasPNL PolacoFran Gomez MassaccesiAinda não há avaliações
- Effects of Neuro-Linguistic Programming (NLP) Imagery Model On Enhancing Kickboxers' PerformanceDocumento11 páginasEffects of Neuro-Linguistic Programming (NLP) Imagery Model On Enhancing Kickboxers' PerformanceIveta NikolovaAinda não há avaliações
- LAC Session Guide (Online) - Direct Fluency Instruction For Developing Independent ReadersDocumento7 páginasLAC Session Guide (Online) - Direct Fluency Instruction For Developing Independent ReadersJhe AzañaAinda não há avaliações
- Klassen Froese Klassen 2014 RoleofInterestDocumento19 páginasKlassen Froese Klassen 2014 RoleofInterestNur NabilahAinda não há avaliações
- Elements of Communication ProcessDocumento4 páginasElements of Communication ProcessSue S. ZandersAinda não há avaliações
- EFT Premarital Curriculum - JordanDocumento33 páginasEFT Premarital Curriculum - JordanojmalleryAinda não há avaliações
- Assessment of Activities of Daily Living, Self-Care, and IndependenceDocumento11 páginasAssessment of Activities of Daily Living, Self-Care, and IndependenceayuAinda não há avaliações
- EDUC 202 Lesson 1.1Documento7 páginasEDUC 202 Lesson 1.1Stephanie Jane PultaAinda não há avaliações
- Loss of Appetite - NCPDocumento1 páginaLoss of Appetite - NCPlyrad1168% (25)
- Dari DausDocumento4 páginasDari DausSalmah YusufAinda não há avaliações
- AUTISMDocumento25 páginasAUTISMAyesha ArshedAinda não há avaliações
- Mentally Strong People (Articles)Documento4 páginasMentally Strong People (Articles)dllordAinda não há avaliações
- Basic Concepts On PsychopharmacologyDocumento47 páginasBasic Concepts On PsychopharmacologyjisooAinda não há avaliações
- Alcoholism Is A Disinhibitory Disorder: Neurophysiological Evidence From A Go/No-Go TaskDocumento21 páginasAlcoholism Is A Disinhibitory Disorder: Neurophysiological Evidence From A Go/No-Go TaskmirymirelaAinda não há avaliações
- ISC Psychology at 2021Documento7 páginasISC Psychology at 2021vijayAinda não há avaliações
- Types of ValidityDocumento4 páginasTypes of ValidityShireen XadaAinda não há avaliações
- Introduction To Psychiatric Nursing: Module 2: ConceptsDocumento26 páginasIntroduction To Psychiatric Nursing: Module 2: ConceptsJoric MagusaraAinda não há avaliações
- Clinicians' Perceptions of The Benefits of Aquatic Therapy For Young Children With Autism A Preliminary StudyDocumento10 páginasClinicians' Perceptions of The Benefits of Aquatic Therapy For Young Children With Autism A Preliminary Study黃安全Ainda não há avaliações
- Second Language Acquisition: Krashen's Hypotheses of His Monitor TheoryDocumento2 páginasSecond Language Acquisition: Krashen's Hypotheses of His Monitor Theoryyas serAinda não há avaliações
- Printable Iq Test With Answers PDFDocumento2 páginasPrintable Iq Test With Answers PDFBiniam Nega25% (12)
- Kyambogo University: Faculty of Engineering Depertment of Civil and Building EngineeringDocumento4 páginasKyambogo University: Faculty of Engineering Depertment of Civil and Building Engineeringskalema34Ainda não há avaliações
- Classical ConditiongDocumento16 páginasClassical ConditiongLiana OlagAinda não há avaliações
- Distúrbios Neurocomportamentais Presos em Alcatraz: Relatos de Caso em Três Famosos PresidiáriosDocumento3 páginasDistúrbios Neurocomportamentais Presos em Alcatraz: Relatos de Caso em Três Famosos PresidiáriosTelenrico MatemáticoAinda não há avaliações
- Ricks Iris2Documento6 páginasRicks Iris2api-377713383Ainda não há avaliações
- Getting 360 Degree Feedback RightDocumento13 páginasGetting 360 Degree Feedback RightLawi Anupam100% (2)