("~ DEPARTMENT OF HEALTH & HUMAN SERVICES
J.
Public Health Service
Centers for Disease Control and Prevention
April 9, 2010
Anne Weismann CREW
1400 Eye Street, NW Suite 450
Washington, District of Columbia 20005
Dear Ms. Weismann:
This letter is a third interim response to your Freedom of Information Act (FOIA) request of November 6,2009, pertaining to all records relating to (1) the policy, protocol, and practices of distributing the H1N1 vaccine nationwide including, but not limited to, its distribution state-bystate; and (2) distribution of the H1N1 vaccine to any and all private businesses not engaged directly and primarily in the provision of health care services. FOIA #10-00149.
Enclosed are additional documents which were found in our search (193 pages). Please note:
HHS-generated portions that are redacted were sent to you March 30, 2010, separately in a direct response from Mr. Robert Eckert, Director, HHS FOINPrivacy Acts Division, Office of Public Affairs.
We are withholding certain information where such disclosure would risk circumvention of an agency regulation or statute, impede the effectiveness of an agency's activities, or reveal sensitive information that may put the security and safety of an agency activity or employee at risk. These deletions to two pages of the released documents were made under the provisions of 5 U.S.C. 552(b)(2) of the Act and 45 CFR 5.63 of the Department's implementing regulations (teleconference numbers and passcodes).
You have the right to appeal this decision to deny you full access to agency records. Send your appeal, within 30 days from the date you receive this letter, to the Deputy Assistant Secretary for Public Affairs (Media), U.S. Department of Health and Human Services, Room 17-66,
5600 Fishers Lane, Rockville, Maryland 20857. Please mark both your appeal letter and envelope "FOIA Appeal."
Sincerely yours,
~~~
Katherine Norris
CDC/ATSDR FOIA Officer (Acting) Office of the Chief Information Officer (404) 498-1580
Fax: (404) 498-1575
Enclosures
Norris, Katherine S. (Taffy) (CDC/OCOO/OD)
From:
Sent:
To:
CDC IMS JIC Public Health Workforce (CDC) Friday, July 31, 2009 12:28 PM
'lespino@nphic.org'; Basket, Michelle (CDC/OSELS/NCHM); Harrison, James R. (CDC/CCID/NCIRD); Hill, Antonette Y. (CDC/OID/OD); Janssen, Alan (CDC/OSELS/NCHM); Lennon, Tanya (CDC/OID/NC1RD); McCauley, Mary (CDC(OSELS/NCHM); 'Melissa Talbot'; 'Phyllis Kim'; Smith, Jean Clare (CDC/OID/NCIRD); 'Bob Davis'; Buschick, Jennifer (HHS/OPHS); CDC IMS Chief Of Staff; 'Chad Wood'; Cohen, Mitchell L. (CDC/OID/OD); 'Elizabeth Lautner'; EOC Report (CDC); Fauci, Anthony (NIH/NIAID) [E]; Gomez, Thomas M. (CDC/OID/NCZVED); Hall, Bill (HHS/ASPA); Helfand, Rita (CDC/OID/NCPDCID); 'John Korslund'; Kane, Eileen (HH$/ASPR/OPSP); Krull, Andrea (HHS/OPHS); 'Lyndsay Griffin'; Marshall, Stephanie (HHS); Mayfield, Evan D. (CDC/OCOO/OD); Michael, Gretchen (HHS/ASPR/OPSP); Migliaccio, Kate (HHS/OPHS); Moreno, Julie (HHS/OS); 'National JIC'; Pickering, Larry (CDC/OID/NCIRD); Smith, Amanda (HHS/ASPR/OPSP); Sosin, Dan (CDC/OPHPR/OD); 'Stan Health'; Zaza, Stephanie (COC/OPHPR/OD); 'Anna Buchanan'; 'ASTHO info center'; Bhatt, Achal (CDC/OID/NCIRD); Burns, Erin (CDC/OID/NCIRD); CDC IMS State Health Department Branch Oirector(CDC); Evans, Victoria (CDC/OID/NCIRD); Lemmings, Jennifer (CDC cste.org); PSC Jennifer Joseph; Kilgus, Duane (CDC/OID/NCIRD); Robinson, LaKesha (CDC cste.org); Kan, Lilly (CDCnaccho.org); McConnon, Patrick (CDC cste.orq): 'Paul Etkind'; 'Richard Hughes'; Fasano, Nancy (CDC/OID/NCIRD); Harton, Elizabeth (CDC/OIO/NCPDCID); NCIRD Immunization Grantee Mailbox (CDC); Pope, Kristin (CDC/OID/NCIRO); Rodewald, Lance (CDC/OID/NCIRD); Whitehead, Cynthia (CDC/OID/NCIRD)
Updated Novel H1 N1 Flu CDC key points for July 31,2009
Subject:
Hello, CDC Partners:
Here are today's novel Hi N 1 key points, Feel free to use them to answer public and media questions and to disseminate to your partners.
Best,
Nadya Belins
lead Public Health Workforce Team Lead 404.838.7179
What's New and Updated Today
• Activity Update
• International Update
• Pregnancy and Novel H iN 1 Flu Infection
• Rapid Influenza Diagnostic Tests and Novel H1Nl Flu
• Novel H1Nl Influenza Vaccine
• Novel H lNl Influenza Vaccine Safety
• Seasonal Influenza Vaccine
Activity Update
• Influenza illness, including illness associated with the novel influenza A CH1Nl) virus, is ongoing in the United States.
• Beginning this week, CDC is reporting total hospitalizations and deaths nationally (not by state).
• As of July 31, 2009, 5,514 total novel influenza A CH1Nl) hospitalizations, and 353 total deaths have been reported to CDC by state and local public health departments.
1
• CDC estimates that there have been more than 1 million cases of novel H1Nl flu in the United States.
• The July 31 FfuView Report shows that influenza activity decreased in the United States during July 19-25, 2009; however, there are still higher levels of influenza-like illness than is normal for this time of year. Novel H1Ni flu outbreaks are ongoing in parts of the United States, in some cases with intense activity.
• Twelve (12) states and Puerto Rico are reporting widespread or regional influenza activity:
• This includes four (4) states in the United States that are reporting widespread influenza activity (California, Hawall, Maine, and New Jersey);
• 8 states that are reporting regional influenza activity;
• 19 states and the District of Columbia that are reporting local influenza activity; and
• 19 states that are reporting sporadic activity.
II It is very unusual for this time of year to still be having so many states reporting regional and widespread activity.
• Novel HiNl viruses now make up more than 98% of all sub-typed influenza A viruses analyzed by the U.S. WHO/NREVSS collaborating laboratories.
• The proportion of deaths attributed to pneumonia and influenza (P&I) was below the epidemic threshold.
• Two (2) influenza-associated pediatric deaths were reported to CDC.
• These deaths occurred in Florida and Utah.
• Both of these deaths were associated with novel H1N1 flu.
• The deaths reported this week occurred during weeks 23 and 26 (the weeks ending June 13, 2009 and July 4, 2009).
• Since September 28, 2008, CDC has received 97 reports of laboratory confirmed influenza-associated pediatric deaths that occurred during the 2008-09 influenza season, 28 of which were due to novel influenza A (HiNl) virus infections.
• It's uncertain at this time how severe this pandemic will be in terms of how many people infected will have severe complications or death from novel H1Nl flu-related illness.
• It is likely that localized outbreaks will continue to occur over the summer and that we will see novel H1Nl virus, illness and death during the upcoming U.s. flu season in the fall and winter.
• CDC anticipates that novel H1Nl viruses will co-circulate with regular seasonal influenza viruses over our influenza season.
• The tlmlnq, spread and severity of novel H1Nl virus - in addition to our regular seasonal influenza viruses - are uncertain.
2
International Situation Update
• Novel influenza A (Hf.Nt ) continues to circulate widely.
• Descriptive epidemiology of cases remains similar across countries.
• Isolates sequenced at WHO and CDC suggest that circulating novel influenza A (H1Ni) viruses look similar to A/California/07/2009, which is the reference virus selected by WHO as a potential candidate for novel influenza A (H1Nl) vaccine.
• As of July 27, World Health Organization (WHO) regions have reported 134,503 laboratory-confirmed cases of novel influenza A CHiN 1) and 816 deaths worldwide. The lab-confirmed cases represent an underestimation of total cases in the world as many countries have shifted to strategies of clinical confirmation and prioritization of laboratory testing for only persons with severe illness and/or high risk conditions.
• Currently, the novel influenza A (HiNl) virus is the dominant influenza virus in circulation in New Zealand, Australia, Chile, Argentina and Brazil. .
• Influenza viruses currently being detected in England and Canada are almost exclusively novel Influenza A (H1Nl).
! _ _£Qllowing a seasonal influenza season that was dominated by influenza A (H3N2) virus circulation, South Africa is now detecting novel influenza A (Hf.Nt ) through its routine surveillance system. Currently, however, influenza A (H3N2) remains the dominant virus in circulation in South Africa.
• Many seasonal influenza viruses from these countries have not been subtyped. Of those that have been subtyped in Australia, South Africa, and Argentina, the majority are influenza A (H3N2) viruses.
Pregnancy and Novel HiNi Flu Infection
• An article entitled "Ht.Nt 2009 Influenza Virus Infection During Pregnancy in the USA" has been published in the online edition of The Lancet on July 29, 2009 at http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(09)6i304-0/fulltext.
• CDC has a number of guidance documents on its website related to pregnancy. These are available at www.cdc.govlhlnlflu.
• Pregnant women with suspected or confirmed influenza infection need prompt treatment with antiviral medication.
• Pregnant women are at an increased risk for pregnancy complications if infected with an influenza virus.
• Pregnant women who are otherwise healthy have been severely impacted by the nove!
HiNl influenza virus.
• Pregnant women who have been infected with novel HiNl influenza virus have had a higher rate of hospitalization than the general population.
3
• Of 45 deaths reported to CDC during the first two months of the outbreak, 6 (13%) were in pregnant women.
• Treatment of fever in pregnant women is also important as high fevers may cause problems in a developing fetus, including neural tube defects-.
• CDC has posted clinical guidance for treatment and prophylaxis of pregnant women with suspected or confirmed novel H1Nl influenza at the following link: http://www.cdc.gov/hlnlflu/clinicianpregnant.htm
Rapid Influenza Diagnostic Tests and Novel H1Nl Flu
• On Wednesday, July 29th, CDC issued "Interim Guidance for the Detection of Novel Influenza A Virus Using Rapid Influenza Diagnostic Tests," This guidance updates previous
guidance on this topic and is available at '
http://www.cdc.gov/h1nlflu!guidance!rapidtesting.htm.
• This interim guidance provides an overview of the sensitivities of rapid influenza diagnostic tests (RIDT) in detecting novel influenza A (HiNl) virus in order to help guide the reporting and interpretation of test results.
• This document does not discuss either direct (DFA) or indirect immunofluorescence assays (IF A).
• This guidance is primarily intended for clinical laboratories and clinical practices conducting influenza testing on respiratory specimens from patients with suspected novel influenza A(H1Nl) virus infection.
• Information on laboratory biosafety is available at: http://www.cdc.gov/hlnlflu/guidelineslabworkers.htm
• Interim guidance on clinical testing recommendations is available at: http: !(www.cdc.gov/hlnlflu/specimencollection.htm .
Novel H1Nl Influenza Vaccine:
• CDC's Advisory Committee on Immunization Practices (ACIP), a panel made up of medical and public health experts, met July 29, 2009, to make recommendations on who should receive the new H1Nl vaccine when it becomes available, and to determine which groups of the population should be prioritized if the vaccine is initially available in limited quantities.
• The Committee recommended that initial vaccination efforts focus on five key populations:
• all people 6 months through 24 years of age
• people who live with or care for children younger than 6 months of age
• all pregnant women
• healthcare and emergency services personnel, and
• people aged 25 through 64 years who have health conditions associated with higher risk of medical complications from influenza.
• Together, these key populations equal 159 million.
4
• By vaccinating these priority groups we hope to reduce the impact of H1N1. People in these groups are at higher risk of disease or serious complications, likely to come in contact with novel H1Nl, or who could infect young infants.
• Vaccinating persons who live with or care for children <6 months is the best way to help protect these children since those there is no influenza vaccine for children <6 months.
• Once the demand for vaccine for these prioritized groups has been met at the local level, programs and providers should begih vaccinating everyone from the ages of 25 through 64 years.
• Current studies indicate that the risk for infection among persons age 65 or older is less than the risk for younger age groups. Many older adults seem to already have some existing immunity to the novel H1Nl virus. However, as vaccine supply and demand for vaccine among younger age groups is being met, programs and. providers should also offer vaccination to people 65 years and older.
• Availability and demand for vaccine can be unpredictable. It is possible that initial amounts of vaccine will not be enough to meet demands.
• If vaccine is available in insufficient amounts for the initial priority groups, the following groups would be prioritized:
• pregnant women,
• people who live with or care for children younger than 6 months of age,
• healthcare and emergency services personnel with direct patient contact,
• children 6 months through 4 years of age, and
• children 5 through 18 years of age who have chronic medical conditions.
• Novel H1Nl vaccine supply and availability is projected to increase quickly over time, and vaccine should not be kept in reserve for later administration of the second dose.
• The novel H1Nl vaccine is not intended to replace the seasonal flu vaccine - it is intended to be use along-side seasonal flu vaccine to protect people.
• It is anticipated that seasonal flu and novel H lNl vaccines may be administered on the same day.
• The ACIP recommendations are one important step in a broader plan related to novel H1Nl vaccine production and implementation of a national voluntary vaccination program.
• We are aggressively taking early steps in the vaccine manufacturing process, working closely with manufacturing and the rest of the government.
• CDC isolated the novel H1Nl virus, made candidate vaccine virus strains that can be used to create vaccine, and has provided this virus to industry so they can begin scaling up for production of a Vaccine.
• SCientists in a network of medical research institutions across the United States will soon begin an initial set of five clinical trials of candidate novel H1Nl influenza vaccines. The
5
research will be under the direction of the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health, More information about these clinical trials can be found at http://www3.niaid.nih.gov/news/QAJvteuHiNiqa.htm
• The five manufacturers who already produce U.S.-licensed seasonal vaccine are also conducting their own novel H1Ni influenza vaccine trials under contract with HHs.
• There are many steps involved with producing a vaccine and we are committed to going forward with the NIH, FDA, BARDA, and the manufacturers of influenza vaccines, to see about developing full scale vaccine production.
• If things progress to full scale production, Vaccine may be available as early as midOctober.
• The novel HiNi influenza vaccine will be made using the same processes and facilities that are used to make the currently licensed seasonal influenza vaccines.
• We will provide the public with transparent information about what we know and do not know about the safety and efficacy of novel H1Nl vaccines to help them make informed decisions.
• A mass vaccination program of even a modest scale will involve extraordinary efforts at the federal, state and local levels.
