Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- DementiaDocumento26 páginasDementianadya100% (4)
- Reffered PainDocumento26 páginasReffered PainHappy Septianto SAinda não há avaliações
- ABC Quality and Patient Saftey Workshop FinalDocumento68 páginasABC Quality and Patient Saftey Workshop Finalyousrazeidan1979Ainda não há avaliações
- Ascites Hrs B WPDocumento101 páginasAscites Hrs B WPGhias Un Nabi TayyabAinda não há avaliações
- 傷寒論 Shang Han LunDocumento3 páginas傷寒論 Shang Han LunDave Mainenti97% (30)
- Rheumatoid NCPDocumento2 páginasRheumatoid NCPMARK OLVIER E. MELCHORAinda não há avaliações
- Clark Et Al 2006 Cognitive Task AnalysisDocumento18 páginasClark Et Al 2006 Cognitive Task Analysisapi-264671444Ainda não há avaliações
- Animals Should Not Be Used As A Laboratory ToolsDocumento6 páginasAnimals Should Not Be Used As A Laboratory ToolsLuisa Castillo100% (1)
- General Format For Orthopedic AssessmentDocumento27 páginasGeneral Format For Orthopedic AssessmentMegha Patani100% (7)
- Shulman, L. S. (1987) - Knowledge and Teaching - Foundations of The New Reform. Harvard Educational Review, 57 (1), 1-23.Documento23 páginasShulman, L. S. (1987) - Knowledge and Teaching - Foundations of The New Reform. Harvard Educational Review, 57 (1), 1-23.Rodnarine100% (9)
- Salthouse 1996Documento26 páginasSalthouse 1996api-264671444Ainda não há avaliações
- Contoh JurnalDocumento10 páginasContoh JurnalRatih Atika SeptianiAinda não há avaliações
- Norman 2005 Research in Clinical Reasoning Past History and Current TrendsDocumento3 páginasNorman 2005 Research in Clinical Reasoning Past History and Current Trendsapi-264671444Ainda não há avaliações
- Ericsson 2007 An Expert-Performance Perspective of Research On Medical Expertise The Study of Clinical PerformanceDocumento7 páginasEricsson 2007 An Expert-Performance Perspective of Research On Medical Expertise The Study of Clinical Performanceapi-264671444Ainda não há avaliações
- Implications of The Act-R Learning Theory No Magic BulletsDocumento28 páginasImplications of The Act-R Learning Theory No Magic Bulletsapi-264671444Ainda não há avaliações
- Eichna 1991Documento11 páginasEichna 1991api-264671444Ainda não há avaliações
- Todd and Gigerenzer 2000 Prcis of Simple Heuristics That Make Us SmartDocumento54 páginasTodd and Gigerenzer 2000 Prcis of Simple Heuristics That Make Us Smartapi-264671444Ainda não há avaliações
- NomagicbulletsDocumento27 páginasNomagicbulletsapi-264671444Ainda não há avaliações
- Durning Et Al 2010 Aging and Cognitive Performance PhysiciansDocumento9 páginasDurning Et Al 2010 Aging and Cognitive Performance Physiciansapi-264671444Ainda não há avaliações
- Clark Pointing Placing 03Documento14 páginasClark Pointing Placing 03api-264671444Ainda não há avaliações
- Brown Et Al 1989Documento12 páginasBrown Et Al 1989api-264671444Ainda não há avaliações
- Eva Et Al 2005 Self-Assessment in The Health ProfessionsDocumento9 páginasEva Et Al 2005 Self-Assessment in The Health Professionsapi-264671444Ainda não há avaliações
- Eva Et Al 2006 The Difficulty With EsperienceDocumento8 páginasEva Et Al 2006 The Difficulty With Esperienceapi-264671444Ainda não há avaliações
- J Med Philos-1989-Coulson-109-46Documento38 páginasJ Med Philos-1989-Coulson-109-46api-264671444Ainda não há avaliações
- Lowenstein Et Al 2007 Medical School Faculty DiscontentDocumento8 páginasLowenstein Et Al 2007 Medical School Faculty Discontentapi-264671444Ainda não há avaliações
- Wilson 2002 Six Views of Embodied CognitionDocumento12 páginasWilson 2002 Six Views of Embodied Cognitionapi-264671444Ainda não há avaliações
- Guberman Development of Everyday Mathematics Child Development 67 4 1996 1609-1623Documento16 páginasGuberman Development of Everyday Mathematics Child Development 67 4 1996 1609-1623api-264671444Ainda não há avaliações
- Leinhardt Et Al 1986 The Cognitive Skill of TeachingDocumento21 páginasLeinhardt Et Al 1986 The Cognitive Skill of Teachingapi-264671444100% (1)
- Darosa Et Al 2011 Barriers To Effective Teaching 15Documento7 páginasDarosa Et Al 2011 Barriers To Effective Teaching 15api-264671444Ainda não há avaliações
