Você também pode gostar
- Declaration by The CandidateDocumento39 páginasDeclaration by The CandidateAswathy RCAinda não há avaliações
- NUTRITION ESSENTIALS A Guide For Health ManagersDocumento148 páginasNUTRITION ESSENTIALS A Guide For Health ManagersMatias CAAinda não há avaliações
- Ans2 Research Paper Vitamin ADocumento7 páginasAns2 Research Paper Vitamin Aapi-534404025Ainda não há avaliações
- Vitamin A Deficiency: Diverse Causes, Diverse SolutionsDocumento12 páginasVitamin A Deficiency: Diverse Causes, Diverse SolutionsAviolist AugustavaniaAinda não há avaliações
- VAD ProjectDocumento14 páginasVAD ProjectMr DanielAinda não há avaliações
- Materi MandiriDocumento6 páginasMateri Mandirip17311191006 RANINDYA DWI NOVIYANTIAinda não há avaliações
- Thesis On Vitamin A DeficiencyDocumento8 páginasThesis On Vitamin A DeficiencyLisa Garcia100% (1)
- Cabriadas 2r VadDocumento32 páginasCabriadas 2r VadTintin HonraAinda não há avaliações
- Bioscientific Review (BSR)Documento14 páginasBioscientific Review (BSR)UMT JournalsAinda não há avaliações
- Chapter Two and Three Project Kadpoly 2021Documento33 páginasChapter Two and Three Project Kadpoly 2021dahiru njiddaAinda não há avaliações
- Association Between Vitamin D Status and Undernutrition Indices in Children - A Systematic Review and Meta-Analysis of Observational StudiesDocumento9 páginasAssociation Between Vitamin D Status and Undernutrition Indices in Children - A Systematic Review and Meta-Analysis of Observational StudiesAnggie DiniayuningrumAinda não há avaliações
- Maternal Nutrition & Dietary Awareness in Rural India - Need For Strong Community Supportive MechanismsDocumento3 páginasMaternal Nutrition & Dietary Awareness in Rural India - Need For Strong Community Supportive MechanismsAhmad Jameel QureshiAinda não há avaliações
- Unveiling The Present Landscape of Malnutrition in India: A Comprehensive AssessmentDocumento5 páginasUnveiling The Present Landscape of Malnutrition in India: A Comprehensive AssessmentIJAR JOURNALAinda não há avaliações
- Chapter 2Documento7 páginasChapter 2Mick MickeyAinda não há avaliações
- Ayesha Ishtiaq BS HND 2021-033 (M) Section BDocumento13 páginasAyesha Ishtiaq BS HND 2021-033 (M) Section BAyesha IshtiaqAinda não há avaliações
- Vitamin K 11 21 16Documento13 páginasVitamin K 11 21 16api-345397204Ainda não há avaliações
- Title Defense: MembersDocumento19 páginasTitle Defense: MembersCharlotteAinda não há avaliações
- StuntingDocumento9 páginasStuntingtasyaAinda não há avaliações
- Chapter TwoDocumento12 páginasChapter TwoMuhd SaniAinda não há avaliações
- A Review of Stunting Growth in Children: Relationship To The Incidence of Dental Caries and Its Handling in ChildrenDocumento6 páginasA Review of Stunting Growth in Children: Relationship To The Incidence of Dental Caries and Its Handling in Childrenenda markusAinda não há avaliações
- CH - RH MergedDocumento753 páginasCH - RH MergedAneela KhanAinda não há avaliações
- ERLINFRISKA 2006505505 TheUtilizationofAndroid-BasedApplicationasaStuntingPreventionDocumento11 páginasERLINFRISKA 2006505505 TheUtilizationofAndroid-BasedApplicationasaStuntingPreventioninidurinidAinda não há avaliações
- Building A Prediction Model FoDocumento9 páginasBuilding A Prediction Model Fosyukrianti syahdaAinda não há avaliações
- Prevalence of Vitamin A Deficiency in South Asia: Causes, Outcomes, and Possible RemediesDocumento11 páginasPrevalence of Vitamin A Deficiency in South Asia: Causes, Outcomes, and Possible RemediesDhimas Ihza MahendraAinda não há avaliações
- MalnutritionDocumento7 páginasMalnutritionapurvaapurva100% (1)
- Ebiomedicine: Research PaperDocumento7 páginasEbiomedicine: Research PaperSri Widia NingsihAinda não há avaliações
- Anaemia Policy BriefDocumento7 páginasAnaemia Policy BriefAini DjunetAinda não há avaliações
- Nutritional Status of Children in India and SDGSDocumento7 páginasNutritional Status of Children in India and SDGSInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Factors Related To Stunting in Toddlers: 1 Indanah Kudus, Indonesia Indanah@umkudus - Ac.id 2 Ratna Dewi J Kudus, IndonesiaDocumento5 páginasFactors Related To Stunting in Toddlers: 1 Indanah Kudus, Indonesia Indanah@umkudus - Ac.id 2 Ratna Dewi J Kudus, Indonesiasitii nurlelaAinda não há avaliações
