Você também pode gostar
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideAinda não há avaliações
- Quick Creole for Medical Personnel: Hope Literature, Haitian Creole Medical PhrasebookNo EverandQuick Creole for Medical Personnel: Hope Literature, Haitian Creole Medical PhrasebookAinda não há avaliações
- Bedside Med HX Maker PDFDocumento2 páginasBedside Med HX Maker PDFjustinryanAinda não há avaliações
- Clinical Paperwork For StudentsDocumento16 páginasClinical Paperwork For StudentsRyanAinda não há avaliações
- RM# Name: RM# Name: Age: Doctor/Consults: Age: Doctor/ConsultsDocumento2 páginasRM# Name: RM# Name: Age: Doctor/Consults: Age: Doctor/Consultsseaturtles505Ainda não há avaliações
- 1 2 Building Health SkillsDocumento4 páginas1 2 Building Health Skillsapi-261782961Ainda não há avaliações
- UKOOADocumento2 páginasUKOOAIsidor Danon100% (3)
- CVA Nursing Case StudyDocumento76 páginasCVA Nursing Case StudyGabriel Apalisok100% (1)
- Official Medical Examination Form (2021 GKS-U)Documento1 páginaOfficial Medical Examination Form (2021 GKS-U)hAinda não há avaliações
- CC: Demo: Hpi: Allergies: Pertinent ROS: Vitals:: LabsDocumento4 páginasCC: Demo: Hpi: Allergies: Pertinent ROS: Vitals:: Labsagrawa03Ainda não há avaliações
- The AMBOSS 100 Day Study Plan - Your No1 Study Guide For Final ExamsDocumento30 páginasThe AMBOSS 100 Day Study Plan - Your No1 Study Guide For Final Examsovermega100% (1)
- Periodontal Flap Surgery Techniques and ConsiderationsDocumento38 páginasPeriodontal Flap Surgery Techniques and ConsiderationsChauhan Naresh100% (1)
- Nursing SheetDocumento1 páginaNursing Sheetseaturtles505100% (1)
- Introduction History and ExaminationDocumento43 páginasIntroduction History and ExaminationDanyal Hassan100% (1)
- Nursing Concept MapDocumento3 páginasNursing Concept MapSheAinda não há avaliações
- Pediatric Clinical H&PDocumento7 páginasPediatric Clinical H&PJay Vee100% (1)
- Octaseeds Rise Review Posttest Compilation 120qDocumento19 páginasOctaseeds Rise Review Posttest Compilation 120qAngela Saldajeno100% (3)
- CSC Proforma - FeverDocumento6 páginasCSC Proforma - Fever127 Shruthik Patel ThotaAinda não há avaliações
- COPD Patient Profile: 73-Year-Old Male TeacherDocumento14 páginasCOPD Patient Profile: 73-Year-Old Male Teacherprashanth100% (1)
- AA Vision and MissionDocumento8 páginasAA Vision and MissionAkshata BansodeAinda não há avaliações
- Antenatal Assessment 18Documento13 páginasAntenatal Assessment 18naga mani100% (1)
- Paediatric History and Examination 08092012-2Documento10 páginasPaediatric History and Examination 08092012-2Shahin KazemzadehAinda não há avaliações
- Toddler Assessment FormDocumento7 páginasToddler Assessment FormBinal Joshi50% (2)
- Pediatric History Taking and Physical ExamDocumento32 páginasPediatric History Taking and Physical ExamCJ Tee100% (1)
- Appendicitis Nursing Care GuideDocumento32 páginasAppendicitis Nursing Care GuideUday Kumar100% (1)
- CSC Proforma - GeneralDocumento6 páginasCSC Proforma - General127 Shruthik Patel ThotaAinda não há avaliações
- Antepartum HemorrhageDocumento3 páginasAntepartum Hemorrhagenur1146Ainda não há avaliações
- Drugs and Tinnitus - Neil Bauman PHD - April '09Documento2 páginasDrugs and Tinnitus - Neil Bauman PHD - April '09DownTheTheRabbitHole108Ainda não há avaliações
- Antenatal History FormatDocumento9 páginasAntenatal History FormatBincy Jilo90% (20)
- Antenatal Assessment FormatDocumento9 páginasAntenatal Assessment FormatVijith.V.kumar93% (14)
- 의사 발급 건강 진단서(Certificate of HealthDocumento1 página의사 발급 건강 진단서(Certificate of HealthHendra SetiawanAinda não há avaliações