Novel H1Nl Influenza Vaccine Safety
• As medical and public health professionals, parents, and grandparents, ensuring the health and safety of our children is a top priority.
• We are concerned with protecting our nation's children from vaccine-preventable diseases like influenza and preventing any possible adverse events from vaccines.
• The potential for more severe illness and many more deaths or disability caused by this new strain of influenza weighs heavily on our minds - as does the unfortunate outcome of the 1976 swine flu vaccination program.
• The novel H1Nl flu vaccines will be very much like seasonal flu vaccines, which have a very good safety profile. However, no vaccine is 100% safe. This vaccine will be no exception.
• Those who choose vaccinatlon for themselves or their children will be screened for contraindications (such as egg allergy) and will receive information sheets describing the vaccine's risks and benefits, signs and symptoms of adverse events to look for following vaccmatlon, and how to report adverse events.
• We expect that H iNl vaccines will be available in multiple formulations, including a formulation that does not contain the preservative thimerosal.
• CDC is working to enhance our safety monitoring systems and will actively encourage providers and vaccine recipients to report to us adverse events following vaccination (whether or not they believe the vaccine caused the event). We will be monitoring very closely for any signs that the vaccine is causing unexpected adverse events and we will work with state and local health officials to investigate any unusual events rapidly.
6
Seasonal Influenza Vaccine
• The new HiNi influenza virus is a reminder of the unpredictable nature of influenza, and the importance of prevention.
• While the novel Ht Nt influenza virus has been the focus of attention since the spring, it is important that we do not forget the risks posed by seasonal influenza viruses.
• Every year in the United States, on average 5% to 20% of the population gets the flu; more than 200,000 people are hospitalized from flu complications, and; about 36,000 people die from flu-related causes. Some people, such as older people, young children, and people with certain health conditions, are at high risk for serious complications from seasonal influenza.
• The single best way to protect yourself and your loved ones against the flu is to get vaccinated each year.
• We hope that people, especially those at high risk for serious complications and their close contacts, will start to go out and get vaccinated in September or as soon as vaccine is available at their doctors' offices or in their communities.
• It is not too early to get a flu vaccine as soon as it is available in August or September.
The protection you get from the vaccine will not wear off before the flu season is over.
• While we hope that people who want to avoid getting seasonal influenza will not delay getting vaccinated, we know that some will. We will be encouraging them to get vaccinated throughout the influenza season, into December, January, and beyond.
• Annual flu vaccines contain three viruses: one A (HiNi) virus, one A (H3N2) virus and //one B virus. The viruses in the vaccine change each year based on international surveillance and scientists' estimations about which types and strains of viruses will circulate in a given year.
• We recognize the fact that annual flu vaccines contain an A (HiNi) virus may cause some confusion. The novel HiNi influenza virus that has caused the current pandemic is not the same as the HiNi virus in the seasonal flu vaccine.
• We want to make sure that we communicate clearly to the public that the seasonal flu vaccine is not expected to protect against the novel HiNi influenza virus. There are efforts underway to develop a safe and effective novel HtNt vaccine.
• As always, it's not possible for us to predict at this time of year whether this year's seasonal vaccine will be a good match with Circulating viruses.
• Influenza viruses are constantly changing - they can change from one season to the next or they can even change within the course of the same season.
• Experts must pick which viruses to include in the vaccine many months in advance in order for vaccine to be produced and delivered on time.
• Because of these factors, there is always the possibility of a sub-optimal match between Circulating viruses and the viruses in the vaccine.
7
• While a less than ideal virus match can reduce the vaccine's effectiveness against the variant virus, the vaccine can still offer cross-protection against related influenza viruses and prevent many illnesses and flu-related complications.
Updated Key Points July 31 200 ...
s
Norris, Katherine S. (IaffX} (CDC/OCOO/OD)
From:
Sent:
To:
Subject:
CDC IMS JIC Public Health Workforce Thursday, December 10, 2009 2:58 PM CDC IMS JIC Public Health Workforce
CDC Current and Recent Key Messages, December 10, 2009
12-10-2009 Daily Key Messages ....
CDC Current and Recent Key Messages, December 10, 2009 2009 H1N1 Influenza Vaccine Supply
• 2009 Hl Nl Vaccine Allocation. Total available as of Dec. 10 is 85.2mmion doses, 12.6 more available doses than last Friday (~23% of doses are nasal sprayer).
2009 HINl Severity - Updated Cases Estimates of 2009 HiNi
• (See hUp:!lwww.cdc.gov/h1n1flu!estimates=2009. H1N1.htm for details.)
• CDC developed a method to provide an estimated range of the total number of 2009 H1Nl cases, hospitalizations and deaths in the United States as well as a breakdown of these estimates by age groups during the pandemic.
• CDC provided its first set of estimates on these figures on November 12, 2009 for period from April through October 17, 2009. On December 10, 2009, CDC updated these estimates for April through November 14, 2009.
• CDC estimates that approximately 47 million cases of 2009 HIN1 occurred between April and November 14, 2009. (An increase in 25 million from the estimate reported on November 12.)
• CDC estimates that approximately 213,000 2009 H1N1-related hospitalizations occurred between April and Nov. 14,2009. (An increase in 115,000 from the estimate reported on November 12.)
• CDC estimates that approximately 9,820 2009 HtNl-related deaths occurred between April and November 14, 2009. For children 0-17 years old, CDC estimates approximately 1,090 deaths; ages 18-64 approximately 7,450 deaths; and ages 65 years and older approximately 1,280 deaths. (An total increase in 5,920 from the estimate reported on November 12.)
• With seasonal influenza, about 60 percent of seasonal flu-related hospitalizations and 90 percent of flu-related deaths occur in people 65 years and older. In comparison, CDC estimates of death by age group associated with 2009 H1N1 through November 14 are that about 87% of deaths have occurred in people younger than 65 years.
• Approximately 15% of the U.S. population has been infected by the 2009 H1N1 virus. 2009 HlNl-related Deaths Rates in American Indians and Alaskan Natives
• American Indians and Alaska Natives (AI/AN) were 4 times more likely to die from 2009 H1Nl than the general population, according to a recent investigation of influenza-related deaths occurring in 12 states between April 15 and November 13, 2009.
• About 10% of deaths occurred among American Indians and Alaska Natives, although they make up only about 3% of the population in these 12 states. After adjusting for differences in the ages of these groups, this means American Indians and Alaska Natives are 4 times more likely to die from 2009 H1N1 than the general population.
• Because of these findings, CDC is increasing awareness among American Indians and Alaska Natives and their health-care providers about H1Nl influenza. Health professionals and agencies, especially those serving American Indians and Alaska Natives, should expand community education regarding the risk for influenza
1
complications and mortality, use influenza antiviral medication early for those at increased risk for HINI influenza complications, and promote vaccination against 2009 HINI and seasonal influenza.
• The factors that place American Indians and Alaska Natives populations at higher risk for influenza-related deaths are unknown, but may include higher rates of underlying chronic illness such as diabetes. The age-specific prevalence of diabetes in American Indians and Alaska Natives adults is two to three times higher than for U.S. adults in general. Poverty and other social determinants of health may create barriers to medical care. The American Indians and Alaska Natives poverty rate for households with children under 18 years of age is 30% -a rate that is twice the national rate and three times the rate for non-Hispanic whites.
2009 H1Nl Vaccine
• Among the five initial target groups for the 2009 HINI vaccine identified by the Advisory Committee on Immunization Practices are health care and emergency medical services personnel. Healthcare and emergency medical personnel are encouraged to get the 2009 HINl vaccine because infections among healthcare workers have been reported and an infected healthcare worker can be a potential source of infection for vulnerable patients. Additionally, increased absenteeism in this population could reduce our healthcare system capacity.
• Vaccination is the best way to prevent the flu and its complications. This is the reason that CDC, national health organizations, and healthcare providers are encouraging persons at high risk for influenza complications and death to get vaccinated against the 2009 HlNI influenza as well as the 2009-2010 seasonal influenza.
2
Norris, Katherine S. (Taffy> (CDC/OCOO/OD)
From:
Sent:
To:
Subject:
CDC IMS JIC Public Health Workforce Friday, November 06, 2009 3:01 PM CDC IMS JIC Public Health Workforce
CDC Updated Key Points: November 6,2009
Importance:
High
Updated 2009 F0943 CDC FluView -ilNi Key POints N.. Oct 31 2009 ....
Good afternoon Partners,
Enclosed are the updated CDC key points for seasonal and 2009 Hi N1 flu as of November 6,2009. Also enclosed is the updated FluView U.S. Weekly Influenza Surveillance Report for MMWR Week 43 (October 25- 31, 2009).
Have a great weekend.
1
2009 H1Nl Influenza Updated Key Points November 6, 2009
What's New and Updated
o Activity Update
o International Situation Update
o 2009 HiNi Influenza Vaccine
o 2009 H iN 1 Influenza Vaccine Safety
o Seasonal Influenza Vaccine
A Summary of CDC Key Public Health Messages this Season
• Flu activity remains high in the United States. Forty-eight states are reporting widespread flu activity. Nationally, visits to doctors for influenza-like-illness declined slightly from last week, but are still very high. Flu-related hospitalizations and deaths continue to increase and are very high nation-wide compared to what is expected for this time of year
• While influenza is unpredictable, high levels of influenza activity may continue for several weeks, and even after flu activity peaks, it's possible that other waves of influenza activity may occur - caused by either 2009 H1Nl viruses or regular seasonal flu viruses.
• CDC recommends a three-step approach to fighting the flu:
o vaccination;
o everyday preventive actions, including covering coughs and sneezes, frequent hand washing, and staying home when sick;
o and the correct use of antiviral drugs if your doctor recommends them.
• 2009 H1Nl vaccination has begun. Supplies are increasing daily, but remain limited. We ask members of the public who want to receive this vaccine to be patient as this program expands and more vaccine becomes available. There will be enough vaccine available for anyone who wishes to receive it.
Activity Update
• It's very important that antiviral drugs be used early to treat flu in people who are very sick (for example people who are in the hospital) and people who are sick with flu and have a greater chance of getting serious flu complications, like people with asthma, diabetes or people who are pregnant.
• Each week CDC analyzes information about influenza disease activity in the United States and publishes findings of key flu indicators in a report called FluView.
Page of 1 of 12
2009 HlN1 Influenza Updated Key Poi nts November 6, 2009
• Information collected during the week of October 25-31, 2009 is reported in FluView on November 6, 2009.
• Be!ow is a summary of the most recent key indicators:
• Visits to doctors for influenza-like illness (IU) nationally decreased very slightly this week over last week after four consecutive weeks of sharp increases.
• While III declined slightly, visits to doctors for influenza-like illness remain at much higher levels than what is expected for this time of the year and parts of the country continue to see sharp increases in activity.
• It's possible that nationwide III could rise again. III continues to be higher than what is seen during the peak of most regular flu seasons.
• Total influenza hospitalization rates for laboratory-confirmed flu continue to climb and are higher than expected for this time of year.
• Hospitalization rates continue to be highest is younger populations with the highest hospitalization rate reported in children 0-4 years old.
• The proportion of deaths attributed to pneumonia and influenza (P&I) based on the 122 Cities Report continues to increase and has been higher for five week now than what is expected at this time of year.
• In addition, 18 flu-related pediatric deaths were reported this week; 15 of these deaths were confirmed 2009 HiNi, and three were influenza A viruses, but were not subtyped.
• Since April 2009, CDC has received reports of 129 laboratory-confirmed pediatric 2009 H1Nl deaths and another 15 pediatric deaths that were laboratory confirmed as influenza, but where the flu virus subtype was not determined. (More information on these pediatric deaths is available below.)
• Forty-eight states are reporting widespread influenza activity at this time; a decline of one state over last week. They are: Alabama, Alaska, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, Florida, Georgia, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, South Carolina! South Dakota, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
• This many reports of widespread activity at this time of year are unprecedented during seasonal flu.
Page of 2 of 12
2009 H1Nl Influenza Updated Key Points November 6,2009
• Almost all of the influenza viruses identified so far continue to be 2009 H1Nl influenza A viruses.
• These viruses remain similar to the virus chosen for the 2009 H1Nl vaccine, and remain susceptible to.the antiviral drugs oseltamivir and zanamivir with rare exception
Pediatric Deaths
• During Week 43 (the week ending October 31, 2009), 18 influenzaassociated pediatric deaths were reported to CDC.
o These deaths occurred in California [8], Indiana, Louisiana [2], Mississippi, NeW York, Oklahoma, Texas [2J, Virginia, and West Virginia.
o Fifteen of these deaths were confirmed 2009 HiNi, and three were influenza A viruses, but unsubtyped.
o These deaths occurred between July 12 and October 31, 2009.
o Seven deaths reported this week, occurred during the 2008-09 flu season, bringing the total number of reported pediatric deaths that occurred during that season to 124.
• The cumulative total number of laboratory-confirmed pediatric deaths related to 2009 H1Nl since April 2009 is 129. (Since August 30, 2009 when the flu season "re-set", CDC has received reports of 85 fluassociated pediatric deaths; 73 of these were due to 2009 H1Nl, and the remaining 12 were influenza A viruses that were not subtyped.)
• A table showing reports of flu-related pediatric deaths (including a cumulative total of 2009 H1Nl pediatric deaths since April, 2009) is available on the CDC website at http://www.cdc.gov/hlnlflu/updates/us/#pedhlnlcases .
• Since CDC began tracking pediatric flu-related deaths in 2003-2004, the number of pediatric deaths reported to CDC has ranged from 46 during the 2005-2006 season to 153 during the 2003-2004 season.
• Information on how hospitalizations and deaths are being reported this season is available at http://www.cdc.gov/hlnlflu/reportingga.htm
International Situation Update
• The 2009 H1Nl influenza virus is the predominant influenza virus in circulation in most countries worldwide.
• In temperate regions of the Southern Hemisphere, little disease due to 2009 HiN1 has been reported.
Page of 3 of 12
2009 H1Nl Influenza Updated Key Points November 6, 2009
o The epidemiology of disease caused by 2009 H1N1 influenza in the Southern Hemisphere has been very similar to what was described in the United States in the spring of 2009.
o There have been no significant changes detected in the 2009 H1N1 influenza viruses isolated from persons in the Southern Hemisphere as compared to viruses isolated from persons in the Northern Hemisphere.
• In tropical regions of the Americas and Asia, influenza activity due to 2009 H1Nl remains variable.
• In temperate regions of the Northern Hemisphere, high rates of influenzalike illness (IU) activity due to 2009 H1Nl continues to increase across many countries in Europe and Asia, as well as parts of the United States, Mexico and Canada.
• According to the World Health Organization (WHO), the majority of 2009 H1Nl influenza isolates tested worldwide remain sensitive to oseltamivir, an antiviral medicine used to treat influenza. Worldwide, only 42 2009 H1Nl isolates tested have been found to be resistant to oseltamivir - 14 of these isolates were detected in the United States.