- Jurnal Defisiensi Vitamin ADocumento16 páginasJurnal Defisiensi Vitamin AAdlia Ulfa SyafiraAinda não há avaliações
- Albumin and Serum Vitamin A Status of Malnourished ChildrenDocumento6 páginasAlbumin and Serum Vitamin A Status of Malnourished ChildrenVidinikusumaAinda não há avaliações
- 782Documento20 páginas782Aarathi raoAinda não há avaliações
- POSHAN Abhiyaan: Fighting Malnutrition in The Time of A PandemicDocumento17 páginasPOSHAN Abhiyaan: Fighting Malnutrition in The Time of A PandemicBijay Kumar MahatoAinda não há avaliações
- Anam Khan - E163Documento13 páginasAnam Khan - E163jacacomarketingAinda não há avaliações
- Who NMH NHD 14.4 EngDocumento8 páginasWho NMH NHD 14.4 EngFahriah AsniarAinda não há avaliações
- Chapter One 1.1 Background To The StudyDocumento33 páginasChapter One 1.1 Background To The StudyTajudeen AdegbenroAinda não há avaliações
- Vitamin-A Deficiency and Its Determinants Among PRDocumento9 páginasVitamin-A Deficiency and Its Determinants Among PRaizah afifaturAinda não há avaliações
- Factors Related To Stunting in Toddlers: 1 Indanah 2 Ratna Dewi JDocumento4 páginasFactors Related To Stunting in Toddlers: 1 Indanah 2 Ratna Dewi Jsanita putriAinda não há avaliações
- 341 Nutrient Deficiency or Disease: Definition/Cut-off ValueDocumento7 páginas341 Nutrient Deficiency or Disease: Definition/Cut-off ValueTariqAinda não há avaliações
- Navigating The Clinical Landscape of Severe Acute Malnutrition in India's Pediatric DemographicDocumento10 páginasNavigating The Clinical Landscape of Severe Acute Malnutrition in India's Pediatric DemographicInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Malnutrition: The Crisis of Malnutrition in IndiaDocumento5 páginasMalnutrition: The Crisis of Malnutrition in IndiaDane PukhomaiAinda não há avaliações
- Micronutrient Program - Department of HealthDocumento3 páginasMicronutrient Program - Department of HealthMelvin MarzanAinda não há avaliações
- Meeting Nutritional Needs Through School FeedingDocumento40 páginasMeeting Nutritional Needs Through School Feedingjmn_0905Ainda não há avaliações
- Vitamin b12 ThesisDocumento4 páginasVitamin b12 ThesisSomeoneToWriteMyPaperForMeNewark100% (3)
- Micronutrient ThesisDocumento4 páginasMicronutrient Thesisabdiqadir ali adanAinda não há avaliações
- Chapter: OneDocumento44 páginasChapter: OneCare 101Ainda não há avaliações
- Children 10 00695Documento16 páginasChildren 10 00695BBD BBDAinda não há avaliações
- The Causes and Effect of Maknutrition Among Children at Tudun Wada in Makarfi Local Government Area of Kaduna State.Documento47 páginasThe Causes and Effect of Maknutrition Among Children at Tudun Wada in Makarfi Local Government Area of Kaduna State.YUSUF AMINUAinda não há avaliações
- Who NMH NHD 14.3 EngDocumento12 páginasWho NMH NHD 14.3 EngHanny Hernadha Putri DharmawanAinda não há avaliações
- WHO NMH NHD 14.3 EngDocumento14 páginasWHO NMH NHD 14.3 EngizzaaaaawAinda não há avaliações
- Ijret20140306114 PDFDocumento7 páginasIjret20140306114 PDFYolanda SimamoraAinda não há avaliações
- Berger. Et - Al 2008Documento8 páginasBerger. Et - Al 2008Trianto Budi UtamaAinda não há avaliações
- 543-Original Article-3692-1-10-20211219 - TerbitDocumento11 páginas543-Original Article-3692-1-10-20211219 - TerbitAtik PramestiAinda não há avaliações
- Strengthening Peer Educator On Mother's Knowledge and Attitudes of Stunting in Ogan Komering Ilir RegencyDocumento7 páginasStrengthening Peer Educator On Mother's Knowledge and Attitudes of Stunting in Ogan Komering Ilir RegencyIts4peopleAinda não há avaliações
- The Global Alliance For Vitamin A (GAVA) : Strategic Plan 2016-2020Documento20 páginasThe Global Alliance For Vitamin A (GAVA) : Strategic Plan 2016-2020MohammedAinda não há avaliações
- Akhtar S Et Al., 2013. Micronutrient Deficiencies in South AsiaDocumento8 páginasAkhtar S Et Al., 2013. Micronutrient Deficiencies in South AsiaAtulAinda não há avaliações