- Evidence Based Oral MedicineDocumento13 páginasEvidence Based Oral MedicineShantanu DixitAinda não há avaliações
- Medical Examination Format-RevisedDocumento2 páginasMedical Examination Format-RevisedAkram KhanAinda não há avaliações
- (Certificate of Health) : (Form 7)Documento2 páginas(Certificate of Health) : (Form 7)Trabajos UniversidadAinda não há avaliações
- DHS CFS 600 Certificate of Child Examination Form IL444-4737Documento2 páginasDHS CFS 600 Certificate of Child Examination Form IL444-4737ArtueroAinda não há avaliações
- HealthapprasalDocumento2 páginasHealthapprasalapi-235111661Ainda não há avaliações
- Prescreen ExamDocumento2 páginasPrescreen Examapi-286308864Ainda não há avaliações
- Nursing Process - VaricocoeleDocumento11 páginasNursing Process - VaricocoeleKayle Irah CaburnayAinda não há avaliações
- Antenatal Assessment ToolDocumento16 páginasAntenatal Assessment Toolpandem soniyaAinda não há avaliações
- Physician'S School Entrance Examination: ImmunizationsDocumento2 páginasPhysician'S School Entrance Examination: ImmunizationsBianca ChanAinda não há avaliações
- Donor Profile: General InformationDocumento25 páginasDonor Profile: General InformationPeon AvanttiAinda não há avaliações
- 의사발급 공식건강검진표 (Official Medical Examination) : 1. Personal InformationDocumento1 página의사발급 공식건강검진표 (Official Medical Examination) : 1. Personal InformationNana AntidzeAinda não há avaliações
- Physical Exam Checklist TemplateDocumento7 páginasPhysical Exam Checklist TemplateDaily ScentAinda não há avaliações
- Buat CaseDocumento13 páginasBuat CaseBima Sena Arya YudhaAinda não há avaliações
- NCSaug 2011Documento24 páginasNCSaug 2011Julius Corpuz BustamanteAinda não há avaliações
- Preventive Care Checklist Male English 2011Documento2 páginasPreventive Care Checklist Male English 2011sjessAinda não há avaliações
- Arvin High School$Physical Examination Form$20191115144801Documento1 páginaArvin High School$Physical Examination Form$20191115144801MGA GamingAinda não há avaliações
- Student Exchange Program Application FormDocumento5 páginasStudent Exchange Program Application FormAqsha ViazeldaAinda não há avaliações
- Mid A AssignmentDocumento24 páginasMid A AssignmentTHE HOWDAY COMPANYAinda não há avaliações
- Pediatric case presentation on morbilliDocumento86 páginasPediatric case presentation on morbilliacildevilAinda não há avaliações
- Complete Medical History FormDocumento1 páginaComplete Medical History FormRichard SazoAinda não há avaliações
- 2020 Korea Application Form7Documento1 página2020 Korea Application Form7jazminAinda não há avaliações
- Case Report on Acute Glomerulonephritis in a 10-Year-Old BoyDocumento67 páginasCase Report on Acute Glomerulonephritis in a 10-Year-Old BoyRuth linayantiAinda não há avaliações
- Health DeclarationDocumento5 páginasHealth Declarationust dol100% (1)
- Health HistoryDocumento1 páginaHealth Historymolly_hayes_24Ainda não há avaliações
- UntitledDocumento59 páginasUntitledRobin KeaneAinda não há avaliações
- Trip Application FormDocumento7 páginasTrip Application Formj_morgan_allen1528Ainda não há avaliações
- Neral Information II. HISTORY OF PRESENT ILLNESS: Patient ExperiencedDocumento10 páginasNeral Information II. HISTORY OF PRESENT ILLNESS: Patient ExperiencedBianca Watanabe - RatillaAinda não há avaliações
- West Visayas State University College of NursingDocumento18 páginasWest Visayas State University College of NursingJohn Xavier S. AbianAinda não há avaliações
