Você também pode gostar
- RVOT Stenting in TOF PatientDocumento31 páginasRVOT Stenting in TOF PatientHannaTashiaClaudiaAinda não há avaliações
- Transposition of Great ArteriesDocumento21 páginasTransposition of Great ArteriesAlusio Navosailagi VUNIIVI100% (1)
- Modi Fied Blalock Taussig Shunt: A Not-So-Simple Palliative ProcedureDocumento7 páginasModi Fied Blalock Taussig Shunt: A Not-So-Simple Palliative ProcedureJakler NicheleAinda não há avaliações
- High Versus Normal Blood Pressure Targets in Relation To Right Ventricular Dysfunction After Cardiac Surgery: A Randomized Controlled TrialDocumento11 páginasHigh Versus Normal Blood Pressure Targets in Relation To Right Ventricular Dysfunction After Cardiac Surgery: A Randomized Controlled TrialDina RyantiAinda não há avaliações
- AritmiaDocumento9 páginasAritmiaDayuKurnia DewantiAinda não há avaliações
- Review Article: Bedside Ultrasound in Resuscitation and The Rapid Ultrasound in Shock ProtocolDocumento14 páginasReview Article: Bedside Ultrasound in Resuscitation and The Rapid Ultrasound in Shock ProtocolClaudioValdiviaAinda não há avaliações
- Obesity in Patient with VSD and Pulmonary HypertensionDocumento8 páginasObesity in Patient with VSD and Pulmonary HypertensionDr AnitaHsParewasiAinda não há avaliações
- Case Report Cteph EditDocumento13 páginasCase Report Cteph EditapekzzzzAinda não há avaliações
- Down Syndrome: Case ReportsDocumento4 páginasDown Syndrome: Case ReportsPedro CardosoAinda não há avaliações
- 1 SMDocumento6 páginas1 SMAditya NobelAinda não há avaliações
- AAFP Board Review ClinchersDocumento53 páginasAAFP Board Review ClinchersJessica E Isom100% (2)
- Case ReportDocumento4 páginasCase ReportStella RAinda não há avaliações
- 2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathyDocumento9 páginas2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathybanupluAinda não há avaliações
- OutDocumento4 páginasOutMaria Zarah MenesesAinda não há avaliações
- 朱家权氯沙坦猪模型Documento10 páginas朱家权氯沙坦猪模型shentujin1997Ainda não há avaliações
- Journal of Nursing: Basic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest RadiographyDocumento8 páginasJournal of Nursing: Basic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest RadiographyNiala AlmarioAinda não há avaliações
- Insuficiencia Por EndocarditisDocumento4 páginasInsuficiencia Por EndocarditisKatherin TorresAinda não há avaliações
- Cardiogenic Shock: Physical FindingsDocumento9 páginasCardiogenic Shock: Physical FindingsEduardo Perez GonzalezAinda não há avaliações
- SEHGAL 2016 - A New Look at Bronchopulmonary Dysplasia - Post Capillary Pathophysiology and Cardiac DysfunctionDocumento8 páginasSEHGAL 2016 - A New Look at Bronchopulmonary Dysplasia - Post Capillary Pathophysiology and Cardiac DysfunctionRafael JustinoAinda não há avaliações
- PulmCirc 005 407Documento5 páginasPulmCirc 005 407Andreea KAinda não há avaliações
- Pulmonary EmbolismDocumento5 páginasPulmonary EmbolismNica Duco100% (2)
- Heart MurmurDocumento6 páginasHeart MurmurYogendran MAinda não há avaliações
- Basic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest RadiographyDocumento7 páginasBasic Cardiac Assessments: Physical Examination, Electrocardiography, and Chest Radiographyrowd1yAinda não há avaliações
- Art 11Documento6 páginasArt 11Andreea Raluca CimpoiAinda não há avaliações
- Tetralogy of FallotDocumento5 páginasTetralogy of FallotSaloni MehtaAinda não há avaliações
- Jurnal Internasional Peb Nifas 5Documento10 páginasJurnal Internasional Peb Nifas 5Herdian KurniawanAinda não há avaliações
- Article 1Documento4 páginasArticle 1Fakhar Mahmood ShahidAinda não há avaliações
- Amniotic Fluid EmbolismDocumento30 páginasAmniotic Fluid EmbolismDonmer Ibañez Juan100% (1)
- Category 1) Pulmonary Hypertension Diagnosis and Treatment of Secondary (NonDocumento11 páginasCategory 1) Pulmonary Hypertension Diagnosis and Treatment of Secondary (NonAmit GoelAinda não há avaliações
- Eisenmenger SyndromeDocumento41 páginasEisenmenger SyndromeJennifer DixonAinda não há avaliações
- Cardiac RadiologyDocumento10 páginasCardiac RadiologyHaluk AlibazogluAinda não há avaliações
- Transesophageal Echocardiography: The Hemodynamic Monitoring UtilizingDocumento14 páginasTransesophageal Echocardiography: The Hemodynamic Monitoring UtilizingvegasbabyAinda não há avaliações
- Pancytopenia in A Surgical Patient, A Rare Presentation of HyperthyroidismDocumento3 páginasPancytopenia in A Surgical Patient, A Rare Presentation of HyperthyroidismIdaamsiyatiAinda não há avaliações