• The World Health Organization (WHO) continues to report updated 2009 H1N1 flu-associated laboratory-confirmed cases and deaths on its Web page (http://www.who.int/csr/disease/swineflu/updates/en/). These laboratory-confirmed cases represent a substantial underestimation of total cases in the world, as many countries focus surveillance and laboratory testing only on people with severe illness.
• Since April 19, 2009, more than 60 percent of all influenza specimens reported to WHO have been 2009 H1Nl.
• On September 17, 2009, several countries including the United States announced plans to donate 2009 H1Nl vaccine or funds to support vaccination campaigns in less developed countries.
2009 H1Nl Influenza Vaccine
In this Section:
o Supply
o Recommendations
o Research
Supply
Page of 4 of 12
2009 H1Nl Influenza Updated Key Points November 6,2009
• The aggregate number of 2009 HiNi flu vaccine doses allocated are now being posted daily by 12:00 PM ET and are available at http://www.cdc.gov/hlnlflu/vaccination/vaccinesupply.htm.
• (Updated) As of Wednesday, November 4, 2009, there were a total of 28,036,300 doses ordered and a total of 26,248r100 shipped.
• (Updated) As of Friday, November 6, 2009, a total of 38,038,100 doses were available for ordering. Of those available doses, 27,480,000 doses were injectable (flu shots) and 10,558,100 were LAIV (nasal spray vaccine).
• The vaccine situation changes rapidly - throughout each day, vaccine is being shipped from the vaccine manufacturers to McKesson distribution centers; orders are coming into McKesson; orders are being processed and shipped; and vaccine is arriving in thousands of places across the country.
• 2009 H1Nl vaccination has begun but initial supplies are small. More doses are expected for shipment each week. We ask members of the public who want to receive this vaccine to be patient as this program expands and more vaccine becomes available. There will be enough vaccine available for anyone who wishes to receive it.
• First doses of 2009 H1N1 vaccine were administered outside of the clinical trials on Monday, October 5, 2009.
• Initial doses of 2009 H iN 1 "flu shot" were shipped the week of October 12, with additional doses scheduled for shipment each week.
• The challenges associated with the U.S. influenza vaccine supply are multi-faceted. Influenza viruses change from year to year, so influenza vaccines must be updated annually to include the viruses that research indicates are most likely to circulate in the upcoming season. Once the viruses are selected for the new formulation, manufacturers operate under a very tight timeline for producing, testing, releasing and distributing the vaccine. Due to these time constraints, any problems encountered during production may cause shortages or delays, and in fact, such problems have impacted the seasonal supply during some recent influenza seasons, and can occur with any type of influenza vaccine, including the 2009 H1Nl vaccine.
• The vaccine development process is complex and forecasting how much vaccine will be available at a certain time is challenging and amounts will vary from week to week. Millions of doses of vaccine are in the pipeline and federal, state and local public health authorities are working hard to get vaccine out to the public as soon as it is received.
Page of 5 of 12
2009 H1Nl Influenza Updated Key Points November 6, 2009
• A decision had to be made between waiting to distribute vaccine until large quantities were ready to be shipped versus distributing limited quantities of the vaccine sooner. The latter was chosen knowing that it would create some challenges and frustrations (for our public health partners in the states/ providers, and the public), but also knowing that it would allow for people to start being protected against this disease sooner.
• It also is important to keep in mind that there will be lag times between states placing orders and vaccine actually being distributed (we are not cutting corners in terms of steps like quality control checks) - and any number of things can create lag times between time of distribution to states and when vaccine actually arrives in provider offices or clinics.
• This vaccine program is a massive and challenging undertaking and is being carried out at a time when state and local health departments have experienced severe budget cuts.
• (New) A new video podcast is now available on the CDC website; "H1N 1 Flu Vaccine- Why the Delay?" explains how flu vaccines are made, manufactured, shipped and how people can find vaccine in their area. To watch the podcast, visit
httg: I/www2c.cdc.gov/godcastslplayer.asp?f=262894# or http://www.cdc.gov/Features/H1N1VaccineDelayf on YouTube.
• (New) The federal government allocates vaccine on a pro rata basis to state health departments and some big city health departments who then make decisions about how to distribute vaccine equitably and efficiently within their jurisdictions.
• (New) Employee or workplace health clinics (among other locations) are a legitimate-and very effective-place to administer vaccine during a time of shortage. These clinics can and do reach and target people in priority vacclnatlon groups, including pregnant women and 18 to 64 year workers with medical conditions that put them at higher risk for influenza complications.
Recommendations
• A report in the August 21, 2009, Morbidity and Mortality Weekly Report (MMWR) provides official recommendations by CDC's Advisory Committee on Immunization Practices (ACIP) regarding the use of vaccine against 2009 H1Nl influenza. This report is available at http://www.cdc.gov/mmwripreview/mmwrhtml/rr58e0821al.htm
Page of 6 of 12
2009 H1Nl Influenza Updated Key Points November 6, 2009
• The guiding principle of these recommendations is to vaccinate as many persons as possible as quickly as possible with an emphasis on vaccinating certain target groups with initial doses of vaccine.
• These recommendations:
1) Identify five initial target groups for vaccination efforts comprising an estimated 159 million persons (pregnant women, persons who live with or provide care for infants younger than 6 months, health care and emergency medical services personnel, children and young adults aged 6 months through 24 years, and persons aged 25 through 64 years who have medical conditions that put them at higher risk for influenza-related complications),
2) Establish a priority subset of persons within the initial target groups in the event that initial vaccine availability is unable to meet demand, and
3) Provide guidance on use of 2009 H1Nl vaccine in other adult population groups as vaccine availability increases.
• The recommendations are broad and allow for flexibility to accommodate local variability in vaccine needs and demands. Providers should be aware of and follow any additional guidance provided by their state or local health departments. If no additional guidance is provided at the state or local level, providers should vaccinate among the initial target group populations on a first come, first serve basis.
• Simultaneous administration of inactivated vaccines (shots) against seasonal and the 2009 H1N1 influenza viruses is permissible if different anatomic sites are used (for example, one vaccine in each arm).
• (New) CDC has no recommendation regarding the administration of acetaminophen or other antipyretic drugs following influenza vaccination. You should follow the guidance of your physician or other health care provider.
Research on Public Knowledge, Attitudes and Beliefs
• (New) A national poll with a representative sample of 1,073 adults aged 18 and over was conducted by the Harvard School of Public Health (HSPH) on October 30 through November 1, 2009. The poll asked about people's perceptions and experiences of trying to get the Ht Nt vaccine for themselves or their children.
• (New) 91% of the polling sample who were unable to get the 2009 HiN1 flu vaccine said that they will try again this year to get the vaccine for themselves, their children or both.
o Even though there was only a limited amount of 2009 HiNl vaccine available in early October, more vaccine wil! continue to become
Page of 7 of 12
2009 HiNi Influenza Updated Key Points November 6, 2009
available over the upcoming weeks and months. Therefore, individuals who were unable to initially get the vaccine and plan to try again once more vaccine is available should contact various settings such as local health departments, healthcare provider websites and hotllnes, schools, and other private settings, such as pharmacies and workplaces to see if the vaccine is available.
• (New) To view a full report of the Harvard Poll press release, visit http://www . hsph. ha rva rd .edu/news/press-releases/
2009 HiNi Influenza Vaccine Safety
In this section:
o General H'l Nl, Vaccine Safety
o Vaccine Safety Monitoring
o Background Rates of Medical Events General HiNi Vaccine Safety
• CDC expects that the 2009 HtNt influenza vaccines will have similar safety profiles as seasonal influenza vaccines, which have very good safety track records.
• The types and frequencies of side effects from the 2009 H1N1 influenza vaccine will likely be similar to those experienced following seasonal influenza vaccines which are mild, localized reactions.
• The most common side effects of the vaccines are pain, redness, or swelling where the shot was given in the arm or a runny nose and headache after the nasal spray.
Vaccine Safety Monitoring
• HHS released a report on the Federal Plans to Monitor Immunization Safety for the Pandemic 2009 Ht.Nt Influenza Vaccination Program: http://flu.gov/professionallfederal/monitorimmunizationsafety.html
• CDC and its partners are using several systems to monitor the safety of 2009 H'l N'L influenza vaccine. Two primary systems that are in use are the Vaccine Adverse Event Reporting System (VAERS), which is jointly operated with FDA, and the Vaccine Safety Datalink (VSD) Project.
• CDC has enhanced vaccine safety monitoring efforts in several ways:
o The Vaccine Adverse Event Reporting System (VAERS) is a voluntary reporting system that identifies potential vaccine safety signals: healthcare providers are actively reminded to report suspected issues,
Page of 8 of 12
2009 H1Nl Influenza Updated Key Points November 6, 2009
and medical personnel are conducting daily reviews and follow-up [http://vaers.hhs.gov].
o Second, a new Web-based active surveillance system is being implemented to prospectively follow tens of thousands of vaccinated people [www.myflushot.org],
o Third, large population-based systems that link computerized vaccination data with healthcare codes will be used to conduct rapid and ongoing analyses. This approach includes data from large managed care plans, other health plans, Department of Defense, Medicare and the Veterans/ Administration.
o Fourth, active case finding for GBS is being conducted in 10 areas of the United States (a combined population of about 50 million people).
o Findings from all sources are cross-referenced and reviewed by government and outside scientists to be sure any concerns are rapidly addressed.
• Vaccine safety monitoring includes reviewing adverse events reported by providers, manufacturers, people who were vaccinated or their caregivers.
o An adverse event following immunization is a medical incident that occurs after someone receives an immunization.
o Adverse events maybe coincidental (meaning occurring around the same time but not related to vaccination) or caused by vaccination.
o Adverse events can be reported by providers, manufacturers, people who were vaccinated or their caregivers,
• The purpose of vaccine safety monitoring is timely identification of any clinically significant adverse events following immunization, as well as to provide timely information to the public, vaccine providers, public health officials, and policy makers.
Background Rates of Medical Events
• Adverse events-such as sudden deaths, spontaneous abortions, and Guillaln-Barre syndrome-will occur in the population. These will occur whether or not people have been vaccinated. In the context of vaccine safety monitoring, we call these naturally occurring events "background rates."
• Awareness of the background rates of several adverse events is critical to assessing the safety of the vaccine. This information allows public health and medical experts to identify when adverse events are occurring more frequently than would be expected in the absence of vaccination and need
Page of 9 of 12
2009 H1Nl Influenza Updated Key Points November 6, 2009
more detailed investigation to determine if the vaccine is causing the adverse events.
• Background rates are helpful as a too! to assess vaccine safety by comparing the expected rate of adverse events to the actual/observed rate in any given timeframe once vaccination begins.
• Some clustering - a number of cases in a limited timeframe or area - of adverse events occurs normally, and we can expect this clustering to continue during the period that 2009 H1N 1 vaccinations are given.
• By comparing the expected rate of adverse events to the actual/observed rate in any given timeframe, we can put adverse event reports in proper context.
• There are some limitations of background rates. Background rates can vary widely by location, age, sex and ethnlcltv, and therefore these factors should be considered when using background rates to compare events that occur following vaccination.
• Background rates by themselves usually are not sufficient as a way to fully assess vaccine safety. Full analysis requires review of individual reports and carefully controlled epidemiologic study.
• While background rates tell us that we cannot jump to conclusions or assume that any vaccine caused a particular health event, CDC takes every single adverse event report seriously and individually reviews all reports of serious adverse events so that potential problems can be quickly detected and investigated.
Seasonal Influenza Vaccine
• Two systems that look at seasonal influenza vaccinations administered and billed show that many more individuals have been vaccinated this season than at the same time last year. This is most likely due to the early availability of vaccine and public interest in getting vaccinated.
• CDC continues to recommend seasonal flu vaccination. Currently the vast majority of influenza being reported to CDC is 2009 H iN 1. Influenza is very unpredictable but CDC expects both 2009 HiNl flu and seasonal flu to cause illness, hospital stays and deaths this season.
Seasonal Influenza Vaccine Supply and Distribution
• Local areas may not have received as much vaccine as they anticipated at this point in the season and providers seeking additional vaccine now may be unable to purchase it. For more information about seasonal supply, please refer to IVATS (http://www.preventinfluenza.org/ivats/) over the coming weeks.
Page of 10 of 12
2009 H1Nl Influenza Updated Key Points November 6, 2009
• The largest supplier of seasonal flu vaccine, Sanofi Pasteur is experiencing a delay in their shipments. Currently, the company has shipped more than half of the 50.5 million doses of Sanofi Pasteur seasonal flu vaccine ordered by U.S. health care providers. It could be November before customers receive their complete orders.
• CDC is working with manufacturers, states, and immunization providers to identify existing seasonal flu vaccine and get it to providers who can administer it to people who need and want it,
• Most will be able to obtain vaccine from their usual provider, but some will have to obtain the vaccine from an alternative provider
• (Updated) As of October 30, more than 91 million doses of seasonal influenza vaccine have been distributed (this is about 79% of doses expected this season).
• At the current time, five influenza vaccine manufacturers are projecting as many as 114 million doses of seasonal influenza vaccine will be available from currently licensed manufacturers in the United States for use during the 2009-10 influenza season.
• Manufacturer projections indicate that the vast majority of vaccine will be distributed by the end of October. However, some vaccine distribution may continue into November, including doses that are ordered during the fa II.
• CDC's seasonal influenza web Site is at http://www.cdc.gov/flu with a new design, the latest information updates, and free resources.
• (New) More information about seasonal flu vaccine supply can be found
at: http://www .cdc.gov jflu/professionals!vaccination/ #supply
Flu Activity May Occur in "Wavesu
• The timing, spread and severity of influenza viruses is uncertain.
• Outbreaks of influenza may occur in different places at different times.
• Outbreaks may occur in waves of about 6-12 week time periods.
• These waves of influenza may occur over a year or so after the emergence of a new influenza virus.
• In past pandemics, "waves" of activity have been observed.
• The first wave is usually a smaller wave; followed by a larger "peak" wave. Subsequent smaller waves can occur as well.
Page of 11 of 12
2009 H1Nl Influenza Updated Key Points November 6, 2009
• The United States experienced its first wave of 2009 H iN 1 pandemic activity in the spring of 2009.
• At this time, we are experiencing a second wave of 2009 HiNl activltv.
• Flu activity is widespread in most of the country at this time, which is highly unusual during regular seasonal flu for this time of year, but not unexpected for a pandemic.
• Nationally, activity is continuing to increase.
• It's not possible to predict how long activity will remain high, when this wave will peak and when activity will begin to decline.
• Even after flu activity peaks during the current wave, it's possible that other waves of influenza activity may occur - caused by either 2009 H1Nl viruses or regular seasonal flu viruses.
• Because the timing and spread of influenza viruses are unpredictable, CDC is continuing to recommend vaccination with seasonal influenza vaccine and 2009 H1Nl vaccine for those people in whom it is recommended.
