Você também pode gostar
- Renal Lab Report FinalDocumento12 páginasRenal Lab Report Finalapi-437387942Ainda não há avaliações
- Kidney Regulation of Osmolarity - How the Kidneys Control Salt and Water LevelsDocumento4 páginasKidney Regulation of Osmolarity - How the Kidneys Control Salt and Water LevelsYoyo WuAinda não há avaliações
- 2003 - Rapid Water and Slow Sodium Excretion of Acetated Ringer in Cellular SwellingDocumento5 páginas2003 - Rapid Water and Slow Sodium Excretion of Acetated Ringer in Cellular Swellingmarco marcoAinda não há avaliações
- Water Balance in Human (Report)Documento4 páginasWater Balance in Human (Report)Syairah87Ainda não há avaliações
- Lab Exercise 8 Kidney Function and UrinalysisDocumento11 páginasLab Exercise 8 Kidney Function and UrinalysisJoseline SorianoAinda não há avaliações
- AssignmentDocumento6 páginasAssignmentleone shikukuAinda não há avaliações
- Fluidoterapia altera parâmetros hematológicos e urinários em cãesDocumento7 páginasFluidoterapia altera parâmetros hematológicos e urinários em cãesLucas AugustoAinda não há avaliações
- Evaluation of DiureticsDocumento56 páginasEvaluation of DiureticsPonkiya AnkitAinda não há avaliações
- JGLG TLA2 Refelective WritingDocumento3 páginasJGLG TLA2 Refelective WritingJunnin Gay GarayAinda não há avaliações
- Ranal SystemDocumento35 páginasRanal SystemAdil IrshadAinda não há avaliações
- Effects of Varying Alcohol Concentration On Cellular Respiration of Mouse (MusDocumento10 páginasEffects of Varying Alcohol Concentration On Cellular Respiration of Mouse (MusShannen SenaAinda não há avaliações
- Osmoregulation in Earthworms ExplainedDocumento28 páginasOsmoregulation in Earthworms ExplainedMa-anJaneDiamosAinda não há avaliações
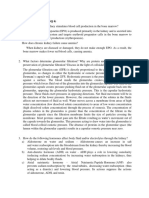
- Nutritional Physiology Study Question 6Documento3 páginasNutritional Physiology Study Question 6Julie Amor ZantuaAinda não há avaliações
- Fluid, Electrolyte, and Acid-Base BalanceDocumento41 páginasFluid, Electrolyte, and Acid-Base BalanceRn nadeenAinda não há avaliações
- Specific Gravity and Chloride Concentration Volume, Acidity, Specific Gravity and Chloride ConcentrationDocumento11 páginasSpecific Gravity and Chloride Concentration Volume, Acidity, Specific Gravity and Chloride ConcentrationOlyver SangAinda não há avaliações
- Fluid Volume BalanceDocumento73 páginasFluid Volume BalanceSalman HabeebAinda não há avaliações
- Minister of Health Kafue College of Nursing and Midwifery Public Health NursingDocumento9 páginasMinister of Health Kafue College of Nursing and Midwifery Public Health NursingLawrence Favor SilungweAinda não há avaliações
- Fluid and Electrolyte BalanceDocumento3 páginasFluid and Electrolyte BalancejalajaraniAinda não há avaliações
- Study Guide 2Documento34 páginasStudy Guide 2api-260095216Ainda não há avaliações
- Surmacz Regulation of Fluid and Electrolyte Balance1Documento20 páginasSurmacz Regulation of Fluid and Electrolyte Balance1leone shikukuAinda não há avaliações
- Lab Activity EditDocumento4 páginasLab Activity EditBryanAinda não há avaliações
- Module 2 Fluid Electrolyte Disorders Acid Base Notes 9th EdDocumento15 páginasModule 2 Fluid Electrolyte Disorders Acid Base Notes 9th EdSara FAinda não há avaliações
- Anesthetic Efficacy of Clove Oil and Its Impact On Hematological and Biochemical Changes in Channa Striatus (Bloch, 1793)Documento9 páginasAnesthetic Efficacy of Clove Oil and Its Impact On Hematological and Biochemical Changes in Channa Striatus (Bloch, 1793)researchinbiologyAinda não há avaliações
- Basic of Fluid Therapy ImaDocumento69 páginasBasic of Fluid Therapy Imal Made ArtawanAinda não há avaliações
- Effects of Sugar on Urine ParametersDocumento19 páginasEffects of Sugar on Urine ParametersdktkaAinda não há avaliações
- Iv FluidsDocumento6 páginasIv FluidsCrishara PalomoAinda não há avaliações
- METABOLISME AIRDocumento15 páginasMETABOLISME AIRAyu FadhilahAinda não há avaliações