- Monica Ironsuppl FrontiersDocumento10 páginasMonica Ironsuppl FrontiersPia GayyaAinda não há avaliações
- Micronutrient Status of Indian Population.7Documento11 páginasMicronutrient Status of Indian Population.7Nishita SuratkalAinda não há avaliações
- User's Guide to Eye Health Supplements: Learn All about the Nutritional Supplements That Can Save Your VisionNo EverandUser's Guide to Eye Health Supplements: Learn All about the Nutritional Supplements That Can Save Your VisionNota: 5 de 5 estrelas5/5 (1)
- Breastfeeding and vitamin D supplementation: Do you need it?No EverandBreastfeeding and vitamin D supplementation: Do you need it?Ainda não há avaliações
- Theodore Henry Shackleford - My Country and Other PoemsDocumento246 páginasTheodore Henry Shackleford - My Country and Other Poemschyoung0% (1)
- Fruit Logistica Trend Report 2018 Part1Documento19 páginasFruit Logistica Trend Report 2018 Part1Jesu Gajardo OrósticaAinda não há avaliações
- Transcript of Let's Master English's Podcast Episode 1 PDFDocumento4 páginasTranscript of Let's Master English's Podcast Episode 1 PDFJulieta VillanuevaAinda não há avaliações
- Action Plan Gift GivingDocumento5 páginasAction Plan Gift GivingAnnie Lyn De ErioAinda não há avaliações
- Tutorial Wedge Shoe Cake by Sugar & Spice CakesDocumento51 páginasTutorial Wedge Shoe Cake by Sugar & Spice Cakesacdnadmin75% (4)
- Past Perfect Tense Past Perfect Continuous 3Documento4 páginasPast Perfect Tense Past Perfect Continuous 3Mau Diaz0% (1)
- TerrestrialDocumento19 páginasTerrestrialdebanjanr262Ainda não há avaliações
- Avocado Oil Refined Tx008222 PdsDocumento3 páginasAvocado Oil Refined Tx008222 Pdskwamina20Ainda não há avaliações
- Consumer Perception About Fastfood Centres in AsabaDocumento8 páginasConsumer Perception About Fastfood Centres in AsabaOpia AnthonyAinda não há avaliações
- Study Guide Cookery NC 2Documento7 páginasStudy Guide Cookery NC 2FRANCIS D. SACROAinda não há avaliações
- Budget of WorkDocumento18 páginasBudget of WorkCicille Grace Alajeño CayabyabAinda não há avaliações
- Batna BasicsDocumento43 páginasBatna BasicsPrabina ShakyaAinda não há avaliações
- Snow White and The Seven DwarfsDocumento15 páginasSnow White and The Seven DwarfsLê Đình TrungAinda não há avaliações
- At The Farm 16Documento18 páginasAt The Farm 16api-677034951Ainda não há avaliações
- Bahrain New Regulation For Medical DeviceDocumento2 páginasBahrain New Regulation For Medical Devicegulafsha1Ainda não há avaliações
- 11 - 19, 21-23, 24-25, 27Documento8 páginas11 - 19, 21-23, 24-25, 27Guile PTAinda não há avaliações
- The Vice Busting DIET - Julia HaveyDocumento237 páginasThe Vice Busting DIET - Julia HaveyCristiVlad100% (1)
- Good Gov Social Res. Module 9Documento5 páginasGood Gov Social Res. Module 9Sofia T. OlbesAinda não há avaliações
- Times Leader 12-04-2011Documento88 páginasTimes Leader 12-04-2011The Times LeaderAinda não há avaliações
- 1 2+PATHFI1+HandoutDocumento10 páginas1 2+PATHFI1+HandoutDonna Aizel MagbujosAinda não há avaliações
- Philippine Council For Agriculture and Fisheries Agricultural and Fishery Council ProfileDocumento2 páginasPhilippine Council For Agriculture and Fisheries Agricultural and Fishery Council ProfileRio Vic Aguilar GeronAinda não há avaliações
- The Nether Better Upgrade ManualDocumento24 páginasThe Nether Better Upgrade ManualJosue Mejia100% (1)
- MPUDocumento5 páginasMPU威陈Ainda não há avaliações
- Parent HandbookDocumento24 páginasParent Handbookapi-295769704Ainda não há avaliações
- Section2 1Documento13 páginasSection2 1JessicaAinda não há avaliações
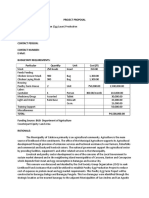
- Egg Layer ProposalDocumento3 páginasEgg Layer ProposalCoronwokers Homebase94% (16)
- Bad Ac Action PlanDocumento5 páginasBad Ac Action PlanCamille Kristine Dionisio100% (7)
- Final Case StudyDocumento18 páginasFinal Case Studyapi-487702467100% (1)
- Manipur State InformationDocumento3 páginasManipur State InformationCHAITANYA SIVAAinda não há avaliações
- Chemistry Project CHIRANJIBIDocumento18 páginasChemistry Project CHIRANJIBIKrìsHna BäskēyAinda não há avaliações