Você também pode gostar
- Binocular Vision Anomalies Part 1Documento10 páginasBinocular Vision Anomalies Part 1irijoaAinda não há avaliações
- New in OrthopticsDocumento5 páginasNew in Orthopticsgargi.c100% (2)
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsNo EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsAinda não há avaliações
- Astigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandAstigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Orthoptic Exercises for OptometristsDocumento6 páginasOrthoptic Exercises for OptometristsCatalin GeorgeAinda não há avaliações
- Strabismus Quick GuideDocumento4 páginasStrabismus Quick Guideghitza80100% (1)
- Clinical Orthoptics 2019Documento97 páginasClinical Orthoptics 2019Joseph IsraelAinda não há avaliações
- Basic Eye ExamDocumento8 páginasBasic Eye ExamLisa AguilarAinda não há avaliações
- Vision RehabilitationDocumento46 páginasVision RehabilitationDrGENAinda não há avaliações
- NATIONAL OPTOMETRY BOARDS (NOB) Part I BASIC SCIENCE: Passbooks Study GuideNo EverandNATIONAL OPTOMETRY BOARDS (NOB) Part I BASIC SCIENCE: Passbooks Study GuideAinda não há avaliações
- The Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersNo EverandThe Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersAinda não há avaliações
- Binocular Vision - Orthoptics PDFDocumento147 páginasBinocular Vision - Orthoptics PDFMacarena Alvarez0% (1)
- The Skeffington Perspective of the Behavioral Model of Optometric Data Analysis and Vision CareNo EverandThe Skeffington Perspective of the Behavioral Model of Optometric Data Analysis and Vision CareAinda não há avaliações
- Contact Lenses For ChildrenDocumento6 páginasContact Lenses For ChildrenmelikebooksAinda não há avaliações
- Foreign Optometrist For CanadaDocumento9 páginasForeign Optometrist For CanadaABDUL HAMEEDAinda não há avaliações
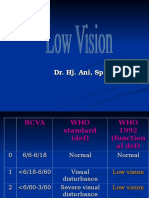
- Low VisionDocumento36 páginasLow VisionIqbal HabibieAinda não há avaliações
- Strabismus: By: Audra Bishop Beth Moline Elisabeth CohenDocumento60 páginasStrabismus: By: Audra Bishop Beth Moline Elisabeth CohenmalathiAinda não há avaliações
- The Spotty RetinaDocumento5 páginasThe Spotty RetinaJose Luis Mato AhcanAinda não há avaliações
- Accommodation TestsDocumento11 páginasAccommodation TestsNat Kang100% (1)
- Clinical Accomodation ProblemsDocumento15 páginasClinical Accomodation ProblemsdwindaAinda não há avaliações
- Far-Sightedness, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandFar-Sightedness, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- CET Strabismus Investigation and ManagementDocumento6 páginasCET Strabismus Investigation and ManagementSitifa AisaraAinda não há avaliações
- Review of Low Vision RehabilitationDocumento47 páginasReview of Low Vision Rehabilitationmulito777100% (1)
- Contact Lens Design Tables: Tables for the Determination of Surface Radii of Curvature of Hard Contact Lenses to Give a Required Axial Edge LiftNo EverandContact Lens Design Tables: Tables for the Determination of Surface Radii of Curvature of Hard Contact Lenses to Give a Required Axial Edge LiftAinda não há avaliações
- Care of the Child with Ophthalmic ProblemsNo EverandCare of the Child with Ophthalmic ProblemsAinda não há avaliações
- Esotropia PDFDocumento41 páginasEsotropia PDFputriAinda não há avaliações
- 12 - Objective RefractionDocumento11 páginas12 - Objective RefractionSumon SarkarAinda não há avaliações
- Basic Sciences in Ophthalmology - 9788184486087-EmailDocumento446 páginasBasic Sciences in Ophthalmology - 9788184486087-EmailwulanfarichahAinda não há avaliações