- Dileep N. LOBO, Zeno STANGA, J. Alastair D. SIMPSON, John A. ANDERSON, Brian J. ROWLANDS and Simon P. ALLISONDocumento7 páginasDileep N. LOBO, Zeno STANGA, J. Alastair D. SIMPSON, John A. ANDERSON, Brian J. ROWLANDS and Simon P. ALLISONMaria De Los AngelesAinda não há avaliações
- Mechanism of Urine FormationDocumento5 páginasMechanism of Urine FormationovacuteAinda não há avaliações
- Order 678392 Summary and Analyze Experiment DataDocumento9 páginasOrder 678392 Summary and Analyze Experiment DatatuluAinda não há avaliações
- Practical OsmorelulationDocumento37 páginasPractical OsmorelulationDinaAinda não há avaliações
- Consumption of Low Tds Water: A Committee Report BY Water Quality Association Science Advisory Committee 1992-1993Documento13 páginasConsumption of Low Tds Water: A Committee Report BY Water Quality Association Science Advisory Committee 1992-1993nurhuda majidAinda não há avaliações
- Fluids, electrolytes and acid-base balanceDocumento13 páginasFluids, electrolytes and acid-base balanceMansoor TariqAinda não há avaliações
- Osmosis Lab DiscussionDocumento2 páginasOsmosis Lab Discussionsoha zubairAinda não há avaliações
- METABOLISME AIR DAN MINERALDocumento15 páginasMETABOLISME AIR DAN MINERALKlara SintaAinda não há avaliações
- 25.9 Regulation of Fluid Volume and Composition - Anatomy and Physiology 2e - OpenStaxDocumento4 páginas25.9 Regulation of Fluid Volume and Composition - Anatomy and Physiology 2e - OpenStaxMarlene AngwaforAinda não há avaliações
- Lab ReportDocumento5 páginasLab ReportPauline Mae RoquidAinda não há avaliações
- HomeostasisDocumento4 páginasHomeostasisJoAinda não há avaliações
- Fluid Electrolyte BalanceDocumento19 páginasFluid Electrolyte BalanceRatna VimalAinda não há avaliações
- Ii. Hydroelectrolytic Imbalance PDFDocumento30 páginasIi. Hydroelectrolytic Imbalance PDFIvanes IgorAinda não há avaliações
- IV Therapy 2 PDFDocumento132 páginasIV Therapy 2 PDFJulie May SuganobAinda não há avaliações
- Role of Kidney in Salt and Water HomeostasisDocumento31 páginasRole of Kidney in Salt and Water HomeostasisHakimah K. Suhaimi100% (1)
- Lect 02Documento5 páginasLect 02Iptysam Al-AlawiAinda não há avaliações
- Hormones: ADH and Diabetes InsipidusDocumento10 páginasHormones: ADH and Diabetes InsipidusAnanyaAinda não há avaliações
- Body FluidsDocumento59 páginasBody FluidsAmmar SmadiAinda não há avaliações
- Water Balance Laboratory HandoutDocumento8 páginasWater Balance Laboratory HandoutTheng.SethAinda não há avaliações
- UrineDocumento15 páginasUrineTheophilus Offei DarkoAinda não há avaliações
- Consumption of Low Tds Water: Established Drinking Water StandardsDocumento7 páginasConsumption of Low Tds Water: Established Drinking Water Standardsadeelyaseen1Ainda não há avaliações
- Urine Serum Ratio To Predict Response To Fluid RestrictionDocumento8 páginasUrine Serum Ratio To Predict Response To Fluid Restrictionkromatin9462Ainda não há avaliações
- Fluids and Electrolytes A Fast and Easy Way To Understand Acid-Base Balance Without MemorizationDocumento195 páginasFluids and Electrolytes A Fast and Easy Way To Understand Acid-Base Balance Without MemorizationNayely MoralesAinda não há avaliações
- Flluid and ElectDocumento107 páginasFlluid and ElectHassan SalamehAinda não há avaliações
- Hyperglycemia Hyponatremia Osmolarity CalculationDocumento4 páginasHyperglycemia Hyponatremia Osmolarity CalculationduhsknwsAinda não há avaliações
- Fluids, Electrolytes, and Acid-Base HomeostasisDocumento9 páginasFluids, Electrolytes, and Acid-Base HomeostasisaclumutAinda não há avaliações
- Nursing Fluids and ElectrolytesDocumento14 páginasNursing Fluids and Electrolytesaga1028100% (18)
- Fluid and Electrolytes for Nursing StudentsNo EverandFluid and Electrolytes for Nursing StudentsNota: 5 de 5 estrelas5/5 (12)
- The Clinical Biology of Sodium: The Physiology and Pathophysiology of Sodium in MammalsNo EverandThe Clinical Biology of Sodium: The Physiology and Pathophysiology of Sodium in MammalsAinda não há avaliações