- Transposition of Great ArteriesDocumento18 páginasTransposition of Great Arteriesparmeshori100% (2)
- Current Management of Infants and Children With Single Ventricle AnatomyDocumento13 páginasCurrent Management of Infants and Children With Single Ventricle AnatomyjahangirealamAinda não há avaliações
- Hypoplastic Left Heart SyndromeDocumento13 páginasHypoplastic Left Heart SyndromeYaser AlmafrajiAinda não há avaliações
- 2021 Chowdhury AW - A Rare Combination of Complex Congenital HeartDocumento4 páginas2021 Chowdhury AW - A Rare Combination of Complex Congenital HeartPratyay HasanAinda não há avaliações
- The Effect of Cilostazol On Right Heart FunctionDocumento43 páginasThe Effect of Cilostazol On Right Heart FunctionGunawan YogaAinda não há avaliações
- Mksap 17 MCQ FullDocumento282 páginasMksap 17 MCQ Fullfermann100% (1)
- Case Report Missed Connections: Identification of Atrial Septal Defect by MRIDocumento4 páginasCase Report Missed Connections: Identification of Atrial Septal Defect by MRIMuhammad Nur Ardhi LahabuAinda não há avaliações
- Assessment of Pulse Transit Time To Indicate Cardiovascular Changes During Obstetric Spinal AnaesthesiaDocumento6 páginasAssessment of Pulse Transit Time To Indicate Cardiovascular Changes During Obstetric Spinal AnaesthesiaprabuAinda não há avaliações
- Management of Tetralogy of FallotDocumento45 páginasManagement of Tetralogy of FallotAditya MadhavpeddiAinda não há avaliações
- Order ID 3416232.edited - EditedDocumento5 páginasOrder ID 3416232.edited - Editedngunyijohn001Ainda não há avaliações
- Congestive Heart Failure/Pulmonary Edema Case FileDocumento4 páginasCongestive Heart Failure/Pulmonary Edema Case Filehttps://medical-phd.blogspot.comAinda não há avaliações
- Transesophageal Echocardiography For The Noncardiac Surgical PatientDocumento13 páginasTransesophageal Echocardiography For The Noncardiac Surgical PatientSindhuNugrohoMuktiAinda não há avaliações
- Poster Presentation CCRA Malang 2014Documento3 páginasPoster Presentation CCRA Malang 2014alfarobi yogiAinda não há avaliações
- Left Atrial Expansion Index Predicts All-Cause Mortality and Heart Failure Admissions in DyspnoeaDocumento8 páginasLeft Atrial Expansion Index Predicts All-Cause Mortality and Heart Failure Admissions in DyspnoeaMathew McCarthyAinda não há avaliações
- A Case of Benign, Multiple MetastasesDocumento2 páginasA Case of Benign, Multiple MetastasesCesar Antonio Ulloa BarbaranAinda não há avaliações
- Pacemaker Related RHFDocumento4 páginasPacemaker Related RHFFaQihuddin AhmadAinda não há avaliações
- Venous Air Embolism During Anterior Lumbar Surgery: Case ReportDocumento3 páginasVenous Air Embolism During Anterior Lumbar Surgery: Case ReportFika Khulma SofiaAinda não há avaliações
- ST 1Documento6 páginasST 1sserggiosAinda não há avaliações
- Hipertrofia VD en HTADocumento8 páginasHipertrofia VD en HTAgustavo reyesAinda não há avaliações
- Corazon y SojenDocumento7 páginasCorazon y Sojenmaria cristina aravenaAinda não há avaliações
- Transposition of The Great Arteries PDFDocumento6 páginasTransposition of The Great Arteries PDFSakuntalaPalanki100% (2)
- Patent Ductus Arteriosus Stenting For Palliation of Severe Pulmonary Arterial Hypertension in ChildhoodDocumento5 páginasPatent Ductus Arteriosus Stenting For Palliation of Severe Pulmonary Arterial Hypertension in ChildhoodEffendi TanAinda não há avaliações
- Jurnal 5Documento6 páginasJurnal 5Siti rahmi AbukhaerAinda não há avaliações
- Introduction: A 45-Year-Old Female With A Long Time History of CardiovascularDocumento1 páginaIntroduction: A 45-Year-Old Female With A Long Time History of CardiovascularCalin CraciunAinda não há avaliações
- Assignment 4 MHPPDocumento11 páginasAssignment 4 MHPPBabar AliAinda não há avaliações
- Bronchial AsthmaDocumento3 páginasBronchial AsthmaSabrina Reyes0% (1)
- Screening For Microalbuminuria in Patients With Diabetes: How? Why?Documento2 páginasScreening For Microalbuminuria in Patients With Diabetes: How? Why?Abhishek SenAinda não há avaliações
- 1 Florendo Vs Philam PlansDocumento6 páginas1 Florendo Vs Philam PlansRon GamboaAinda não há avaliações
- Idea DisabilitiesDocumento6 páginasIdea Disabilitiesapi-425284294Ainda não há avaliações
- SuctioningDocumento23 páginasSuctioningrnrmmanphd100% (2)
- Questionnaire AnemiaDocumento1 páginaQuestionnaire AnemiaYanuar Adi Pranata50% (2)
- Captopril Sublingual Vs OralDocumento8 páginasCaptopril Sublingual Vs OralTa RaAinda não há avaliações
- Last Look Nephrology & Rheumatology (Medicine Must Know)Documento43 páginasLast Look Nephrology & Rheumatology (Medicine Must Know)rohankananiAinda não há avaliações