- Right Hand Column Guide to Eye Exam EssentialsDocumento3 páginasRight Hand Column Guide to Eye Exam Essentialssharu4291Ainda não há avaliações
- LOW VISION ASSESSMENT AND REHABILITATION GUIDEDocumento50 páginasLOW VISION ASSESSMENT AND REHABILITATION GUIDEHerin NataliaAinda não há avaliações
- Visual FieldsDocumento86 páginasVisual FieldsoptorameshgpAinda não há avaliações
- Medical management of glaucoma for optometristsDocumento9 páginasMedical management of glaucoma for optometristsAmador GielasAinda não há avaliações
- Optometry's Role As A Primary Health Care Provider in Managed CareDocumento13 páginasOptometry's Role As A Primary Health Care Provider in Managed CareANDREW OMAKAAinda não há avaliações
- Understanding Aberrometry for Eye CareDocumento54 páginasUnderstanding Aberrometry for Eye Caresightbd100% (2)
- Simplifying Strabismus: A Practical Approach to Diagnosis and ManagementNo EverandSimplifying Strabismus: A Practical Approach to Diagnosis and ManagementAinda não há avaliações
- Choice of Artificial Tear Formulation For Patients With Dry Eye: Where Do We Start?Documento5 páginasChoice of Artificial Tear Formulation For Patients With Dry Eye: Where Do We Start?Priscila Verduzco100% (1)
- Post Trauma Vision SyndromeDocumento10 páginasPost Trauma Vision SyndromeEvelyn SepulvedaAinda não há avaliações
- CPG 19Documento78 páginasCPG 19anon-24970100% (1)
- Contact Applanation TonometryDocumento6 páginasContact Applanation TonometryAmirhosseinSamadzadehAinda não há avaliações
- Core Ophthalmic Knowledge: Academy MOC Essentials® Practicing Ophthalmologists Curriculum 2017-2019Documento294 páginasCore Ophthalmic Knowledge: Academy MOC Essentials® Practicing Ophthalmologists Curriculum 2017-2019Dayana Rosales DuránAinda não há avaliações
- Glaucoma and Ocular HypertensionDocumento6 páginasGlaucoma and Ocular HypertensionsoniasistAinda não há avaliações
- A Critical Evaluation of The Evidence Supporting The Practice Behavioral Vision TherapyDocumento23 páginasA Critical Evaluation of The Evidence Supporting The Practice Behavioral Vision TherapyPierre A. RodulfoAinda não há avaliações
- RefraksiDocumento84 páginasRefraksinaroetocapkutilAinda não há avaliações
- Examination of Case of StrabismusDocumento76 páginasExamination of Case of StrabismusDr-SunitaVimal100% (1)
- Cycloplegic Retinoscopy in InfancyDocumento5 páginasCycloplegic Retinoscopy in InfancyStrauss de LangeAinda não há avaliações
- Clinical Optometry Related FilesDocumento14 páginasClinical Optometry Related FilesHasan AnsariAinda não há avaliações
- Nungki-Esodeviations & ExodeviationsDocumento36 páginasNungki-Esodeviations & ExodeviationsNia RoosdhantiaAinda não há avaliações
- PPP Refractive Error & Refractive Surgery PDFDocumento104 páginasPPP Refractive Error & Refractive Surgery PDFMia NursalamahAinda não há avaliações
- Everything You Need to Know About Artificial EyesDocumento24 páginasEverything You Need to Know About Artificial Eyesapoorva1509Ainda não há avaliações
- OptoPrep Part1 StudyCalendar 6-Month PDFDocumento7 páginasOptoPrep Part1 StudyCalendar 6-Month PDFmelanieAinda não há avaliações
- Brewster StereoscopeDocumento17 páginasBrewster StereoscopeNavami KrishnaAinda não há avaliações
- Sports Vision G. JanssenDocumento35 páginasSports Vision G. Janssenphilip davisAinda não há avaliações
- Clinical Exam For OphthalmologyDocumento6 páginasClinical Exam For Ophthalmologynuuraaisya50% (2)
- The Retina and its DisordersNo EverandThe Retina and its DisordersJoseph BesharseNota: 2 de 5 estrelas2/5 (2)
- Low Vision - Assistive DevicesDocumento89 páginasLow Vision - Assistive DevicesKavi Rehabian0% (1)
