Você também pode gostar
- C6 Psychological DisorderDocumento9 páginasC6 Psychological DisorderHanan FuadAinda não há avaliações
- Definition of Terms PDFDocumento7 páginasDefinition of Terms PDFkireeeAinda não há avaliações
- General Definition, Causes, and Types of Mental IllnessDocumento6 páginasGeneral Definition, Causes, and Types of Mental Illnesszahra03762Ainda não há avaliações
- Causes and Types of Mental DisordersDocumento12 páginasCauses and Types of Mental DisordersJay-Jay Bordeos100% (1)
- The Psychiatric ER Survival Guide: Tips for ResidentsDocumento32 páginasThe Psychiatric ER Survival Guide: Tips for Residentsmonkey85222Ainda não há avaliações
- Mental IllnessDocumento5 páginasMental Illnessapi-351578529Ainda não há avaliações
- Panna Dhai Maa Subharti Nursing College: Topic: Mood Disorder Amritanshu Chanchal M.SC Nursing 2 YearDocumento42 páginasPanna Dhai Maa Subharti Nursing College: Topic: Mood Disorder Amritanshu Chanchal M.SC Nursing 2 YearamritanshuAinda não há avaliações
- Notes On Psych QbankDocumento16 páginasNotes On Psych Qbankamcmed100% (1)
- Mental Health Check in Tip SheetDocumento3 páginasMental Health Check in Tip SheetDiana SamAinda não há avaliações
- Mood Disorders OutlineDocumento19 páginasMood Disorders OutlineAki HimeAinda não há avaliações
- Understanding Psychological DisordersDocumento166 páginasUnderstanding Psychological DisordersYasirali1999gmail.com YasiraliAinda não há avaliações
- Dissociation and Dissociative DisordersDocumento20 páginasDissociation and Dissociative DisordersRicky DAinda não há avaliações
- Abnormal Psychology, Twelfth Edition: SchizophreniaDocumento40 páginasAbnormal Psychology, Twelfth Edition: SchizophreniaSheAinda não há avaliações
- 4-Dissociation and FormDocumento30 páginas4-Dissociation and FormArmandoAinda não há avaliações
- Patterns of Maladaptive BehaviorDocumento49 páginasPatterns of Maladaptive BehaviorArrelee MangasparAinda não há avaliações
- Understanding Depression: Helping Families & Friends Find Better WaysDocumento4 páginasUnderstanding Depression: Helping Families & Friends Find Better WaysRajAnandAinda não há avaliações
- FactSheets FullDocumento28 páginasFactSheets FullGinaAinda não há avaliações
- 3 - Mood DisordersDocumento44 páginas3 - Mood DisordersBoss --Ainda não há avaliações
- Psychiatric and Mental Health Nursing - Wikipedia PDFDocumento83 páginasPsychiatric and Mental Health Nursing - Wikipedia PDFJanani AmmuAinda não há avaliações
- Behavioral TherapyDocumento54 páginasBehavioral TherapyIsha BhusalAinda não há avaliações
- Psychosis Neurosis and Othe Mental DisorderDocumento15 páginasPsychosis Neurosis and Othe Mental DisorderEr Ankita ChaudharyAinda não há avaliações
- Chapter 8 Mental Health and Mental IllnessDocumento52 páginasChapter 8 Mental Health and Mental Illnesskyro draxAinda não há avaliações
- Exploring The Relationship Between Non Suicidal Self-Injury and Borderline Personality Traits in Young AdultsDocumento9 páginasExploring The Relationship Between Non Suicidal Self-Injury and Borderline Personality Traits in Young Adultsme13Ainda não há avaliações
- Personality DisordersDocumento95 páginasPersonality Disorderscatherine faith gallemitAinda não há avaliações
- Anxiety Disorders I Part 1: Ethel Maureen P. Pagaddu, MDDocumento7 páginasAnxiety Disorders I Part 1: Ethel Maureen P. Pagaddu, MDRaiMalsiPilarAinda não há avaliações
- What To Do If You're Feeling SuicidalDocumento3 páginasWhat To Do If You're Feeling Suicidalapi-346509377Ainda não há avaliações