- Test Bank For Essentials of Pediatric Nursing 2nd Edition Theresa KyleDocumento13 páginasTest Bank For Essentials of Pediatric Nursing 2nd Edition Theresa KyleJamesJacksonjbpof100% (76)
- Elstrott 2019Documento9 páginasElstrott 2019Aurha Akmal GinarisAinda não há avaliações
- Growing in Vitro Diagnostics (IVD) Market To Set New Business Opportunities For Start Up CompanyDocumento2 páginasGrowing in Vitro Diagnostics (IVD) Market To Set New Business Opportunities For Start Up CompanyPR.comAinda não há avaliações
- Chicken Pox SOAPDocumento8 páginasChicken Pox SOAPKevin NyasogoAinda não há avaliações
- American Thoracic Society Cigarette Smoking and Health 2Documento5 páginasAmerican Thoracic Society Cigarette Smoking and Health 2miftahul masruriAinda não há avaliações
- Spinal Cord Injuries and SyndromeDocumento18 páginasSpinal Cord Injuries and SyndromeKim Sunoo100% (1)
- Pathology CVS #5 by Omar BaniErshaidDocumento5 páginasPathology CVS #5 by Omar BaniErshaidبصيص اليقينAinda não há avaliações
- ERPM Viva Long Cases III v2.0Documento17 páginasERPM Viva Long Cases III v2.0Bhagya Pramodh AriyarathnaAinda não há avaliações
- Fine Tuning the Nutrition Care ProcessDocumento13 páginasFine Tuning the Nutrition Care ProcessRacquel Jahn CorderoAinda não há avaliações
- Qasida Tuba Qaseeda Tooba Shaykh Musa Ruhani Al BaziDocumento33 páginasQasida Tuba Qaseeda Tooba Shaykh Musa Ruhani Al BaziYakoob Mahomed Perfume House67% (3)
- Preoperative Testing and Medication ManagementDocumento27 páginasPreoperative Testing and Medication ManagementWidya JelitaAinda não há avaliações
- Policies To Promote Child Health 25 Full JournalDocumento204 páginasPolicies To Promote Child Health 25 Full JournalDiksha DuhanAinda não há avaliações
- 7 Uses For Medical MarijuanaDocumento4 páginas7 Uses For Medical MarijuanaYhojan Surco ZavalaAinda não há avaliações
- HSN101Documento3 páginasHSN101Raha RajabigamasaeiAinda não há avaliações
- Discuss What Resources Are Often Necessary For Nonacute Care For Cardiorespiratory IssuesDocumento2 páginasDiscuss What Resources Are Often Necessary For Nonacute Care For Cardiorespiratory IssuesBettAinda não há avaliações
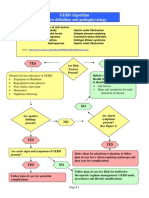
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocumento3 páginasGERD Algorithm Review Definition and Pathophysiology: NO YESdianyAinda não há avaliações
- MP SuccessfulPersonalTrainerDocumento14 páginasMP SuccessfulPersonalTrainerAnthony Dinicolantonio100% (1)
- Epidemiology - Exercises. Gaetano MarroneDocumento4 páginasEpidemiology - Exercises. Gaetano Marronemillion assefaAinda não há avaliações
- Raji Tribe11Documento12 páginasRaji Tribe11Keya PandeyAinda não há avaliações
- Non-Plaque Induced GingivitisDocumento30 páginasNon-Plaque Induced GingivitisDentist AymanAinda não há avaliações
- Notes On History Taking in The Cardiovascular SystemDocumento9 páginasNotes On History Taking in The Cardiovascular Systemmdjohar72100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 3.5 de 5 estrelas3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNo EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNota: 4 de 5 estrelas4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeAinda não há avaliações
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 3.5 de 5 estrelas3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementNo EverandTechniques Exercises And Tricks For Memory ImprovementNota: 4.5 de 5 estrelas4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 5 de 5 estrelas5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesNo EverandThe Ultimate Guide To Memory Improvement TechniquesNota: 5 de 5 estrelas5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNo EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNota: 5 de 5 estrelas5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNo EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNota: 5 de 5 estrelas5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNo EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNota: 3.5 de 5 estrelas3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisNo EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisNota: 5 de 5 estrelas5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingNo EverandThe Happiness Trap: How to Stop Struggling and Start LivingNota: 4 de 5 estrelas4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsAinda não há avaliações
- The Tennis Partner: A Doctor's Story of Friendship and LossNo EverandThe Tennis Partner: A Doctor's Story of Friendship and LossNota: 4.5 de 5 estrelas4.5/5 (4)