Page of 12 of 12
the Influenza
2009-2010 Influenza Season Week 43 ending October 31, 2009
All data are preliminary and may change as more reports are received,
Synopsis: During week 43 (October 25-31) 2009), influenza activity remained elevated in the U.S.
o 5,258 (37.2%) specimens tested by U.S. World Health Organization (WHO) and National Respiratory and Enteric Virus Surveillance System (NREVSS) collaborating laboratories and reported to CDC/Influenza Division were positive for influenza.
o Over 99% of all subtyped influenza A viruses being reported to CDC were 2009 influenza A (H1N1) viruses.
o The proportion of deaths attributed to pneumonia and influenza (P&I) was above the epidemic threshold.
o Eighteen influenza-associated pediatric deaths were reported. Fifteen of these deaths were associated with 2009 influenza A (H1N1) virus infection and three were associated with an influenza A virus for which the subtype was undetermined.
o The proportion of outpatient visits for influenza-like illness (Ill) was above the national baseline. AIL 10 regions reported III above region-specific baseline levels.
o Forty-eight states reported geographically widespread influenza activity, two states reported regional influenza activity; the District of Columbia reported local influenza activity; Puerto Rico and Guam reported sporadic influenza activity, and the U.S. Virgin Islands did not report.
atlona an eglona ummary of elect urver ance ornponen s
Data for current week Data cumulative since August 30, 2009 (Week 35)*
Number of A
HHS Out- % jurisdictions A (Subty-
Surveillance patient positive reporting A (H1) A (H3) 2009 A (unable ping not B Pediatric
Regions""* ILit for flu~ regional or (H1N1) to sub- perfor- Deaths
widespread type)¥ med)
activity§
Nation Elevated 37.2% 50 of 54 18 35 32,814 331 15,285 102 85
Region 1 Elevated 29.6% 60f6 5 2 867 5 138 7 0
Region 2 Elevated 21.6% 20f4 1 5 349 0 251 3 1
Region 3 Elevated 53.4% 5 of6 1 6 6,494 17 815 10 6
Region 4 Elevated 20.8% 8 of 8 ° 1 3,090 56 3,348 13 21
Region 5 Elevated 49.9% 60f6 4 15 5,119 81 861 10 6
Region 6 Elevated 20.4% 5 of 5 0 3 1,977 4 3,234 10 33
Region 7 Elevated 45.3% 40f4 4 1 2,677 136 743 8 1
Region 8 Elevated 40.7% 60f6 2 0 5,053 1 5,112 36 7
Region 9 Elevated 36.9% 4 of 5 0 1 5,438 23 677 3 6
Region 10 Elevated 33.1% 40f4 1 1 1,750 8 106 2 4
, .. N .
dR
IS
S
S
c
t
Influenza season offiCially begins each year at week 40. This season data from week 35 Will be Included to show the trend of Influenza activity before the offiCial start of the 2009-10 influenza season.
**HHS regions (Region 1 CT. ME, MA. NH. RI, VT; Region 2: NJ, NY. Puerto Rico, US Virgin Islands; Region 3: DE, DC, MD, PA. VA, \fIN; Region 4: AL, FL, GA, KY. MS. NC. SC. TN; Region 5: Il, IN, MI, MN, OH, WI; Region 6: AR, LA. NM, OK. TX; Region 7: IA. KS. MO. NE; Region 8: CO. MT, NO. SD. UT. WY; Region 9: AZ. CA. Guam, HI. NV; and Region 10: AK, ID, OR, WA).
t Elevated means the % of visits for III is at or above the national or reqion-speciflc baseline. :j: National data are for current week; regional data are for the most recent three weeks.
§ Includes all 50 states, the District of Columbia, Guam. Puerto Rico, and U.S. Virgin Islands.
¥ The majority of influenza A viruses that cannot be sub-typed as seasonal influenza viruses are 2009 A (H1 N1) influenza viruses upon further testing.
U.S. Virologic Surveillance: WHO and NREVSS collaborating laboratories located in all 50 states and Washington D.C., report to CDC the number of respiratory specimens tested for influenza and the number positive by influenza type and subtype. The results of tests performed during the current week are summarized in the table below.
Week 43
No. of specimens tested 14,151
No. of positive specimens (%) 5,258 (37.2%)
Positive specimens by type/subtype
Influenza A 5,244 (99.7%)
A (2009 H1N1) 3,889 (74.2%)
A (subtyping not performed) 1,310 (25.0%)
A (unable to subtype) 41 (0.8%)
A (H3) 2 (0.0%)
A (H1) 2 (0.0%)
Influenza B 14 (0.3%) During week 43, seasonal influenza A (Hi), A (H3), and B viruses co-circulated at low levels with 2009 influenza A (H1 N1) viruses. Over 99% of all subtyped influenza A viruses reported to CDC this week were 2009 influenza A (H 1 N 1) viruses.
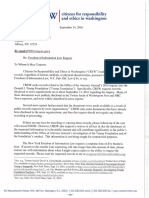
Influenza Positive Tests Reported to CDC by U.S. WHO/NREVSS Collaborating Laboratories, National Summary, August 3D-October 31, 2009
10000 55
~A (2009 H1N1)
9000 ~ A (Unable to Subtype) 50
(/) ~A(H3)
·c 8000 _A(H1) 45
(J) !="'""'~t A (Subtyping not Performed)
E I!l!!ilil'ii!l B
'0 7000 - Percent Pos itive 40
(J)
Q. (J)
(/) 35 :G
(J) 6000 '(7)
> 30 ~
:p
'(7) 5000 ....-
0 c
0... 25 (J)
'+- 4000 2
0 20 ~
I-
(J)
.0 3000
E 15
::1
Z 2000
10
1000 5 o
35 37 39 41 43 45 47 49 51 1 3 5 7 9 11 13 15 17 19
Week
2009-2010 Influenza Season - Week 43, ending October 31, 2009
2
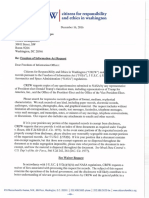
Pneumonia and Influenza Hospitalization and Death Tracking: This new system was implemented on August 3D, 2009, and replaces the weekly report of laboratory confirmed 2009 H1N1-related hospitalizations and deaths that began in April 2009. Jurisdictions can now report to CDC counts of hospitalizations and deaths resulting from all types or subtypes of influenza, not just those from 2009 H1 N1 influenza virus. To allow jurisdictions to implement the new case definition, counts were reset to zero on August 30, 2009. From August 30 - October 31, 2009, 17,838 laboratory-confirmed influenza associated hospitalizations and 672 laboratory-confirmed influenza associated deaths were reported to CDC. CDC will continue to use its traditional surveillance systems to track the progress of the 2009-10 influenza season.
Weekly Laboratory-Confirmed Influenza-Associated Hospitalizations and Deaths, National Summary, August 30 - October 31,2009
4500
~ 4000
g 3500
III
:&11 3000
~
g. 2500
0
:I: 2000
-
0 1500
...
CIi
.!l 1000
E
:::l
Z 500
0
125
0 100
:S
III
(1) 75
0
-
0
..
(1) 50
.!l
E
:::s
z 25
0 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52
Week
2009-2010 Influenza Season - Week 43, ending October 31, 2009
3
Antigenic Characterization: CDC has antigenically characterized one seasonal A (H1N1), two A (H3N2) and 2392009 influenza A (Hi Nt) viruses collected since September 1,2009.
One seasonal influenza A (H1N1) virus was tested and is related to the influenza A (H1Ni) component of the 2009-10 Northern Hemisphere influenza vaccine (NBrisbane/59/2007).
Both influenza A (H3N2) viruses tested showed reduced titers with antisera produced against NBrisbane/10/2007, the 2009-2010 Northern Hemisphere influenza A (H3N2) vaccine component, and were antlgenically related to A/Perth/16/2009, the WHO recommended influenza A (H3N2) component of the 2010 Southern Hemisphere vaccine formulation.
Two hundred thirty-eight (99.6%) of 239 2009 influenza A (H1N1) viruses tested are related to the NCaliforniaJ07/2009 (Hi N1) reference virus selected by WHO as the 2009 Hi N1 vaccine virus and one virus (0.4%) tested showed reduced titers with antisera produced against NCalifornia/07/2009.
Annual influenza vaccination is expected to provide the best protection against those virus strains that are related to the vaccine strains, but limited to no protection may be expected when the vaccine and circulating virus strains are so differenct as to be from different lineages. Antigenic characterization of 2009 influenza A(H 1 N 1) viruses indicates that these viruses are only distantly related antigenlcally and genetically to seasonal influenza A(H1 N1) viruses, suggesting that little to no protection would be expected from vaccination with seasonal influenza vaccine. It is too early in the influenza season to determine if seasonal influenza viruses will circulate widely or how well the vaccine and circulating strains will match.
Antiviral Resistance: Since September 1,2009,2562009 influenza A (Hi N1) virus isolates have been tested for resistance to the neuraminidase inhibitors (oseltamivir and zanamivir), and 628 2009 influenza A (H 1 N 1) original clinical samples were tested for a single known mutation in the virus that confers oseltamivir resistance. In addition, one influenza A (H3N2) and 152 influenza A (Hi N1) virus isolates have been tested for resistance to the adamantanes (amantadine and rimantadine). Additional laboratories perform antiviral testing and report their results to CDC. The results of antiviral resistance testing performed on these viruses are summarized in the table below.
Antlvl IR·t
T
R
s
C II
d S·
S t b 1 2009
n rvira esis ance estmg esu ts on arnpres o ecte mce eptern er , .
Resistant Resistant Resistant
Viruses Viruses, Viruses Viruses, Isolates Viruses,
tested (n) Number (%) tested (n) Number (%) tested (n) Number (%)
Oseltamivir Zanamivir Adamantanes
Seasonal
Influenza A 0 o (0) 0 0(0) 0 o (0)
(H1N1)
Influenza A 0 0(0) 0 0(0) 1 1 (100)
(H3N2)
Influenza B 0 0(0) 0 0(0) N/A* N/A*
2009
Influenza A 884 2t:t: (0.2) 256 0(0) 152 152 (100)
(H1N1) "The adamantanes (amantadine and rirnentadlne) are not effective against Influenza B VIruses.
+Two screening tools were used to determine oseltarnlvlr resistance: sequence analysis of viral genes and a neuraminidase inhibition assay.
;j: Additiona! laboratories perform antiviral resistance testing and report their results to CDC. Two additional oseltamivir resistant 2009 influenza A (H 1 N1) viruses have been identified by these laboratories since September 1, 2009, bringing the total number to 4. One previously reported case was reclassifled after additional te sting did not confirm oseltamivir resistance.
2009-2010 Influenza Season - Week 43, ending October 31, 2009
4
Over 99% of the subtyped influenza A viruses reported during week 43 were 2009 influenza A (H1N1) viruses, and all 2009 H1N1 viruses tested since April 2009 have been resistant to the adamantanes (amantadine and rimantadine).
Antiviral treatment with oseltamivir or zanamivir is recommended for all patients with confirmed or suspected influenza virus infection who are hospitalized or who are at higher risk for influenza complications. Additional information on antiviral recommendations for treatment and chemoprophylaxis of influenza virus infection is available at http://www.cdc.gov/H1N1flu/recommendations.htm.
2009 influenza A (H 1 N 1) viruses were tested for oseltamivir resistance by a neuraminidase inhibition assay and/or detection of genetic sequence mutation, depending on the type of specimen tested. Original clinical samples were examined for a single known mutation in the virus that confers oseltamivir resistance in currently circulating seasonal influenza A (H1N1) viruses, while influenza virus isolates were tested using a neuraminidase inhibition assay that determines the presence or absence of neuraminidase inhibitor resistance, followed by the neuraminidase gene sequence analysis of resistant viruses.
The majority of 2009 influenza A (Hi N1) viruses are susceptible to the neuraminidase inhibitor antiviral medication oseltarnivir; however, rare sporadic cases of oseltamivir resistant 2009 influenza A (Hi Nt) viruses have been detected worldwide. Since September 1, 2009,four cases have been identified in the United States, and a total of 14 cases of oseltamivir resistant 2009 influenza A (Hi N1) viruses have been identified in the United States since April 2009 (11 viruses identified by CDC and three viruses identified by additional laboratories). The 14 total cases include a new case detected from a specimen collected before September 1, 2009, and one previously reported case was reclassified after additional testing did not confirm oseltamivir resistance. All tested viruses retain their sensitivity to the neuraminidase inhibitor zanamivir. Twelve patients (including 10 of the viruses detected at CDC and two viruses identified by the additional laboratories) had documented exposure to oseltamivir through either treatment or chemoprophylaxis, one patient is under investigation to determine exposure to oseltamivir, and one patient had no documented oseltarnivir exposure. Occasional development of oseltamivir resistance during treatment or prophylaxis is not unexpected. Enhanced surveillance is expected to detect additional cases of oseltamivir resistant 2009 influenza A (Hi N1) viruses, and such cases will be investigated to assess the spread of resistant strains in the community.
To prevent the spread of antiviral resistant virus strains, CDC reminds clinicians and the public of the need to continue hand and cough hygiene measures for the duration of any symptoms of influenza, even while taking antiviral medications (http://www.cdc.gov/mmwr/preview/mmwrhtmllmm5832a3.htm).
2009-2010 Influenza Season - Week 43. ending October 31. 2009
5
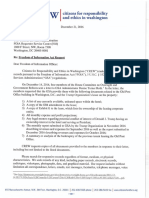
Pneumonia and Influenza (P&I) Mortality Surveillance: During week 43,7.4% of all deaths reported through the 122-Cities Mortality Reporting System were due to P&1. This percentage was above the epidemic threshold of 6.7% for week 43. Including week 43, P&I mortality has been above threshold for five consecutive weeks.
Pneumonia and Influenza Mortality for 122 U.S. Cities Week ending 10/31/2009
12
Epidemic Threshold
06 10 CL
.B
(J) :::::! o C/)
:5 8
co (J)
o
«
'+-
o
'# 6
Seasonal Baseline
2005
2006
2007
\ 2008
2009
4~------------------------------------------------------------
40 50 10 20 30 40 50 10 20 30 40 50 10 20 30 40 50 10 20 30 40
Weeks
Influenza-Associated Pediatric Mortality: Eighteen influenza-associated pediatric deaths were reported to CDC during week 43 (California [8], Indiana, Louisiana [2J, Mississippi, New York, Oklahoma, Texas [2], Virginia, and West Virginia). Fifteen of these deaths were associated with 2009 influenza A (Hi N1) virus infection and three were associated with an influenza A virus for which the subtype is undetermined. These deaths occurred between July 12 and October 31,
2009. Seven deaths reported during week 43 occurred during the 2008-09 season, bringing the total number of reported pediatric deaths occurring during that season to 124. Since August 30, 2009, CDC has received 85 reports of influenza-associated pediatric deaths that occurred during the current influenza season (12 deaths in children less than 2 years old, nine deaths in children 2-4 years old, 30 deaths in children 5-11 years old, and 34 deaths in individuals 12-17 years old). Seventy-three of the 85 deaths were due to 2009 influenza A (H 1 N 1) virus infections, and the remaining 12 were associated with influenza A virus for which the subtype is undetermined. A total of 129 deaths in children associated with 2009 influenza A (H 1 N1) virus infection have been reported to CDC.