- Early Identification Psychosis: PrimerDocumento16 páginasEarly Identification Psychosis: PrimerGrace LAinda não há avaliações
- Daily self-care checklist for chronic illnessDocumento3 páginasDaily self-care checklist for chronic illnessdepanqueAinda não há avaliações
- Understanding and Teaching Students With Traumatic Brain InjuryDocumento38 páginasUnderstanding and Teaching Students With Traumatic Brain InjuryJeffAinda não há avaliações
- What are the most common types of learning disabilitiesDocumento10 páginasWhat are the most common types of learning disabilitiesjabea lyongaAinda não há avaliações
- PsychosisDocumento2 páginasPsychosisGrace LAinda não há avaliações
- NCM 105 Childhood Developmental DoDocumento12 páginasNCM 105 Childhood Developmental DoSandra GabasAinda não há avaliações
- Chapter 16 - Psychological Disorders NotesDocumento5 páginasChapter 16 - Psychological Disorders NotesManan JainAinda não há avaliações
- Non-Suicidal Self-Injury Assessment Tool Nssi-AtDocumento10 páginasNon-Suicidal Self-Injury Assessment Tool Nssi-Atapi-353060939Ainda não há avaliações
- Psychiatric Comprehensive Case StudyDocumento10 páginasPsychiatric Comprehensive Case Studyapi-5390652010% (1)
- Schizoaffective Disorder FactsheetDocumento16 páginasSchizoaffective Disorder FactsheetVictoria AdhityaAinda não há avaliações
- Psychology 1010Documento73 páginasPsychology 1010Jorge Cuello VasquezAinda não há avaliações
- Anxiety DisordersDocumento20 páginasAnxiety DisordersHndrAinda não há avaliações
- Treatment of Psychological DisordersDocumento34 páginasTreatment of Psychological DisordersAndreia AlmeidaAinda não há avaliações
- DepressionDocumento2 páginasDepressionapi-263996400Ainda não há avaliações
- Mental Health and Mental IllnessDocumento15 páginasMental Health and Mental Illnessronasoldevilla100% (3)
- Use Drugs - Pay To Die Drugs AddictionDocumento11 páginasUse Drugs - Pay To Die Drugs AddictionelvineAinda não há avaliações
- Psychological Disorders: AP Psychology Mr. HollandDocumento20 páginasPsychological Disorders: AP Psychology Mr. Hollandyummywords1254Ainda não há avaliações
- Anxiety and Stress-Related IllnessDocumento171 páginasAnxiety and Stress-Related Illnessbluecindy87Ainda não há avaliações
- Why Do Teens Consider Suicide (EAPP)Documento5 páginasWhy Do Teens Consider Suicide (EAPP)michaellamigas04Ainda não há avaliações
- Personality Disorder (F60) : ParanoidDocumento5 páginasPersonality Disorder (F60) : ParanoidboblishAinda não há avaliações
- Chapter 14 Psychological Disorders.Documento9 páginasChapter 14 Psychological Disorders.BorisVanIndigoAinda não há avaliações
- Psy 214 Lwcture 7Documento27 páginasPsy 214 Lwcture 7Hope MashakeniAinda não há avaliações
- Borderline Personality DisorderDocumento9 páginasBorderline Personality DisorderSiva Nandhan0% (1)
- Delusional DisorderDocumento4 páginasDelusional DisorderDr-Mohamed EssawyAinda não há avaliações
- Mental Illness: SymtomsDocumento17 páginasMental Illness: SymtomsDaphnae GuzonAinda não há avaliações
- Mental Health Class Assignment 1 Week 7 Sem 3Documento17 páginasMental Health Class Assignment 1 Week 7 Sem 3api-582247328Ainda não há avaliações
- What Exactly Is A Mental IllnessDocumento2 páginasWhat Exactly Is A Mental IllnessEllee Hades100% (1)
- The Signs of Controlling BehaviourDocumento3 páginasThe Signs of Controlling BehaviourKarthik VasireddyAinda não há avaliações
- Bender, Mirror, Mirror On The Wall, Reflecting On NarcissismDocumento10 páginasBender, Mirror, Mirror On The Wall, Reflecting On NarcissismjuaromerAinda não há avaliações