- The Supervisory Relationship Questionnaire (SRQ)Documento3 páginasThe Supervisory Relationship Questionnaire (SRQ)kartuteAinda não há avaliações
- Rephrasing Exercises - Exercices de Traduction IntralingualeDocumento89 páginasRephrasing Exercises - Exercices de Traduction IntralingualeIulia CalinAinda não há avaliações
- BowlbyArticleHarris BerintheArtsed1Documento5 páginasBowlbyArticleHarris BerintheArtsed1kartuteAinda não há avaliações
- Health Writing ChecklistDocumento13 páginasHealth Writing ChecklistkartuteAinda não há avaliações
- Verbs and PhonemicsDocumento4 páginasVerbs and PhonemicskartuteAinda não há avaliações
- The Psychological Impact of Hair Loss: Anxiety, Depression and Reduced Self-EsteemDocumento1 páginaThe Psychological Impact of Hair Loss: Anxiety, Depression and Reduced Self-EsteemkartuteAinda não há avaliações
- Newborn Care - 3A. Clinical History and ExaminationDocumento13 páginasNewborn Care - 3A. Clinical History and ExaminationkartuteAinda não há avaliações
- Brief Therapy Based On Interrupting Ironic Processes The Palo Alto ModelDocumento19 páginasBrief Therapy Based On Interrupting Ironic Processes The Palo Alto ModelkartuteAinda não há avaliações
- DJ Archive Inventory 2007Documento11 páginasDJ Archive Inventory 2007kartuteAinda não há avaliações
- SOCCONSTDocumento28 páginasSOCCONSTkartuteAinda não há avaliações
- Data Mining in The Pharmaceutical IndustryDocumento61 páginasData Mining in The Pharmaceutical IndustrykartuteAinda não há avaliações
- Data Mining in The Pharmaceutical IndustryDocumento61 páginasData Mining in The Pharmaceutical IndustrykartuteAinda não há avaliações
- Suicide Assessment and ScreeningDocumento46 páginasSuicide Assessment and ScreeningkartuteAinda não há avaliações
- The Family Semantics Grid (Ugazio)Documento28 páginasThe Family Semantics Grid (Ugazio)kartute100% (1)
- Clincal VignettesDocumento1 páginaClincal VignetteskartuteAinda não há avaliações
- Books For Clinical SupervisionDocumento5 páginasBooks For Clinical Supervisionkartute50% (2)
- McKinsey Cancer Center - Next Wave of Innovation in OncologyDocumento16 páginasMcKinsey Cancer Center - Next Wave of Innovation in OncologykartuteAinda não há avaliações
- Bullying PreventionDocumento49 páginasBullying PreventionkartuteAinda não há avaliações
- Manual Singer FileteadoraDocumento31 páginasManual Singer FileteadorakartuteAinda não há avaliações
- SFT ManualDocumento59 páginasSFT ManualMistor Dupois WilliamsAinda não há avaliações
- Key Systemic IdeasDocumento20 páginasKey Systemic IdeaskartuteAinda não há avaliações
- A Recent Trainee's PerspectiveDocumento13 páginasA Recent Trainee's PerspectivekartuteAinda não há avaliações
- Astrologers Cheat SheetDocumento1 páginaAstrologers Cheat Sheetkartute100% (1)
- Acuerdo Politica de Desarrollo Agrario Integral PDFDocumento22 páginasAcuerdo Politica de Desarrollo Agrario Integral PDFdianaAinda não há avaliações
- Social Withdrawal, Peer Rejection and BullyingDocumento15 páginasSocial Withdrawal, Peer Rejection and BullyingkartuteAinda não há avaliações
- Demistifying Social Media - 12Documento11 páginasDemistifying Social Media - 12AdnanaAinda não há avaliações
- 8020 RuleDocumento6 páginas8020 Rulezakria.zubair4388Ainda não há avaliações
- Marketing and The 7psDocumento10 páginasMarketing and The 7pskartuteAinda não há avaliações
- Glaucoma ChapterDocumento32 páginasGlaucoma ChapterAhmed Omara100% (5)
- Peripheral Ulcerative KeratitisDocumento145 páginasPeripheral Ulcerative KeratitisCarlos OrtegaAinda não há avaliações
- Recent Advances in Glaucoma Diagnosis and ManagementDocumento5 páginasRecent Advances in Glaucoma Diagnosis and ManagementLanangAinda não há avaliações