Among the 85 deaths in children, 53 children had specimens collected for bacterial culture from normally sterile sites and 17 (32.1 %) of the 53 were positive; Staphylococcus eureus was identified
2009-2010 Influenza Season - Week 43, ending October 31,2009
6
in eight (47.1%) of the 17 children. One S. aureus isolate was sensitive to methicillin, six were methicillin resistant, and one did not have sensitivity testing performed. Twelve (70.6%) of the 17 children with bacterial coinfections were five years of age or older, and five (29.4%) of the 17 children were 12 years of age or older.
20
18
16
14 2006·07
II) Number of Deaths
.J::
- Reported= 78
: 12
"C
- 10
0
...
Cl)
.Q 8
E
:::s
Z 6 Number of Influenza-Associated Pediatric Deaths by Week of Death: 2006-07 season to present
Number of Deaths Reported=85
2007-08
Number of Deaths Reported = 88
2008-09
Number of Deaths Reported= 124
4
2
0
0 >:D N >:D N co '¢ 0 >:D N co N co '¢ 0 >:D N co '¢ a (") m to ,,- t- (") os
-e- '¢ Lf') a ,,- ...... N co (") '¢ '¢ 0 a ...... N ~ (") (") '¢ io a a ..- N N (") C')
, , , , I , , , , , , , , , , , I I , I , , m m I I
<D <D <D t- t- t- t- t- t- t- t- eo 00 co eo eo eo eo co 00 (j) (j) m c» (j)
0 a 0 0 0 0 0 <:) 0 <:) 0 <:) <:) <:) 0 0 0 0 0 <:) <:) 0 a 0 a a 0
0 a <:) 0 0 0 <:) a <:) 0 0 0 a a a 0 a a 0 a 0 0 0 a 0 0 a
N N N N N N N N N N N N N N N N N N N N N N N N N N N
Week of Death lliID 2009 Influenza A (Hi Nt) Deaths Reported Current Week III 2009 Influenza A (Hi N1) Deaths Reported Previous Weeks
II Deaths Reported Current Week Ii Deaths Reported Previous Weeks
Influenza-Associated Hospitalizations: Laboratory-confirmed influenza-associated hospitalizations are monitored using a population-based surveillance network that includes the 10 Emerging Infections Program (EIP) sites (CA, CO, CT, GA, MD, MN, NM, NY, OR and TN) and 6 new sites (lA, ID, MI, ND, OK and SO).
During September 1, 2009 - October 31, 2009, the following preliminary laboratory-confirmed overall influenza associated hospitalization rates were reported by EIP and the new sites (rates include influenza A, influenza B, and 2009 influenza A (H1N1));
Rates [EIP (new sites)] for children aged 0-4 years and 5-17 years were 3.1 (7.3) and 1.5 (2.9) per 10,000, respectively. Rates [EIP (new sites)] for adults aged 18-49 years, 50-64 years, and;:: 65 years were 1.2 (1.2),1.3 (1.2) and 1.0 (1.1) per 10,000, respectively.
2009-2010 Influenza Season - Week 43, ending October 31,2009
7
EIP Influenza Laboratory-Confirmed Cumulative Hospitalization Rates, 2009-10 and Previous Three Seasons*
C:=J 2009-10 Network case count - 2009-10 New sites ~ate. :
-2009-10 EIP rate -2008-09 EIP rate"
-2007-08 EIP rate -2006-07 EIP rate J
7.5 0-4 yr r 300 I
6.0
200
4.5
3.0
100
1.5
~ __ ~o~~~~~~~~~~~~~============~LQ~ __ ~
6 :: 5-17 yr rr :::
i 4.5
1 3.0
r 100
1.5 I
._Q,Q_0.0~. ~:::::::::::::=:~~'* ~~I O:.....__.
~ 7.5 18-49 yr r 300 i
d' 6.0
~ ~ I
! :: 9
~ __:; In n : 00 ~
~ 7.5l 300
50-64 yr
6.0 .
] ~o
4.5
3.0
100
1.5
4.5
200
3.0
100
1.5
o
3537394143454749515324681012141618
Week
* The 2008-09 EIP rate ended as of April 14, 2009 due to the onset of the 2009H 1 N1 season.
2009-2010 Influenza Season - Week 43, ending October 31,2009
8
Outpatient Illness Surveillance: Nationwide during week 43,7.7% of patient visits reported through the U.S. Outpatient Influenza-like Illness Surveillance Network (IUNet) were due to influenza-like illness (Ill). This percentage is above the national baseline of 2.3%.
Percentage of Visits for Influenza-like Illness (Ill) Reported by
the U.S. Outpatient Influenza-like Illness Surveillance Network (ILlNet)) Weekly National Summary) October 1, 2006 - October 31, 2009
9
8
7
6
...J
c-
o 5
'+-
<f)
:t:::
.~
> 4
4-
0
~
0
3
2 O+mmmmrrmrnmrnmmmrr~mmmmmrnmmmm~~m==mmm~mrnmmmrrmmrnmrnm~mmmmrn
~ 0\) ,,\) 1J ,,;)\') ~ ~\') ,,\') ~ ::,\') ~ 0\') ,,\') ~ ~\) \II\')
\.')'0 \.')<0 ~ ~ ~ ~ ~ ",\')'0 ,,\')'0 ,,\')'0 \.')'0 \.')'0 \.')OJ ~ \.')OJ \.')os
~~ ~~~~~ ~~f),,'0~~ ~~~f),,\$
Week
--14-- % III ••• National Baseline
On a regional level, the percentage of outpatient visits for III ranged from 5.0% to 10.7% during week 43, and decreased in five of the 10 surveillance regions compared to the previous week. All 10 regions reported a proportion of outpatient visits for I LI above their region-specific baseline levels.
2009-2010 Influenza Season - Week 43, ending October 31, 2009
9
Region 1 - CT, ME, MA, NH, RI, VT
6 '
Region 2 - NJ, NY, USVI
Region 3 - DE, DC, MD, PA, VA. WV
12
Region 4 - AL, FL, GA, KY, MS, NC, SC, TN
Region 5 - IL, IN, MI, MN, OH, WI
10
Region 6 - AR, LA, NM, OK, TX
Region 7 - IA. KS, MO, NE
Region 8 - CO, MT,. NO., so, UT, WY
Region 9 - AZ, CA, HI, NV
: 1 .
Region 10 - AK, ID, OR, WA
% III
I ••••• I • • Baseline
NOTE: Scales differ between regions
2009-2010 Influenza Season - Week 43, ending October 31,2009
10
Geographic Spread of Influenza as Assessed by State and Territorial Epidemiologists: The influenza activity reported by state and territorial epidemiologists indicates geographic spread of both seasonal influenza and 2009 influenza A (H1 N1) viruses and does not measure the severity of influenza activity.
During week 43, the following influenza activity was reported:
• Widespread influenza activity was reported by 48 states (Alabama, Alaska, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, Florida, Georgia, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, Pennsylvania, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, and Wyoming).
• Regional influenza activity was reported by two states (Hawaii and Mississippi).
• Local influenza activity was reported by the District of Columbia.
• Sporadic influenza activity was reported by Puerto Rico and Guam,
• The U,S. Virgin Islands did not report.
Weekly Influe:nzaActlvityEstimates. Rep.oded by State &; TerritoriafEpidemiologists* ~ek ending'OCtober 31,2009c" Week43
Puerto.RlcO
Guam
<;:,
u.s. Virgin IslandS
.... _
No Report No Activity Sporadic
Local
Regional Widespread
'!. Th1s map.ll'ldicates geographic spread & does netmeasure t\le severity of influenza activity
A description of surveillance methods is available at http://www.cdc.gov/flu/weeklylf1uactivity.htm
Report prepared: November 6, 2009.
2009-2010 Influenza Season - Week 43, ending October 31,2009
11
WHO Collaborating Laboratory Reports
2009-2010 Influenza Season
Update; Friday, November 06,2009
Summary for All Regions
No. of No. of No. (%) of Postivite specimens by
CDC Reporting Specimens Specimens Positive Type/Subtype
Week Laboratories Tested for Influenza A(H11 MIB} AH1SWINE AUNSUB A-Unk B
200935 127 13253 2584 (19.50 ) 2 12 1508 37 1023 2
200936 127 15618 3317 (21.24 ) 1 3 1933 14 1357 9
200937 125 17078 3711 (21.73 ) 5 1 2193 22 1485 5
200938 121 17411 3894 (22.37 ) 4. 8 2418 34 1417 13
200939 117 17997 4910 (27.28 ) 3 6 3199 54 1637 11
200940 109 19672 6525 (33.17 ) 0 3 4591 27 1891 13
200941 110 24171 9057 (37.47 ) 1 0 6107 40 2895 14
200942 100 23772 9329 (39.24 ) 0 0 6976 62 2270 21
200943 74 14151 5258 (37.16 ) 2 2 3889 41 1310 14
Totals 1010 163123 48585 (29.78 ) 18 35 32814 331 15285 102 2009-2010 Influenza Season - Week 43, ending October 31, 2009
12
WHO Collaborating Laboratory Reports
2009-2010 Influenza Season
Updat.e: Friday, November 06,2009
Summary by Region
HHS Region 1 (CT, ME, MA, NH, RI, VT)
No. of No. of No. (0/0) of Positive specimens by
CDC Reporting Specimens Specimens Positive Type / Subtype
Week Laboratories Tested for Influenza A{Hl) AH3 AHlSWINE AUNSUB AUNK B
200935 10 460 12 ( 2.61 ) 0 0 11 0 1 0
200936 10 489 28 ( 5.73 ) 1 1 23 0 3 0
200937 10 678 48 ( 7.08 ) 3 0 43 0 2 0
200938 10 756 43 ( 5.69 ) 1 0 34 2 6 0
200939 10 756 48 ( 6.35 ) 0 0 41 0 5 2
200940 10 779 50 ( 6.42 ) 0 1 46 0 3 0
200941 9 772 145 ( 18.78 ) 0 0 134 0 10 1
200942 8 1017 337 ( 33.14 ) 0 0 301 1 33 2
200943 5 898 313 ( 34.86 ) 0 0 234 2 75 2
Totals 82 6605 1024 ( 15.50 ) 5 2 867 5 138 7
HHS Region 2 (NJ, NY)
No. of No.of . No. (0/0) of Positive specimens by
CDC Reporting Specimens Specimens Positive Type / Subtype
Week Laboratories Tested for Influenza A{Hl} AH3 AHISWINE AUNSUB AUNK B
200935 11 293 15 ( 5.12 ) 1 1 8 0 5 0
200936 11 359 15 ( 4.18 ) 0 0 14 0 1 0
200937 12 465 20 ( 4.30 ) 0 0 15 0 5 0
200938 11 517 14 ( 2.71 ) 0 1 6 0 7 0
200939 11 552 16 ( 2.90 ) 0 1 8 0 7 0
200940 9 634 52 ( 8.20 ) 0 2 31 0 17 2
200941 9 689 81 ( 11.76 ) 0 0 51 0 30 0
200942 10 985 242 ( 24.57 ) 0 0 107 0 134 1
200943 8 532 154 ( 28.95 ) 0 0 109 0 45 0
Totals 92 5026 609 ( 12.12 ) 1 5 349 0 251 3
HHS Region 3 (DE, DC, MD, PA, VA, WV)
No. of No. of No. (%) of Positive specimens by
CDC Reporting Specimens Specimens Positive Type / Subtype
Week Laboratories Tested for Influenza Am!) AH3 AHlSWINE AUNSUB AUNK B
200935 12 1072 128 ( 11.94 ) 1 1 120 0 6 0
200936 12 1464 184 ( 12.57 ) 0 1 169 0 14 0
200937 12 1645 269 ( 16.35 ) 0 0 252 0 15 2
200938 11 1705 343 ( 20.12 ) 0 3 292 6 38 4
200939 10 1467 504 ( 34.36 ) 0 0 453 0 51 0
200940 9 1619 754 ( 46.57 ) 0 0 648 2 104 0
200941 10 3489 1609 ( 46.12 ) 0 0 1450 3 155 1
200942 10 4526 2593 ( 57.29 ) 0 0 2260 2 329 2
200943 6 1645 959 ( 58.30 ) 0 1 850 4 103 1
Totals 92 18632 7343 ( 39.41 ) 1 6 6494 17 815 10 2009-2010 Influenza Season - Week 43. ending October 31, 2009
13
WHO Collaborating Laboratory Reports
2009-2010 Influenza Season
Update: Friday, November 06, 2009
Summary by Region
HHS Region 4 (AL, FL, GA, KY, MS, NC, SC, TN)
No. of No. of No. (%) of Positive specimens by
CDC Reporting Specimens Specimens Positive Type / Subtype
Week Laboratories Tested for Influenza A(Hl} AH3 AHISWINE AUNSUB AUNK B
200935 17 3308 789 ( 23.85 ) 0 0 359 10 420 0
200936 17 3470 896 ( 25.82 ) 0 0 356 3. 534 3
200937 17 3033 767 ( 25.29 ) 0 0 322 3 441 1
200938 18 3109 826 ( 26.57 ) 0 0 393 5 428 0
200939 18 3176 900 ( 28.34 ) 0 1 462 18 417 2
200940 15 2694 745 ( 27.65 ) 0 0 407 5 332 1
200941 16 2503 633 ( 25.29 ) 0 0 310 4 318 1
200942 16 3350 570 ( 17.01 ) 0 0 292 8 267 ,.,
.J
200943 8 1769 382 ( 21.59 ) 0 0 189 0 191 2
Totals 142 26412 6508 ( 24.64 ) 0 1 3090 56 3348 13
HHS Region 5 (IL, IN, MI, MN, OH, WI)
No. of No. of No. (%) of Positive specimens by
CDC Reporting Specimens Specimens Positive Type / Subtype
Week Laboratories Tested for Influenza A(Hll AH3 AHlSWINEAUNSUB AUNK B