- Allan V. Horwitz, Jerome C. Wakefield, Robert L. Spitzer - The Loss of SadnessDocumento304 páginasAllan V. Horwitz, Jerome C. Wakefield, Robert L. Spitzer - The Loss of SadnessLucas Dutra100% (1)
- Suicide: A Temporary Solution For A Temporary ProblemDocumento20 páginasSuicide: A Temporary Solution For A Temporary ProblemurvashichaudharyAinda não há avaliações
- Psychological Disorders: A Unit Lesson Plan For High School Psychology TeachersDocumento57 páginasPsychological Disorders: A Unit Lesson Plan For High School Psychology TeachersMusthafa RafiAinda não há avaliações
- From Nope to Hope: How I Overcame My Suicidal Thoughts (and How You Can Too)No EverandFrom Nope to Hope: How I Overcame My Suicidal Thoughts (and How You Can Too)Ainda não há avaliações
- ConcluDocumento1 páginaConcluapi-270635809Ainda não há avaliações
- IntroDocumento1 páginaIntroapi-270635809Ainda não há avaliações
- GlossaryDocumento7 páginasGlossaryapi-270635809Ainda não há avaliações
- Memory Intelligence and States of MindDocumento11 páginasMemory Intelligence and States of Mindapi-270635809Ainda não há avaliações
- Sensation and PerceptionDocumento11 páginasSensation and Perceptionapi-270635809100% (2)
- Social PsychologyDocumento15 páginasSocial Psychologyapi-270635809Ainda não há avaliações
- Motivation and Emotion 1Documento12 páginasMotivation and Emotion 1api-270635809Ainda não há avaliações
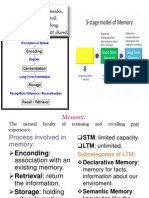
- MemoryDocumento4 páginasMemoryapi-270635809Ainda não há avaliações
- Motivation and EmotionDocumento17 páginasMotivation and Emotionapi-270635809Ainda não há avaliações
- Introduction To Learning Theory and Behavioral PsychologyDocumento4 páginasIntroduction To Learning Theory and Behavioral PsychologyKaruna RajiahAinda não há avaliações
- 13 Personality DevelopmentDocumento32 páginas13 Personality Developmentapi-270635809Ainda não há avaliações
- 12 Chapter 2 BiopsychologyDocumento14 páginas12 Chapter 2 Biopsychologyapi-270635809Ainda não há avaliações
- 4 Introduction To PsychologyDocumento4 páginas4 Introduction To Psychologyapi-270635809Ainda não há avaliações
- 8 Types of ResearchDocumento2 páginas8 Types of Researchapi-270635809Ainda não há avaliações
- History of Psychology Milestones (387 BC to PresentDocumento4 páginasHistory of Psychology Milestones (387 BC to PresentKrea Quizo100% (1)
- IndexDocumento1 páginaIndexapi-270635809Ainda não há avaliações
- 7 Experimental MethodsDocumento2 páginas7 Experimental Methodsapi-270635809Ainda não há avaliações
- Psic EdDocumento27 páginasPsic EdNicolás Robertino LombardiAinda não há avaliações
- Healing The Heart of Trauma and Dissociation With Emdr and Ego State Therapy 1st Edition Ebook PDFDocumento62 páginasHealing The Heart of Trauma and Dissociation With Emdr and Ego State Therapy 1st Edition Ebook PDFkarla.woodruff227100% (41)
- Recovered Memories - Repressed Memory AccuracyDocumento6 páginasRecovered Memories - Repressed Memory AccuracysmartnewsAinda não há avaliações
- Practical Research II - Quantitative ResearchDocumento39 páginasPractical Research II - Quantitative ResearchsethtimkangAinda não há avaliações
- Evolve Mental Health Ch. 17Documento36 páginasEvolve Mental Health Ch. 17wn4tbAinda não há avaliações
- Closing The Front Door of ChilDocumento23 páginasClosing The Front Door of Chilapi-687461513Ainda não há avaliações
- Story, Science, and Self-Care in A Refugee Community:: Initial Impact of The Field Guide For Barefoot PsychologyDocumento33 páginasStory, Science, and Self-Care in A Refugee Community:: Initial Impact of The Field Guide For Barefoot PsychologyEsteban Humberto CanoAinda não há avaliações