- Cataracts: ClassificationDocumento9 páginasCataracts: ClassificationRafay ChacharAinda não há avaliações
- Update On Optical Biometry and Intraocular Lens Power CalculationDocumento15 páginasUpdate On Optical Biometry and Intraocular Lens Power CalculationArdyAinda não há avaliações
- Predisposing Factors and Surgical Outcomes of Intraocular Lens Dislocation After PhacoemulsificationDocumento7 páginasPredisposing Factors and Surgical Outcomes of Intraocular Lens Dislocation After PhacoemulsificationUmmul AzizahAinda não há avaliações
- Treating Aphakia and Ectopia Lentis: Management Options for Lens DisplacementDocumento34 páginasTreating Aphakia and Ectopia Lentis: Management Options for Lens DisplacementMaham RehmanAinda não há avaliações
- MedCat Catalog 2017 2018Documento72 páginasMedCat Catalog 2017 2018minervamoonAinda não há avaliações
- 3D OCT 2000series en - BrochureDocumento9 páginas3D OCT 2000series en - BrochureRodrigo CatalánAinda não há avaliações
- Computer Vision SyndromDocumento25 páginasComputer Vision Syndromoieputri100% (1)
- Erode Hopsitals PDF FreeDocumento826 páginasErode Hopsitals PDF FreeKriti KumariAinda não há avaliações
- Pediatric Refractive Errors AssessmentDocumento81 páginasPediatric Refractive Errors Assessmenthenok birukAinda não há avaliações
- Qigong Eye ExercisesDocumento21 páginasQigong Eye Exercisesdanieljwu13100% (3)
- 06 Cornea PDFDocumento74 páginas06 Cornea PDFLeo TedjaAinda não há avaliações
- Care of The Patient With Presbyopia: Quick Reference GuideDocumento4 páginasCare of The Patient With Presbyopia: Quick Reference GuideFahmi_IskandarAinda não há avaliações
- Biology Investigatory Project (On Eye Diseases)Documento22 páginasBiology Investigatory Project (On Eye Diseases)diya65% (49)
- Final MBBS Part 1 Classes Schedule - Live UpdateDocumento6 páginasFinal MBBS Part 1 Classes Schedule - Live UpdateKrishna VamsiAinda não há avaliações
- Childhood BlindnessDocumento14 páginasChildhood BlindnessAditya Arya PutraAinda não há avaliações
- Science & Technology: The Eyes Have ItDocumento2 páginasScience & Technology: The Eyes Have ItHan YiAinda não há avaliações
- Chapter 14 15 16 PDFDocumento158 páginasChapter 14 15 16 PDFmp1757Ainda não há avaliações
- Nelson Textbook of Pediatrics, 21st Edition 2020 2Documento4 páginasNelson Textbook of Pediatrics, 21st Edition 2020 2lj ChuaAinda não há avaliações
- Clinical Study On Acupuncture For Quality of Life in Patients With Age-Related Macular DegenerationDocumento5 páginasClinical Study On Acupuncture For Quality of Life in Patients With Age-Related Macular DegenerationathiaAinda não há avaliações
- Adult Cataract: Cortical or Soft CataractDocumento6 páginasAdult Cataract: Cortical or Soft CataractJohn Christopher LucesAinda não há avaliações
- Valon 5G BrochureDocumento12 páginasValon 5G BrochureHaag-Streit UK (HS-UK)100% (1)
- Eye 10 Years-1Documento4 páginasEye 10 Years-1deepAinda não há avaliações
- Eye DonationDocumento4 páginasEye DonationVeeresh TopalakattiAinda não há avaliações
- Vitreous Hemorrhage: Retina Eye Specialists Retina Eye SpecialistsDocumento2 páginasVitreous Hemorrhage: Retina Eye Specialists Retina Eye SpecialistsMarcel Antek CivilAinda não há avaliações
- Amblyopia - Detection and TreatmentDocumento7 páginasAmblyopia - Detection and TreatmentPacoAinda não há avaliações
- Complications Caused by Contact Lens Wearing: Jasna Beljan, Kristina Beljan and Zdravko BeljanDocumento10 páginasComplications Caused by Contact Lens Wearing: Jasna Beljan, Kristina Beljan and Zdravko BeljanWagner de AvizAinda não há avaliações
- Waisbourd 2019Documento9 páginasWaisbourd 2019Leandro LopezAinda não há avaliações