200935 17 1100 238 ( 21.64 ) 0 8 163 12 55 0
200936 16 1388 254 ( 18.30 ) 0 0 205 8 40 1
200937 17 1649 272 ( 16.49 ) 0 0 210 5 57 0
200938 15 1744 380 ( 21.79 ) 1 2 280 9 86 2
200939 14 1935 473 ( 24.44 ) 2 4 344 24 98 1
200940 14 2106 784 ( 37.23 ) 0 0 659 5 119 1
200941 13 2518 1187 ( 47.14 ) 0 0 1064 5 116 2
200942 11 2751 1391 ( 50.56 ) 0 0 1196 5 187 3
200943 9 2121 1111 ( 52.38 ) 1 1 998 8 103 0
Totals 126 17312 6090 ( 35.18 ) 4 15 5119 81 861 10
HHS Region 6 (AR, LA, NM, OK, TX)
No. of No. of No. (%) of Positive specimens by
CDC Reporting Specimens Specimens Positive Type / Subtype
Week Laboratories Tested for Influenza A(Hl) AH3 AHISWINE AUNSUB AUNK B
200935 17 3088 619 ( 20.05 ) 0 2 283 1 331 2
200936 17 3816 766 ( 20.07 ) 0 0 252 1 512 1
200937 16 3968 813 ( 20.49 ) 0 1 235 0 577 0
200938 16 4163 778 ( 18.69 ) 0 0 255 1 520 2
200939 14 3631 597 ( 16.44 ) 0 0 168 0 429 0
200940 14 2933 535 ( 18.24 ) 0 0 195 0 339 1
200941 13 2487 480 ( 19.30 ) 0 0 194 0 286 0
200942 10 2094 438 ( 20.92 ) 0 0 267 0 169 2
200943 8 910 202 ( 22.20 ) 0 0 128 1 71 2
Totals 125 27090 5228 ( 19.30 ) 0 3 1977 4 3234 10 2009-2010 Influenza Season - Week 43, ending October 31,2009
14
WHO Collaborating Laboratory Reports
2009·2010 Influenza Season
Update: Friday, November 06,2009
Summary by Region
SHS Region 7 (IA, KS, MO, NE)
No. of No. of No. (%) of Positive specimens by
CDC Reporting Specimens Specimens Positive Type / Subtype
Week Laboratories Tested for Influenza A(HI} AH3 AHISWINE AUNSUB AUNK B
200935 7 601 156 ( 25.96 ) 0 0 100 14 42 0
200936 9 565 137 ( 24.25 ) 0 0 109 2 25 1
200937 7 703 185 ( 26.32 ) 1 0 120 11 52 1
200938 6 746 218 ( 29.22 ) 1 1 172 4 39 1
200939 7 879 329 ( 37.43 ) 1 0 251 8 69 0
200940 5 890 509 ( 57.19 ) 0 0 457 12 39 1
200941 7 1560 762 ( 48.85 ) 0 0 557 25 180 0
200942 8 1716 847 ( 49.36 ) 0 0 635 38 173 1
200943 7 1215 426 ( 35.06 ) 1 0 276 22 124 3
Totals 63 8875 3569 ( 40.21 ) 4 1 2677 136 743 8
HHS Region 8 (CO, MT, ND, SD, UT, WY)
No. of No.of No. (%) of Positive specimens by
CDC Reporting Specimens Specimens Positive Type / Subtype
Week Laboratories Tested for Influenza A(HI2 AH3 AHISWINE AUNSUB AUNK B
200935 16 1643 222 ( 13.51 ) 0 0 104 0 118 0
200936 15 1983 419 ( 21.13 ) 0 0 239 0 177 3
200937 14 2538 550 ( 21.67 ) 1 0 247 0 302 0
200938 15 2591 529 ( 20.42 ) 1 0 287 0 238 3
200939 15 3185 1017 ( 31.93 ) 0 0 520 0 492 5
200940 15 4579 1611 ( 35.18 ) 0 0 778 1 826 6
200941 15 6544 2662 ( 40.68 ) 0 0 1011 0 1643 8
200942 13 4416 1895 ( 42.91 ) 0 0 1046 0 842 7
200943 12 3413 1299 ( 38.06 ) 0 0 821 0 474 4
Totals 130 30892 10204 ( 33.03 ) 2 0 5053 1 5112 36
HHS Region 9 (AZ, CA, HI, NV)
No, of No. of No. (%) of Positive specimens by
CDC Reporting Specimens Specimens Positive Type / Subtype
Week Laboratories Tested for Influenza A(HI} AH3 AHISWINE AUNSUB AUNK B
200935 14 1260 316 ( 25.08 ) 0 0 274 0 42 0
200936 14 1548 490 ( 31.65 ) 0 0 448 0 42 0
200937 14 1680 595 ( 35.42 ) 0 0 565 3 26 1
200938 14 1679 586 ( 34.90 ) 0 1 531 6 47 1
200939 13 1951 795 ( 40.75 ) 0 0 733 2 59 1
200940 13 2554 1212 ( 47.45 ) 0 0 1128 2 82 0
200941 13 2569 1140 ( 44.38 ) 0 0 1008 2 130 0
200942 11 1844 683 ( 37.04 ) 0 0 552 6 125 0
200943 9 1409 325 ( 23.07 ) 0 0 199 2 124 0
Totals 115 16494 6142 ( 37.24 ) 0 1 5438 23 677 3 2009-2010 Influenza Season - Week 43. ending October 31.2009
15
WHO Collaborating Laboratory Reports 2009·2010 Influenza Season Update: Friday, November 06, 2009 Summary by Region
HHS RegioillO (AK, ID, OR, W A)
No. of No. of No. (%) of Positive specimens by
CDC Reporting Specimens Specimens Positive Type / Subtype
Week Laboratories Tested for Influenza A(HI} AH3 AHISWINE AUNSUB AUNK B
200935 6 428 89 ( 20.79 ) 0 0 86 0 3 0
200936 6 536 128 ( 23.88 ) 0 1 118 0 9 0
200937 6 719 192 ( 26.70 ) 0 0 184 0 8 0
200938 5 401 177 ( 44.14 ) a 0 168 1 8 0
200939 5 465 231 ( 49.68 ) 0 0 219 2 10 0
200940 5 884 273 ( 30.88 ) 0 0 242 0 30 1
200941 5 1040 358 ( 34.42 ) 1 0 328 1 27 1
200942 3 1073 333 ( 31.03 ) 0 0 320 2 11 0
200943 2 239 87 ( 36.40 ) 0 0 85 2 0 0
Totals 43 5785 1868 ( 32.29 ) 1 1 1750 8 106 2 2009-2010 Influenza Season - Week 43, ending October 31,2009
16
PNEUMONIA AND INFLUENZA MORTALITY
(Reported from 122 U.S. Cities)
For the Week Ending October 31, 2009
(Week 43)
%OF TOTAL PNEUMONIA INFLUENZA
YEAR WEEK DEATHS EXPECTED THRESH. DEATHS DEATHS DEATHS
2009 35 5.32 5.89 6.32 10304 539 9
2009 36 5.98 5.90 6.33 9249 548 5
2009 37 6.07 5.93 6.36 11250 674 9
2009 38 6.14 5.96 6.39 10848 659 7
2009 39 6.51 6.01 6.44 9878 631 12
2009 40 6.76 6.06 6.49 10766 700 28
2009 41 6.92 6.12 6.55 10175 680 24
2009 42 7.03 6.19 6.62 11068 731 47
2009 43 7.44 6.27 6.70 11136 779 49 2009-2010 Influenza Season - Week 43, ending October 31,2009
17
U.S. Outpatient Influenza-like Illness Surveillance Network (lLINet) 2008-2009 Influenza Season
Update: Friday, October 31,2009
National Summary
. National Baseline: 2.3%
200935 1349 608501 20813 3.42037 3.48544
200936 1365 598810 22297 3.72355 4.06980
200937 1378 684887 26054 3.80413 4.25661
200938 1310 648911 24213 3.73133 4.19316
200939 1321 650218 27924 4.29456 4.91361
200940 1831 773251 43778 5.66155 6.09275
200941 1866 775099 51552 6.65102 7.11748
200942 1824 790770 60357 7.63269 7.87351
200943 1545 676472 50352 7.44332 7.70944 2009-2010 Influenza Season - Week 43, ending October 31, 2009
18
200935 95 63865 257 0.40241 0.63118
200936 95 53335 265 0.49686 0.84598
200937 98 73363 478 0.65155 1.05650
200938 100 75798 619 0.81664 1.06688
200939 101 73501 616 0.83808 1.17527
200940 120 34505 587 1.70120 1.83530
200941 131 33511 901 2.68867 2.74019
200942 127 35594 1956 5.49531 4.94098
200943 118 35184 2246 6.38358 5.67947
HHS 200935 53 89896 1426 1.58628 2.68987
200936 59 91248 1775 1.94525 4.10787
200937 56 95006 1828 1.92409 3.25281
200938 55 100098 2120 2.11792 2.94055
?00939 55 93727 1872 1.99729 2.45894
200940 122 109428 2334 2.13291 2.53822
200941 116 101784 2656 2.60945 4.19748
200942 119 112043 4383 3.91189 6.97877
200943 99 105730 4736 4.47933 9.06849 2009·2010 I nfluenza Season - Week 43, ending October 31, 2009
19
U.S. Outpatient Influenza-like Illness Surveillance Network (ILINet) 2008-2009 Influenza Season
Update: Friday, October 31,2009
Summary by Region
PA VA Baseline: 3.0%
200935 169 82952 1318 1.5889 1.7003
200936 176 90900 2156 2.3718 2.9572
200937 177 101841 2959 2.9055 3.5789
200938 169 94745 3346 3.5316 3.9968
200939 171 87751 3576 4.0752 4.0408
200940 203 106634 5928 5.5592 5.3331
200941 221 120521 8567 7.1083 6.3408
200942 232 121415 14951 12.3140 10.1134
200943 210 117070 14951 12.7710 10.7240 200935 342 129894 9712 7.47687 6.62475
200936 340 126857 9612 7.57704 .6.80238
200937 355 149980 9857 6.57221 6.42875
200938 332 135204 8381 6.19878 5.90545
200939 341 135042 8349 6.18252 6.26950
200940 430 165864 10613 6.39862 6.24031
200941 427 173161 9639 5.56650 5.33821
200942 415 166461 8645 5.19341 4.87857
200943 381 158736 8436 5.31448 4.99848 2009-2010 Influenza Season - Week 43, ending October 31,2009
20
HHSRegionS
200935 200 81020 1513 1.86744 1.75795
200936 209 82658 2068 2.50188 2.34700
200937 207 91566 2229 2.43431 2.33215
200938 206 90202 2183 2.42012 2.20850
200939 193 87724 2421 2.75979 2.40727
200940 264 105664 4681 4.43008 4.08431
200941 260 103991 6397 6.15149 5.80454
200942 250 107545 9754 9.06969 8.86768
200943 218 95711 8268 8.63851 8.62808
HHSRegion6 200936
200937 5142 8.9033 7.2944
200938 132 41479 3445 8.3054 7.6043
200939 137 54848 5458 9.9511 9.4847
200940 200 73550 8676 11.7961 12.5352
200941 201 65451 8600 13.1396 13.2207
200942 193 68697 7444 10.8360 11.1714
200943 139 43301 3926 9.0668 8.7659 2009-2010 Influenza Season - Week 43, ending October 31,2009
21
U.S. Outpatient Influenza-like Illness Surveillance Network (ILINet) 2008·2009 Influenza Season
Update: Friday, October 31, 2009
Summary by Region
HHS Region 7 Baseline: 1.8%
200935 55 13610 516 3.7913 4.1403
200936 60 15278 610 3.9927 4.4792
200937 56 13911 652 4.6869 5.1207
200938 60 17778 933 5.2481 4.9454
200939 61 19431 1002 5.1567 4.7287
200940 117 34113 2512 7.3638 7.1049
200941 116 34669 3685 10.6291 10.6545
200942 116 35347 4054 11.4691 11.7918
200943 95 27040 2141 7.9179 7.7745
HHS Region 8 200935 73 37704 320 0.84872 0.69158
200936 70 34102 522 1.53070 1.38416
200937 70 37783 779 2.06177 1.89509
200938 70 37425 922 2.46359 2.23432
200939 70 39445 1570 3.98023 3.88557
200940 100 53182 3473 6.53041 6.21320
200941 104 51074 4795 9.38834 8.42864
200942 107 52506 4231 8.05813 7.98404
200943 83 35066 1786 5.09325 5.16852 2009-2010 Influenza Season - Week 43, ending October 31,2009
22
U.S. Outpatient Influenza-like Illness Surveillance Network (ILINd) 2008-2009 Influenza Season
Update: Friday, October 31, 2009
Summary by Region
HHS Region 9 Baseline: 2.8%
200935 186 50141 1389 2.77019 2.90471
200936 184 48216 1488 3.08611 3.34221
200937 180 54757 1738 3.17402 3.60581
200938 153 48814 1804 3.69566 3.35550
200939 155 50484 2323 4.60146 4.95502
. 200940 223 76424 3759 4.91861 6.05409
200941 240 79138 5155 6.51394 7.46780
200942 216 79149 3800 4.80107 6.32422
200943 159 48682 2960 6.08028 7.34057 200935 33 7834 380 4.85065 4.8990
200936 37 7167 436 6.08344 4.5691
200937 37 8926 392 4.39166 3.7675
200938 33 7368 460 6.24321 4.8971
200939 37 8265 737 8.91712 7.8739
200940 52 13887 1215 8.74919 8.0931
200941 50 11799 1157 9.80592 10.0118
200942 49 12013 1139 9.48140 9.9386
200943 43 9952 902 9.06350 9.4478 2009-2010 Influenza Season - Week 43, ending October 31, 2009
23
WEEKLY INFLUENZA ACTIVITY ESTI~~TE
REPORTED BY STATE AND TERRITORIAL HEALTH DEPARTMENTS
UNITED STATES INFLUENZA SURVEILLANCE SEASON 2008-09
UPDATE - Week 43 (October 25-31, 2009)
REPORTING AREA WEEK WEEK (;JEEK WEEK WEEK
39 40 41 42 43
REGION 1
MAINE REGIONAL REGIONAL liHDESPR liJIDESPR WIDESPR
N.H. IrVIDESPR WIDESPR liHDESPR WIDESPR WIDESPR
VERMONT LOCAL REGIONAL vJIDESPR WIDESPR WIDESPR
MASS. REGIONAL REGIONAL WIDESPR WIDESPR \'i'IDESPR
R.1. REGIONAL REGIONAL WIDESPR WIDESPR \I\lIDESPR
CONN. REGIONAL REGIONAL REGIONAL WIDESPR IrHDESPR
REGION 2
NEW YORK WIDESPR vHDESPR WIDESPR WIDESPR WIDESPR
NEW JERSEY REGIONAL REGIONAL REGIONAL IrHDESPR WIDESPR
PUERTO RICO LOCAL LOCAL LOCAL LOCAL SPORADIC
VIRGIN IS. NO REPT. NO REPT. NO REPT. NO REPT. NO REPT.