- Adverse Childhood Experiences and TraumaDocumento4 páginasAdverse Childhood Experiences and TraumaAndreea Pal100% (1)
- Presentasi Kelompok 7 Tentang Gangguan JiwaDocumento83 páginasPresentasi Kelompok 7 Tentang Gangguan Jiwamichael palitAinda não há avaliações
- Survival StrategiesDocumento8 páginasSurvival StrategiesDr Jitender SinghAinda não há avaliações
- Core-Competencies-Disaster Mental HealthDocumento8 páginasCore-Competencies-Disaster Mental Healthapi-246285190Ainda não há avaliações
- How to Stop Child AbuseDocumento28 páginasHow to Stop Child AbuseLinta Khan100% (2)
- The Self Care Project WorksheetsDocumento15 páginasThe Self Care Project WorksheetsPrince AroraAinda não há avaliações
- Adolescent Relationship, Gender and SexualityDocumento55 páginasAdolescent Relationship, Gender and SexualityVelprashanth VenkatesanAinda não há avaliações
- Explanations For Survival by Jewish Survivors of The Holocaust - GoldenbergDocumento14 páginasExplanations For Survival by Jewish Survivors of The Holocaust - GoldenberglecteurscribdAinda não há avaliações
- Post-Traumatic Stress DisorderDocumento12 páginasPost-Traumatic Stress Disorderecbt100% (2)
- Application For A Derived Grade 2020: Information and Instructions For Students and Parents/whanauDocumento8 páginasApplication For A Derived Grade 2020: Information and Instructions For Students and Parents/whanauCallum McKinnonAinda não há avaliações
- PSPA3714 Chapter 5 2021Documento70 páginasPSPA3714 Chapter 5 2021Kamogelo MakhuraAinda não há avaliações
- The Advent of Rape Pornography in Sri LankaDocumento8 páginasThe Advent of Rape Pornography in Sri LankaThavam RatnaAinda não há avaliações
- Child Welfare Task Force Report v6Documento25 páginasChild Welfare Task Force Report v6WDIV/ClickOnDetroitAinda não há avaliações
- Acting Out and Working-Through Intergenerational Trauma: An Analysis of The Movie Miss Peregrine's Home For Peculiar ChildrenDocumento16 páginasActing Out and Working-Through Intergenerational Trauma: An Analysis of The Movie Miss Peregrine's Home For Peculiar ChildrenmarinaAinda não há avaliações
- Art As Projective Medium - An Educational Psychological Model To Address Unresolved Trauma in Young AdultsDocumento14 páginasArt As Projective Medium - An Educational Psychological Model To Address Unresolved Trauma in Young AdultsDaniela JovelAinda não há avaliações
- Supreme Court to Hear Appeal in Child Sex Abuse CaseDocumento34 páginasSupreme Court to Hear Appeal in Child Sex Abuse CaseakankshaAinda não há avaliações
- Richard W. Roberts ComplaintDocumento21 páginasRichard W. Roberts ComplaintThe Salt Lake TribuneAinda não há avaliações
- Newport, D.J. and Nemeroff, C.B. Neurobiology of Posttraumatic Stress Disorder. Cognitive Neuroscience JAARTALDocumento8 páginasNewport, D.J. and Nemeroff, C.B. Neurobiology of Posttraumatic Stress Disorder. Cognitive Neuroscience JAARTALg10564433Ainda não há avaliações
- Amygdala Retraining JHH Sept 2010Documento40 páginasAmygdala Retraining JHH Sept 2010OmmachineAinda não há avaliações
- Kick Start Recovery PDocumento21 páginasKick Start Recovery Pjames.dharmawanAinda não há avaliações
- Concept Paper (Earthquake in Bohol)Documento1 páginaConcept Paper (Earthquake in Bohol)Jane SandovalAinda não há avaliações
- Dissociation and Dissociative Disorders Encyclopedia of Feeding and Eating DisordersDocumento7 páginasDissociation and Dissociative Disorders Encyclopedia of Feeding and Eating DisordersAdrián DelgadoAinda não há avaliações
- Midterm HRMDocumento8 páginasMidterm HRMGrad StudentAinda não há avaliações