- Save Your Life with the Elixir of Water: Becoming pH Balanced in an Unbalanced World: How to Save Your LifeNo EverandSave Your Life with the Elixir of Water: Becoming pH Balanced in an Unbalanced World: How to Save Your LifeNota: 2 de 5 estrelas2/5 (2)
- Evil Days of Luckless JohnDocumento5 páginasEvil Days of Luckless JohnadikressAinda não há avaliações
- N4 Electrotechnics August 2021 MemorandumDocumento8 páginasN4 Electrotechnics August 2021 MemorandumPetro Susan BarnardAinda não há avaliações
- CBSE Class 6 Whole Numbers WorksheetDocumento2 páginasCBSE Class 6 Whole Numbers WorksheetPriyaprasad PandaAinda não há avaliações
- Alternate Tuning Guide: Bill SetharesDocumento96 páginasAlternate Tuning Guide: Bill SetharesPedro de CarvalhoAinda não há avaliações
- Anti Jamming of CdmaDocumento10 páginasAnti Jamming of CdmaVishnupriya_Ma_4804Ainda não há avaliações
- Role of PAODocumento29 páginasRole of PAOAjay DhokeAinda não há avaliações
- A Princess of Mars Part 3Documento4 páginasA Princess of Mars Part 3Sheila Inca100% (1)
- Hipotension 6Documento16 páginasHipotension 6arturo castilloAinda não há avaliações
- Dell Compellent Sc4020 Deploy GuideDocumento184 páginasDell Compellent Sc4020 Deploy Guidetar_py100% (1)
- Use Visual Control So No Problems Are Hidden.: TPS Principle - 7Documento8 páginasUse Visual Control So No Problems Are Hidden.: TPS Principle - 7Oscar PinillosAinda não há avaliações
- Ofper 1 Application For Seagoing AppointmentDocumento4 páginasOfper 1 Application For Seagoing AppointmentNarayana ReddyAinda não há avaliações
- Dermatology Study Guide 2023-IvDocumento7 páginasDermatology Study Guide 2023-IvUnknown ManAinda não há avaliações
- Differential Pulse Code ModulationDocumento12 páginasDifferential Pulse Code ModulationNarasimhareddy MmkAinda não há avaliações
- Pulse Width ModulationDocumento13 páginasPulse Width Modulationhimanshu jainAinda não há avaliações
- SEC QPP Coop TrainingDocumento62 páginasSEC QPP Coop TrainingAbdalelah BagajateAinda não há avaliações
- 2020 Global Finance Business Management Analyst Program - IIMDocumento4 páginas2020 Global Finance Business Management Analyst Program - IIMrishabhaaaAinda não há avaliações
- Guide To Raising Capital From Angel Investors Ebook From The Startup Garage PDFDocumento20 páginasGuide To Raising Capital From Angel Investors Ebook From The Startup Garage PDFLars VonTurboAinda não há avaliações
- Jesd8 15aDocumento22 páginasJesd8 15aSridhar PonnurangamAinda não há avaliações
- Chapter 19 - 20 Continuous Change - Transorganizational ChangeDocumento12 páginasChapter 19 - 20 Continuous Change - Transorganizational ChangeGreen AvatarAinda não há avaliações
- Command List-6Documento3 páginasCommand List-6Carlos ArbelaezAinda não há avaliações
- Statistical Decision AnalysisDocumento3 páginasStatistical Decision AnalysisTewfic SeidAinda não há avaliações
- AtlasConcorde NashDocumento35 páginasAtlasConcorde NashMadalinaAinda não há avaliações
- CFO TagsDocumento95 páginasCFO Tagssatyagodfather0% (1)
- France Winckler Final Rev 1Documento14 páginasFrance Winckler Final Rev 1Luciano Junior100% (1)
- 2018 NAMCYA CHILDREN'S RONDALLA ENSEMBLE GuidelinesDocumento3 páginas2018 NAMCYA CHILDREN'S RONDALLA ENSEMBLE GuidelinesJohn Cedrick JagapeAinda não há avaliações
- Felizardo C. Lipana National High SchoolDocumento3 páginasFelizardo C. Lipana National High SchoolMelody LanuzaAinda não há avaliações
- Bula Defense M14 Operator's ManualDocumento32 páginasBula Defense M14 Operator's ManualmeAinda não há avaliações
- Flowmon Ads Enterprise Userguide enDocumento82 páginasFlowmon Ads Enterprise Userguide ennagasatoAinda não há avaliações
- Weone ProfileDocumento10 páginasWeone ProfileOmair FarooqAinda não há avaliações
- Be It Enacted by The Senate and House of Representatives of The Philippines in Congress AssembledDocumento2 páginasBe It Enacted by The Senate and House of Representatives of The Philippines in Congress AssembledCesar ValeraAinda não há avaliações