- Pololi Et Al 2012 Why Are A Quarter of Faculty Considering Leaving 2012 OnlineproofDocumento11 páginasPololi Et Al 2012 Why Are A Quarter of Faculty Considering Leaving 2012 Onlineproofapi-264671444Ainda não há avaliações
- Results of An Academic Promotion and Career Path 13Documento7 páginasResults of An Academic Promotion and Career Path 13api-264671444Ainda não há avaliações
- Ericsson 2004 Deliberate Practice and The Acquisition and 22Documento12 páginasEricsson 2004 Deliberate Practice and The Acquisition and 22api-264671444Ainda não há avaliações
- Regehr Et Al 1996 Issues in Cognitive PsychologyDocumento14 páginasRegehr Et Al 1996 Issues in Cognitive Psychologyapi-264671444Ainda não há avaliações
- Kassirer 2010Documento7 páginasKassirer 2010api-264671444Ainda não há avaliações
- Mcgee Irby 1997 Teaching in The Outpatient ClinicDocumento7 páginasMcgee Irby 1997 Teaching in The Outpatient Clinicapi-264671444Ainda não há avaliações
- Sutkin Et Al 2008Documento15 páginasSutkin Et Al 2008api-264671444Ainda não há avaliações
- Harden Crosby 2000 The Good Teacher Is More Than A LecturerDocumento14 páginasHarden Crosby 2000 The Good Teacher Is More Than A Lecturerapi-264671444Ainda não há avaliações
- Wright Nejm 1998Documento8 páginasWright Nejm 1998api-264671444Ainda não há avaliações
- 811 2Documento16 páginas811 2almightyx10Ainda não há avaliações
- VTR 214 PDFDocumento2 páginasVTR 214 PDFKimberly AndrzejewskiAinda não há avaliações
- Danish Mask StudyDocumento1 páginaDanish Mask StudyJuana AtkinsAinda não há avaliações
- 4 Fundamentals of Health Services ManagementDocumento23 páginas4 Fundamentals of Health Services ManagementMayom Mabuong100% (6)
- Bell 2015Documento5 páginasBell 2015Afien MuktiAinda não há avaliações
- Introduction To HemostasisDocumento16 páginasIntroduction To HemostasisRaiza RuizAinda não há avaliações
- When Are Focused Assessments ConductedDocumento26 páginasWhen Are Focused Assessments ConductedNozomi YukiAinda não há avaliações
- Nonoperative Management of Femoroacetabular ImpingementDocumento8 páginasNonoperative Management of Femoroacetabular ImpingementRodrigo SantosAinda não há avaliações
- UBYT 2019 Yılı Dergi - ListesiDocumento904 páginasUBYT 2019 Yılı Dergi - ListesicemalAinda não há avaliações
- Fixation of Mandibular Fractures With 2.0 MM MiniplatesDocumento7 páginasFixation of Mandibular Fractures With 2.0 MM MiniplatesRajan KarmakarAinda não há avaliações
- 1-Diabetes Package - PO2693771771-269Documento6 páginas1-Diabetes Package - PO2693771771-269KishoreAinda não há avaliações
- Ectopic Pregnancy (m104)Documento13 páginasEctopic Pregnancy (m104)Alphine DalgoAinda não há avaliações
- Pes Planus Concept MapDocumento2 páginasPes Planus Concept MapVeronica Jean U. TubaonAinda não há avaliações
- Is It Okay To Drink Alcohol On Steroids - Google SearchDocumento1 páginaIs It Okay To Drink Alcohol On Steroids - Google SearchEsin SyurmeliAinda não há avaliações
- CS 5 - Duchenne Muscular Dystrophy - EditedDocumento3 páginasCS 5 - Duchenne Muscular Dystrophy - EditedKarishmaK.Dhanani100% (1)
- Solution Manual For Fordneys Medical Insurance 15th Edition Linda SmithDocumento24 páginasSolution Manual For Fordneys Medical Insurance 15th Edition Linda SmithSarahAlexanderrkcq100% (39)
- Allen Part Pedia CaseDocumento3 páginasAllen Part Pedia CasePaul Michael Baguhin0% (1)
- Factors Affecting The Extent of Compliance of Adolescent Pregnant Mothers On Prenatal Care ServicesDocumento29 páginasFactors Affecting The Extent of Compliance of Adolescent Pregnant Mothers On Prenatal Care ServicesNicole LabradoAinda não há avaliações
- Unit One Vocabulary: 'prɔvidәntDocumento53 páginasUnit One Vocabulary: 'prɔvidәntKhanh Chi NguyenAinda não há avaliações
- Dr. Adarsh Chandra Swami - Anaesthesia Doctor in Mohali - Fortis HealthcareDocumento1 páginaDr. Adarsh Chandra Swami - Anaesthesia Doctor in Mohali - Fortis Healthcarej01scottAinda não há avaliações
- Toxicity Review Natural ProductsDocumento5 páginasToxicity Review Natural Productsamino12451Ainda não há avaliações
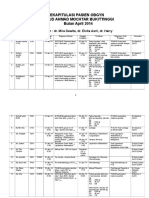
- Rekapitulasi Pasien Obgyn Apr 2014 2Documento20 páginasRekapitulasi Pasien Obgyn Apr 2014 2Ressy Dara AmeliaAinda não há avaliações