- Hpwriteup OutlineDocumento5 páginasHpwriteup OutlinemsmodcAinda não há avaliações
- LIFE INSURANCE JUVENILE MEDICAL FORMDocumento2 páginasLIFE INSURANCE JUVENILE MEDICAL FORMHemant JhaAinda não há avaliações
- History & Physical Examination: Berry Erida HasbiDocumento13 páginasHistory & Physical Examination: Berry Erida HasbiBerdasbi XiphoAinda não há avaliações
- Newborn AssessmentDocumento7 páginasNewborn Assessmentapi-234544335Ainda não há avaliações
- History Taking FormatDocumento10 páginasHistory Taking FormatMuskaan DeepAinda não há avaliações
- Mid A AssignmentDocumento24 páginasMid A AssignmentTHE HOWDAY COMPANYAinda não há avaliações
- Physical Examination FormatDocumento5 páginasPhysical Examination FormatMuhammed sherbinAinda não há avaliações
- Skeleton of History Taking in PaediatricsDocumento37 páginasSkeleton of History Taking in PaediatricsOmar Hassan AgabAinda não há avaliações
- PD 6 To 9Documento103 páginasPD 6 To 9Loai Mohammed IssaAinda não há avaliações
- 5 2 Following A Balanced Food PlanDocumento3 páginas5 2 Following A Balanced Food Planapi-261782961Ainda não há avaliações
- 5 3 Making Healthful Food ChoicesDocumento3 páginas5 3 Making Healthful Food Choicesapi-261782961Ainda não há avaliações
- 5 1 Why Your Body Needs NutrientsDocumento3 páginas5 1 Why Your Body Needs Nutrientsapi-261782961Ainda não há avaliações
- Athlete Code of Conduct Updated 8Documento4 páginasAthlete Code of Conduct Updated 8api-261782961Ainda não há avaliações
- 3 Chapter VocabularyDocumento3 páginas3 Chapter Vocabularyapi-261782961Ainda não há avaliações
- 3 Chapter VocabularyDocumento3 páginas3 Chapter Vocabularyapi-261782961Ainda não há avaliações
- 3 3 CommunicationDocumento3 páginas3 3 Communicationapi-261782961Ainda não há avaliações
- 3 3 CommunicationDocumento3 páginas3 3 Communicationapi-261782961Ainda não há avaliações
- CH 2 Review Game TestDocumento3 páginasCH 2 Review Game Testapi-261782961Ainda não há avaliações
- CH 3 Review Game TestDocumento3 páginasCH 3 Review Game Testapi-261782961Ainda não há avaliações
- 3 1 Your FamilyDocumento3 páginas3 1 Your Familyapi-261782961Ainda não há avaliações
- 3 2 Your Friends and PeersDocumento3 páginas3 2 Your Friends and Peersapi-261782961Ainda não há avaliações
- 2 3 Managing StressDocumento3 páginas2 3 Managing Stressapi-261782961Ainda não há avaliações
- 2 Chapter VocabularyDocumento3 páginas2 Chapter Vocabularyapi-261782961Ainda não há avaliações
- 2 1 Feeling Good About YourselfDocumento4 páginas2 1 Feeling Good About Yourselfapi-261782961Ainda não há avaliações
- CH 1 Review Game TestDocumento3 páginasCH 1 Review Game Testapi-261782961Ainda não há avaliações
- CH 1 Lesson 2 Health SkillsDocumento5 páginasCH 1 Lesson 2 Health Skillsapi-261782961Ainda não há avaliações
- 2 2 Understanding Your EmotionsDocumento4 páginas2 2 Understanding Your Emotionsapi-261782961Ainda não há avaliações
- 1 3 Decisions and Your CharacterDocumento4 páginas1 3 Decisions and Your Characterapi-261782961Ainda não há avaliações
- 1 4 Setting Health GoalsDocumento4 páginas1 4 Setting Health Goalsapi-261782961Ainda não há avaliações
- CH 5 Lesson 3 Healthy Choices & Biggest LoserDocumento29 páginasCH 5 Lesson 3 Healthy Choices & Biggest Loserapi-261782961Ainda não há avaliações
- First Day Procedures Rules Materials Who Am IDocumento19 páginasFirst Day Procedures Rules Materials Who Am Iapi-261782961Ainda não há avaliações
- 1 1 Health and Wellness Lesson PlanDocumento3 páginas1 1 Health and Wellness Lesson Planapi-2617829610% (1)
- 1 Chapter VocabularyDocumento3 páginas1 Chapter Vocabularyapi-261782961Ainda não há avaliações