REGION 3
PENN. WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
DELAWARE WIDESPR WIDESPR WIDESPR II\lIDESPR WIDESPR
MARYLAND vHDESPR WIDESPR lri'IDESPR WIDESPR WIDESPR
D.C. LOCAL LOCAL LOCAL LOCAL LOCAL
VIRGINIA liJIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
W. VIRGINIA REGIONAL WIDESPR WIDESPR WIDESPR WIDESPR
REGION 4
N. CAROLINA WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
S. CAROLINA It\1IDESPR REGIONAL REGIONAL REGIONP,L WIDESPR
GEORGIA WIDESPR WIDESPR liHDESPR WIDESPR WIDESPR
FLORIDA WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
KENTUCKY WIDESPR WIDESPR WIDESPR WIDESPR l;AJIDESPR
TENNESSEE WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
ALABAMA WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
~lISSISSIPPI WIDESPR WIDESPR WIDESPR WIDESPR REGIONAL
REGION 5
OHIO I'lIDESPR WIDESPR vHOESPR WIDESPR WIDESPR
INDIANA tAJIDESPR WIDESPR· vHDESPR WIDESPR WIDESPR
ILLINOIS WIDESPR WIDESPR WIDESPR WIDESPR liHDESPR
MICHIGAN REGIONAL REGIONAL WIDESPR WIDESPR WIDESPR
WISCONSIN REGIONAL WIDESPR WIDESPR tAJIDESPR WIDESPR
MINNESOTA WIDESPR IrHDESPR WIDESPR WIDESPR WIDESPR
REGION 6
ARKANSAS WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
LOUISIANA WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
OKLAH0l'1A WIDESPR WIDESPR WIDESPR tti1IDESPR WIDESPR
TEXAS WIDESPR Il\lIDESPR WIDESPR WIDESPR WIDESPR
NEW MEXICO vHDESPR WIDESPR WIDESPR loll DESPR WIDESPR 2009-2010 Influenza Season - Week 43, ending October 31, 2009
24
REGION 7
IOWA WIDESPR WIDESPR WIDESPR %'IDESPR WIDESPR
MISSOURI WIDESPR liiTIDESPR WIDESPR vHDESPR WIDESPR
NEBRASKA WIDESPR WIDESPR WIDESPR IrHDESPR WIDESPR
KANSAS WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
REGION 8
NORTH DAKOTA REGIONAL WIDESPR WIDESPR WIDESPR WIDESPR
SOUTH DAKOTA WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
MONTANA REGIONAL WIDESPR liHDESPR WIDESPR WIDESPR
WYOMING WIDESPR WIDE3PR WIDESPR vJIDE3PR WIDESPR
COLORADO \'i'IDESPR WIDESPR WIDESPR vHDESPR WIDESPR
UTAH REGIONAL WIDESPR WIDESPR WIDESPR loJIDESPR
REGION 9
ARIZONA WIDESPR WIDESPR vHDESPR WIDESPR lti1IDESPR
NEVADA WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
CALIFORNIA WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
HAWAII LOCAL LOCAL LOO.L REGIONAL REGIONAL
GUAM REGIONAL REGIONAL REGIONAL REGIONAL SPORADIC
REGION 10
IDAHO WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR
WASHINGTON WIDESPR WIDESPR l'i'IDESPR WIDESPR WIDESPR
OREGON TJilIDESPR WIDESPR WIDESPR ~nDESPR WIDESPR
ALASKA WIDESPR WIDESPR WIDESPR WIDESPR WIDESPR Activity Level ILL activity*/Outbreaks Laboratory data
No activity Low And No lab confirmed cases'
Not increased And Isolated lab-confirmed cases
Sporadic OR
Not increased And Lab confirmed outbreak in one institution"
Increased ILL in 1 Recent (within the past 3 weeks) lab
region**; ILL activity in And evidence of influenza in region with
other regions is not increased ILl
increased
Local OR
2 or mOre institutional Recent (within the past 3 weeks) lab
outbreaks (ILl or Lab. evidence of influenza in region with the
confirmed) in 1 region; And outbreaks; virus activity is no greater
ILl activity in other than sporadic in other regions
regions is not increased
Increased ILl in ::2 but Recent (within the past 3 weeks) lab
less than half of the And confirmed influenza in the affected
Regional regions regions
(doesn't apply OR
to states with Institutional outbreaks Recent (within the past 3 weeks) lab
$4 regions) (ILL or lab confirmed) in confirmed influenza in the affected
~2 and less than half of And regions
the regions
Increased ILl and/or Recent (within the past 3 weeks) lab
institutional outbreaks confirmed influenza in the state.
Widespread (ILl or lab confirmed) in And
at least half of the
regions • ILl activity can be assessed using a variety of data sources including sentinel providers, school/workplace absenteeism, and other syndromic surveillance systems that monitor influenza-like illness.
, Lab confirmed case = 'case confirmed by rapid diagnostic test, antigen detection, culture, or peR. • Institution includes nursing home, hospital, prison, school, etc.
'*Region: population under surveillance in a defined geographical subdivision of a state.
2009-2010 Influenza Season - Week 43, ending October 31,2009
25
Norris. Katherine S. (Taffy) (CDC/DCDD/DD)
From:
Sent:
To:
Subject:
Glass, Marquisette L. (CDC/CCEHIP/NCIPC) Monday, September 14, 20093:15 PM Smith, Amanda (HHS{ASPR/OPSP)
RE: Call at Capacity - CDC H1 N1 Vaccine Task Force briefing
Importance:
High
Good afternoon, my apologies. The phone line reached it's capacity and many people were unable to connect. We are having another briefing this afternoon from 4:00-4:30pm, for people who could not get on the call earlier. This is a follow up from August 27, H1 N1 distribution briefing held in Washington, DC.
Fed-DeptAgency_v ax_plan_v6.ppt. ..
Fed_employee_ vax _program_v4.do ...
Thank you,
Marquisette Glass 404-553-81 07
I (b)(2)
Tel econfereo ce NIl m bec
Marquisette Glass
HINl Vaccine Task Force
Centers for Disease Control and Prevention 404-553-8107 (Office)
grp2@cdc.gov
Shimabukuro, Tom (CDC/CCID/NCIRD) Monday, September 14, 2009 3: 12 PM
Smith, Amanda (HHS/ASPR/OPSP)i Glass, Marquisette L. (CDC/CCEHIP/NCIPC) RE: Call at Capacity· CDC H1Nl Vaccine Task Force briefing
From:
Sent:
To:
Subject:
HHS
HHS
-----Original Appointment-----
From: Glass, Marquisette L. (CDCjCCEHIPjNCIPC) Sent: Monday, September 14, 2009 8:08 AM
To: Glass, Marquisette L. (CDCjCCEHIPjNCIPC); Stanley, Toscha (CDCjCCIDjNCIRD); Shimabukuro; Tom (CDCjCCIDjNCIRD); AARON PENDLETON; Smith, Amanda (HHSjASPRjOPSP); AMY RHODES; ANDREA POULIOT; ANDREW LONG; ANDREW MCDONALD; ANDREW MURPHY; ANGELA BROWN; BAHAR MAKANi BEN HERRICK; BENNISE LESTER; BONNIE TIMKO; BRIAN MONAHAN; BRIEN GIBNEY; CAMILLE CARRAWAY; CARMEN CRADDOCK; CATHY ANGOm; CHARLES BENARD; CHARLES STRUCKMEYER; CHERYL FORD; Jones, Cheryl (ACF); chuck young; CISAR GARCIA; COLLEEN PEREZ; CYNTHIA ADAMS; CYNTHIA MCCLAM; DANIEL EARLY; DAVID H. REID III; DAVID WADE; DAWN MCCARTHY; DEBORAH RIZZO; DELORA FLAGG; DENISE RICHARDSON; DONALD L. NOAH; DONNA LEIGHTON; DONNA SPECKHARD; DOUGLAS JONES; DOUGLAS MCGUCKIN; DOUGLAS RUPARD; DYANN A. WAUGH; EDITH COLLINS; ERIC KRm; ERICA SCHWARTZ; FAYE BRESLER; FRANCIE IWAMURA; FRANCIS BACKFIELD; FRANK DENNY; GEORGE KARP; HANK OLTMANN; HARVEY BALL; HELEN VETTORI; JAMES REDINGTON; JANE KELLY; JASON RADDF; JEFF GIUFFRIDA; JENNIFER MCKELVEY; JESUS CANTU; JILL COLBURN; JILL LEWIS; JILL NISSAN; JIM ARMIGER; JOETTE DURHAM; JOHN BRENNAN; JOHN KEYES; JOSEPH M GERHART; Raiti, Joseph (AHRQ); JUANDA SMITH; JUDITH SIBERT; JUDITH SULLIVAN; Blumenthal, Judy (HHSjASPRjOPEO); JULES R. DUVAL; KATHLEEN GARITY; KATHRYN BERNDSTON; KEITH MUMMA; Forde, Kent (HRSA); KIM SMITH; KIMBERLY MOORE; KRISTEN COSTA; Gillham, Kristin (HHSj ASAM); LINDA CROSS; LISA WADE-YOUNG; LLOYD ROBERTS; LONTINA ARTIS; LUCY CUNNINGHAM; MARGE ISLEY; Price Detherage, Maria (HHSjOMHA); De!owery, Mark (PSC); MARK HARTZ; MICHAEL HORAN; MICHELLE ADAMS; MIKE HAVRILESKO; NORMAN FRANKLIN; pATRICIA EVANS; PATRICK OTT; PAUL SMAGH; PAULA CARTER; PAULINE KUEBLER; PAVLA DECOTEAU; PETER GARCIA; PETER TORRES; RALPH BROWN; REGINALD IRBY; REX WAMSLEY; RICHARD
DENDY; RICHARD MILLER; Gruhot, Robert W. (FDA); ROBERT CLAUS; Velasco, Robert (HHSjOMHA); ROBYN L. KENNEDY; ROMEYN ROWLSON; RON BRAVEMAN; Correa-de-Araujo, Rosaly (HHS/IOS); ROSE WILDER; RUSSELL ROWE; SAMANTHA WILLIAMS; SAMUELS C. ANDACE; SANDRA M. CHARLES; SARAH SCRUGGS; SCOTT ROSS; SCOTTER SLADE; SHARON DOBSON; SHERIDAN EASTERLING; SHIRA FLAX; STAN RIGGENBACH; STEPHEN ECK; STEPHEN HASELTON; SUZANNE PIPER; TAIWO CARMICHAEL; Kim, Theodore (HHSjDAB); Yee, Ted (CDC dol.gov); THOMAS FERRANTI NO; TOM YUN; TONYA TEMPLETON; VALERIE ROBERTSON; VICTORIA DAVEY; Holland, Vincent (HHSjASPRjOPEO); VINCENT MICHAND; WALLY BIERSACK; WENDY DAVIS; Jackson, Zhoowan (HHSjASPRjOPEO)
Cc: Blumenthal, Judy (HHSjASPR/OPEO); 'Sibert, Judith'; 'Benard, Charles (OST)'; 'OTT, PATRICK P': 'Iwamura Francie A'; Velasco, Robert (HHS/OMHA); 'Brennan, John'; Kim, Theodore (HHSjDAB); 'RICHARD MILLER (HRT)'; 'Reid, David H - Washington, DC; 'Dobson, Sharon (OST),; Raiti, Joseph (AHRQ); 'Cross, Linda (OST)'; 'Scruggs, Sarah 1.'; Forde, Kent (HRSA); 'Wamsley, Rex'; 'Gerhart, Joseph M'; 'Slade, Scooter'; Catherine.m.Angotti; 'Gibney, Brien R.'; 'Carraway, Camille'; 'Roberts, Lloyd C HQ02'; 'McKelvey, Jennifer (HRjPPIM)'; 'Piper, Suzanne'; Correa-de-Araujo, Rosaly (HHSjIOS); 'Claus, Robert'; 'Queen, Tracy'; 'Easterling, Sheridan B.'; Yee, Ted (CDC dol.gov); 'Irby, Reginald'; 'RAJPAUL SMAGH (TSD)'; 'Jones, Douglas'; 'Evans, Patricia, , WHSjHRD'; 'Grubach, Chris'; 'Duval, Jules'; 'Rizzo, Deborah S'; 'Isley, Marge'; 'Bresler, Faye CIV DLA J-18'; 'McGuckin, Douglas'; 'Vettori, Helen'; 'ROSS, SCOTT K'; 'Arthur, Marty'; 'Pray, Keith'; 'Stringer, Connie'; 'Triplett, John C'; 'RUPARD, DOUGLAS H'; 'Kretz, Eric'; 'Radonovich, Lewis'; 'Cantu Jesus I TIGTA'; 'Adams, Michelle'; 'NORWOOD, Eleanor'; 'Longmire, Atkinson - OSHA'; Delowery, Mark (PSC); 'Waugh, Dyann A - Washington'; 'Greemore, Susan 1.'; 'Martinello, Richard'; 'Bearse, Ronald'; 'Wade, David S.'; 'Speckhard, Donna <CTR>'; 'Kennedy Robyn'; 'Sullivan, Judy (USMS)'; 'Noah, Donald, Col, OASD(HA)'i 'Harrison, Linda S.'; 'Gunnelsl Dale'; 'Pendleton, Aaron C.'
Subject: Updated: CDC HIN1 Vaccine Task Force briefing
When: Monday, September 14, 2009 2:00 PM-3:00 PM (GMT-05:00) Eastern Time (US & Canada). Where: Telecoference: 877-306-6286, pin: 6650537
Good afternoon, this is a follow up from August 27, Hi N1 distribution briefing held in Washington, DC.
2
«File: Fed-DeptAgency_vax_plan_v6.ppt»
Thank you,
Marquisette Glass 404-553-81 07
Teleconference Number:
l(b)(2)
« File: Fed_employee_vax_program_v4.doc »
3
0
(J)
o
._
> ~
...
(J)
(f)
-
J: ......... 0
.c +' 0 (J)
,.. - +' 0
as
IIlII!IIlIIIII (J) C 0
ftS (J)
C/) :x: E '"C
Q) Cl) 0
0 - ::l
'c ca· tn ... (J)
:c (J) -
Q) +' CI) CI) .....
(/) C ._ '"C ... -
(J) CI) (.) ._ C) ca
c - >
co m e E e ca e
E ._ CI) 0 0
:J C > e C) ... > tn s:
I ... Q. o +-'
0 (J) 0 ca CO ~
'"0 e
C (f) ... --. CI) CI) <D
~ lUll. ._ ·0 ...., CI) I
.r::. .. J: > ...., as C) tn ~
+-' CU ...., e e > ca 0 c
CO - W CI) .- 0 0
Q) a- CO ... ... '"§
I (J) '"C E tn Q. CI) 0
'+- ::s ... +' In 0..
0 :x: e +'"' (J) 0 e 0 :J
U ... 0
+-' as ctI ...., .- 0 0
c 0
Q) CJ e Q. c: 0 (J) C\I 0
E .- In (J)
- a. CI) M - l CO
t 0 .c e .c $,...
~ « '"C Q)
0- ::l ..... ca ... '"0
Q) a.. w 0 J: 0 tn CI) Q)
0 -- +'"' ...., 1J._
f! CD - ~ ... tn
. (f) In CO ::l
(/) - M ... "- :I:
:::> :J CO (J) 0 .c e
e CI) J: E ....
--. 3: E
(f) .- > 01
" e ... 0 ...., .-
"" :r: ._ (J) CI) CI.) '"C
"" 0
g - a:: <C
~ :.t: 0 (f) M Z I.L.
1;1. LL.