- Introduction To Health Class Lesson PlanDocumento3 páginasIntroduction To Health Class Lesson Planapi-261782961Ainda não há avaliações
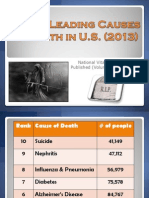
- Leading Cause of Death Lesson PlanDocumento3 páginasLeading Cause of Death Lesson Planapi-261782961Ainda não há avaliações
- Leading Causes of Death 2013Documento14 páginasLeading Causes of Death 2013api-261782961Ainda não há avaliações
- CH 4 Personal HygieneDocumento30 páginasCH 4 Personal Hygieneapi-261782961Ainda não há avaliações
- Ma. Lammatao: Trion AKG Marble LLCDocumento11 páginasMa. Lammatao: Trion AKG Marble LLCNasir AhmedAinda não há avaliações
- Dexamethasone PAR SummaryDocumento17 páginasDexamethasone PAR SummaryJagdish ChanderAinda não há avaliações
- 2020 03 20 - Daily Safety Moment - Coronavirus (COVID-19) Update - No. 719BDocumento2 páginas2020 03 20 - Daily Safety Moment - Coronavirus (COVID-19) Update - No. 719BE. Ricardo Ponce EspejoAinda não há avaliações
- 2016 Issue 1Documento86 páginas2016 Issue 1Fareesha KhanAinda não há avaliações
- Fnsa Final Convention ScheduleDocumento4 páginasFnsa Final Convention ScheduleFNSAAinda não há avaliações
- HSS International PDI Form - February 2023Documento2 páginasHSS International PDI Form - February 2023wyzxy2793Ainda não há avaliações
- Acute Kidney Injury: New Concepts in Definition, Diagnosis, Pathophysiology, and TreatmentDocumento7 páginasAcute Kidney Injury: New Concepts in Definition, Diagnosis, Pathophysiology, and TreatmentMuhamad RizauddinAinda não há avaliações
- Ear - WikipediaDocumento15 páginasEar - WikipediadearbhupiAinda não há avaliações
- Management of Hospital PharmacyDocumento33 páginasManagement of Hospital PharmacyZainab JavaidAinda não há avaliações
- Prescription Template 02Documento2 páginasPrescription Template 024NM19CS099 KUMAR NISHANTAinda não há avaliações
- Director - ProfileDocumento2 páginasDirector - ProfileHimanshu GoyalAinda não há avaliações
- Surgical Versus Medical Treatment of Drug-Resistant Epilepsy: A Systematic Review and Meta-AnalysisDocumento10 páginasSurgical Versus Medical Treatment of Drug-Resistant Epilepsy: A Systematic Review and Meta-AnalysisSebastianAinda não há avaliações
- hw410 Unit 9 AssignmentDocumento12 páginashw410 Unit 9 Assignmentapi-569132011Ainda não há avaliações
- Rabie CateiDocumento3 páginasRabie CateiC LAinda não há avaliações
- Consent Form PDFDocumento2 páginasConsent Form PDFSopheak NGORAinda não há avaliações
- Individual Family Health Insurance ApplicationDocumento7 páginasIndividual Family Health Insurance ApplicationsundarmjkAinda não há avaliações
- 3 - Full Pulpotomy With Biodentine in Symptomatic Young Permanent Teeth With Carious Exposure PDFDocumento6 páginas3 - Full Pulpotomy With Biodentine in Symptomatic Young Permanent Teeth With Carious Exposure PDFAbdul Rahman AlmishhdanyAinda não há avaliações
- Informed Consent - Laser Hair RemovalDocumento4 páginasInformed Consent - Laser Hair RemovalAshraf AboAinda não há avaliações
- Oral Dysfunction in Patients With Head and Neck.10Documento14 páginasOral Dysfunction in Patients With Head and Neck.10Yeni PuspitasariAinda não há avaliações
- NCM 106 BurnsDocumento9 páginasNCM 106 BurnsJudeLaxAinda não há avaliações
- Compensation Fy2018sDocumento218 páginasCompensation Fy2018sJesse YoungbloodAinda não há avaliações
- Managing Pain and Constipation Through Targeted Nursing InterventionsDocumento4 páginasManaging Pain and Constipation Through Targeted Nursing InterventionsCiara ManguiatAinda não há avaliações