'7;'1· f'q ii Iili
'?.y\l'IU;J\,·:l\_\~) Iii Iili m III II September 14, 2009
Proposed 2009 HINl vaccination program for the Federal workforce
Key points from the Centers for Disease Control and Prevention (CDC):
• The Department of Health and Human services (RHS) is in the planning stages for a program to provide HINI vaccine to the Federal workforce in Federal occupational settings
• No final decisions have been made at this point on the scope and scale of a program
• However, HHS is moving forward on coordinating with Federal departments/agencies on implementation planning due to the short timeline
• Federal departments/agencies have several options for receiving vaccine
• Register with and order through the CDC (Marquisette Glass, HINIFedAgcncy@cdc.gov)
• Use existing agreements or establish new agreements with Federal Occupational Health (FOH), (Marcia Furey, 301-594-0246, Marcia.Furey@foh.hhs.gov)
• Contract directly with HRS's Supply Service Center at Perry Point, MD' (Annette Quinones, 410-642-1386, Annette.Ouinones(wpsc.hhs.gov). This option is suggested for those agencies who have existing occupational health programs and providers (other than FOH) who can store\administer vaccine
• Negotiate receipt of vaccine for healthcare workers and emergency medical services personnel through the Department of Veterans Affairs" at VA medical centers (VHA HIN1 Coordination Center, VHAH1NICC@va.gov)
• Refer employees to their doctor, the local health department or other state-based programs (outside of the Federal system)
"FOH, Perry Point and the Department of Veterans Affairs will be receiving vaccine through CDC. Vaccine supply is eventually expected to be sufficient to support additional vaccine requests from additional department/agency demand
• CDC can support shipping vaccine to a limited number of sites, so Federal departments/agencies wishing to order through CDC may have to do a substantial amount of internal redistribution to occupational clinics
• The number of ship-to sites allocated to Federal departments/agencies is to be determined and will be based on department/agency size
• In general, to make the program logistically feasible, CDC may only be able to ship to large Federal departments/agencies (thousands of employees)
• Federal departments/agencies wishing to receive vaccine directly from CDC should be able to receive, store, possibly repackage and redistribute, and internally administer or contract for administration of potentially large amounts of vaccine
• For smaller Federal departments/agencies, CDC recommends contracting with FOH or HHS's Supply Service Center at PelTY Point, MD, which can support smaller and more customized orders
" CDC will be in contact shortly with department/agency points of contact to gather information for the allocation and ordering process (CDC prefers to work with a single POC at the Department level)
Norris. Katherine S. (Taffy) (CDC/OCOO/OD)
From:
Sent:
To:
Cc:
Shimabukuro, Tom (CDC/CCID/NCIRD) Friday, September 18, 20091 :39 PM
Barnes, Bethanne (HHS/ASPR/RPE); Helminiak, Clare (HHS/ASPR/OPEO)
Goldhaber, Benjamin (HHS/ASPR/RPE); Chavez, IIka (HHS/ASPR/OPSP); Smith, Amanda (HHSjASPR/OPSP): Pereira, Esmeralda (HHS/ASPR/RPE)
RE: Federal Workforce Vaccine - OMB Questions
Subject:
Bethanne,
It looks good to me. Thanks for pulling this together.
Tom
Tom T. Shimabukuro, MD, MPH, MBA CDR, U.S. Public Health Service Pandemic Influenza Vaccine Coordinator
Health Services Research and Evaluation Branch Immunization Services Division
National Center for Immunization and Respiratory Diseases Centers for Disease Control and Prevention (CDC)
Phone: 404-639-8542
Fax: 404-639-8614
Email: TShimabukuro@cdc.gov
Regular mail: 1600 Clifton Road, MS E-~2 Atlanta G.;\ 30333
Express mail: 12CorporateSquareBlvd(b)(2)JAtlanta.GA 30329
HHS
HHS
From: Shimabukuro, Tom (CDCjCCID/NCIRD) Sent: Wednesday, September 16, 20095:41 PM
To: Helminiak, Clare (HHSjASPRjOPEO); Barnes, Bethanne (HHS/ASPRjRPE)
Cc: Goldhaber, Benjamin (HHS/ASPR/RPE); Chavez, Ilka (HHS/ASPRjOPSP); Smith, Amanda (HHS/ASPR/OPSP) Subject: RE: Federal Workforce Vaccine - OMB Questions
Just some comments to go along with Clare's responses.
1. Since federal agencies will be able to order vaccine directly, will other large companies? If not, why?
No, the private sector orders thru the State Depts of Public Health which control vaccine flow to the States. Vaccine will be shipped to clinics, offices, health departments, and other project area-designated sites which may include a mix of public health and private sector sites via centralized distribution. This is the same process that is used to ship vaccines for the childhood immunization program to immunization providers. CDC's centralized distribution mechanism will be substantially enhanced to provide capacity for this activity in addition to shipping of other vaccines. Vaccine is allocated to states on a pro rata basis for distribution and dispensing according to state influenza plans. Corporations may not receive medical countermeasures (including vacoines and antivirals) directly from the federal government. Medical countermeasures are provided to the states and are subsequently dispensed according to existing state plans. States working with the stakeholders in their jurisdictions determine the appropriate strategies for distribution and dispensing of medical countermeasures.
TTS: BUsinesses withoccupational health clinics that wish to provide vaccine for their workers have the option to register with the state health department and request vaccine like other vaccine providers in a state. CDC has encouraged state and local health departments to work with large employers and incorporate them into their
2
planning. Additionally, state or local government agencies may also order vaccine for and conduct vaccination clinics for their workforce.
2. Does the federal government have the data to centrally determine the number of workers in the priority populations at each agency? Who has this data?
No. Each Dept put in a request and we will have to have CDC responds as to how they calculated the pro rata allocation to each Dept.
TTS: CDC is primarily concerned with quantifying the number of healthcare workers and emergency medical services personnel in depts/agencies where providing direct patient care is a large part of their day-to-day operations. Adjustments in the initial shipments to these depts/agencies will be made to account for the high number of HCW/EMS. This really involves VA, IHS, NIH, DOD, BOP, FOH and maybe a few others. We assume other ACIP target groups are evenly distributed across agencies so pro rata should be sufficient.
3. Otherwise, will agencies be asked to come up with these estimates on their own? How will they know?
In HHS each agency had to determine their own tiered numbers.
TTS: CDC will distribute vaccine on a pro rata or modified pro rata basis based on dept/agency size with some initial modification for depts/agencies with high
numbers of HCW/EMS. Implementing vaccination will be the responsibility of the dept/agency.
4. How will the allocations to federal agencies be factored into the State's allocations, since federal workers are located across the country. Also, will these allocations particularly skew vaccines needed in DC/MDNA?
The vaccine for the 3M Feds was taken out of the total vaccine order for the country. Each dept is working with CDC as to how to get their vaccine. If a dept uses FOH they can get the vx thru that, or deal directly with Perry Point, or work with their private occupational health clinics. CDC is working with one poe for each Fed dept.
TTS: The federal workforce is -0.96% of the total U.S. population. When factored in to the overall pro ratas, that reduces grantee pro rata allocations by a fractions of a percent, so in the grand scheme the federal allocation in negligible.
HHS
HHS
HHS
5
Norris, Katherine S. crafty) (CDC/OCOO/OD)
From:
Sent:
To:
CDC IMS JIC Public Health Workforce (CDC) Wednesday, August 19, 2009 1 :20 PM
Basket, Michelle (CDC/OSELS/NCHM); Harrison, James R. (CDC/CCID/NCIRD); Hill, Antonette Y. (CDC/OID/OD); Janssen, Alan (CDC/OSELS/NCHM); Lennon, Tanya (CDC/OID/NCIRD); McCauley, Mary (CDC/OSELS/NCHM); 'Melissa Talbot'; 'Phyllis Kim'; Smith, Jean Clare (CDC/OID/NCIRD); 'Bob Davis'; Buschick, Jennifer (HHS/OPHS); CDC
IMS Chief Of Staff; 'Chad Wood'; Cohen, Mitchell L. (CDC/OID/OD); 'Elizabeth Lautner'; EOC Report (CDC); Fauci, Anthony (NIH/NIAID) [E); Gomez, Thomas M. (CDC/OID/NCZVED); Hall, Bill (HHS/ASPA); Helfand, Rita (CDC/OID/NCPDCID); 'John Korslund'; Kane, Eileen (HHS/ASPR/OPSP); Krull, Andrea (HHS/OPHS); 'Lyndsay Griffin'; Marshall, Stephanie (HHS); Mayfield, Evan D. (CDC/OCOO/OD); Michael, Gretchen (HHS/ASPR/OPSP); Migliaccio, Kate (HHS/OPHS); Moreno, Julie (HHS/OS); 'National JIC'; Pickering, Larry (CDC/OIDJNCIRD); Smith, Amanda (HHS/ASPR/OPSP); Sosin, Dan (CDC/OPHPR/OD); 'Stan Health'; Zaza, Stephanie (CDC/OPHPR/OD); 'Anna Buchanan'; 'ASTHO info center'; Bhatt, Achal (CDC/OID/NCIRD); Burns, Erin (CDC/OID/NCIRD); CDC IMS State Health Department Branch Director(CDC); Evans, Victoria (CDC/OID/NCIRD); Lemmings, Jennifer (CDC cste.org); PSC Jennifer Joseph; Kilgus, Duane (CDC/OID/NCIRD); Robinson, LaKesha (CDC cste.org); Kan, Lilly (CDC naccho.org); McConnon, Patrick (CDC cste.org); 'Paul Etkind'; 'Richard Hughes'; Fasano, Nancy (CDC/OID/NCIRD); Harton, Elizabeth (CDC/OID/NCPDC1D); NCIRD Immunization GranteeMailbox(CDC);Pope.Kristin (CDC/OID/NCIRD); Rodewald, Lance (CDC/OID/NCIRD); Whitehead, Cynthia (CDC/OID/NCIRD)
'Iespino@nphic.org'
Talking Points on CDC's novel Hi N1 business guidance Talking Points on Business Guidance 8-19-09BS-FINAL.doc
Cc:
Subject:
Attachments;
Helle, CDC Partners:
Here are CDC's talking points on the business guidance related to novel Hi Nt influenza that CDC released today. This guidance is available at http://www.cdc.gov/h1n1flu/business!guidance! and a toolkit for businesses and
employers related to the guidance is avallable at http:Uwww.cdc.gov!h1n1flu!business/toolkit/.
Please share this information as needed with your partners. The talking points can be used to help field media inquiries.
Best,
Nadya BeJins
Public Health Workforce Team Lead Centers for Disease Control and Prevention Joint Information Center
404.838.7179
Talking Points on CDC's Guidance for Businesses and Employers to Plan and Respond to the 2009·2010 Influenza Season
August 19, 2009
Toptine Messages
• CDC is releasing new guidance that recommends response and planning actions that non-healthcare employers can take now under current flu conditions. These actions will help promote a safer workplace environment for their employees and help maintain continuity in the workplace during the 2009-2010 flu season. The guidance also includes additional strategies to use if flu conditions become more severe.
1
• The new guidance provides recommendations on ways to decrease the spread of seasonal flu and 2009 H1N1 flu in the workplace while making sure businesses can continue to operate as normally as possible.
• Employers should use this guidance to plan for flu now. This includes 1) developing a flexible flu response plan and related workplace policies, or reviewing and revising an existing pandemic flu plan; 2) making sure employees are involved in the development and review of the plan; and 3) testing key components of the plan.
• This guidance provides a menu of tools employers can use to fight flu, in coordination with local health officials-based on local flu conditions and based on what CDC and other public health organizations know about seasonal flu and are learning about the 2009 H1N1 flu virus.
, We know far more about the 2009 HlN1 flu virus than we did when it arrived in April. But we don't yet know what will happen with 2009 HlNl flu in the fall and winter. It could remain at levels similar to what we saw last spring and what has continued into the summer. It could go away entirely, or it could get worse.
• Given ongoing 2009 HINl flu activity this summer, in combination with circulating seasonal flu in the fall and winter, the CDC anticipates more flu cases, hospitalizations, and deaths.
• Because we can't predict how severe 2009-2010 flu season will be, given the impact of seasonal flu and 2009 HINl flu, this guidance is designed to help employers plan for and respond to a continuation of the current flu situation and a more severe outbreak.
• There are things employers can do now to prevent the spread of flu in the workplace and keep their businesses operating as normally as possible. All people with flu-like symptoms should stay home and away from the workplace, hand washing and respiratory etiquette should be encouraged, and routine cleaning of commonly touched surfaces should be performed regularly.
• During a more severe outbreak, employers should take steps to keep people physically apart to reduce the spread of illness (called social distancing). This may include canceling business-related meetings or large gatherings, spacing workers farther apart in the workplace, canceling non-essential travel, and implementing work- from-home strategies.
• CDC and its partners will continue to monitor the spread of flu, the severity of the illness it's causing, and whether the virus is changing. We will provide updates on any changes, revise guidance as needed, and provide further advice to state and local agencies on steps to take.
• Because the 2009-2010 flu season could change rapidly, CDC recommendations may be revised quickly. Employers should make sure they have access to timely and accurate information so that they are aware of changes to the recommendations and can promptly implement any additional measures as a result.
Steps Businesses Can Take Now for Current Flu Conditions
• People who are sick or become sick with flu-like symptoms
o Advise workers to check themselves for any signs of sickness before reporting to work each day; this includes healthy employees with a family member at home with flu.
o People with flu-like symptoms should be separated from other employees and sent home promptly.
They should stay home until at least 24 hours after they are free of fever (100 degrees Fahrenheit or 38 degrees Celsius) or signs of a fever (have chills, feel very warm, have a flushed appearance, or are sweating), without the use of fever-reducing medicines.
o Review sick-leave policies and consider making them flexible and consistent with public health recommendations. Make sure employees are well-aware of these policies.
o Try to provide flexible workplace and leave policies for workers who may need to stay home to care for sick family members or care for children if schools are dismissed.
o Provide information to employees overseas about what to do if they become sick.
e Hygiene/respiratory etiquette
2
o Employees should wash their hands often with soap and water, especially after coughing or
sneezing; alcohol-based hand cleaners can be used if soap and water are not available.
o Employees should cover coughs and sneezes with a tissue; if possible,
o Employers should provide tissues and no-touch disposal receptacles for employees.
LIf no tissues are available, encourage employees to cough or sneeze into their arm or sleeve.
• Routine cleaning
o Frequently clean all commonly touched surfaces in the workplace, such as workstations, countertops, and doorknobs.
o Use the cleaning agents that are usually used in these areas and follow the directions on the label.
No additional disinfection beyond routine cleaning is recommended.
• Take measures to protect people at higher risk of flu complications
o Employees at higher risk of complications from flu should check with their healthcare provider for advice or if they become sick; early treatment with antiviral medicines can prevent hospitalizations and deaths. People at higher risk include pregnant women; children under 5 years of age; adults and children with chronic medical conditions (such as asthma, heart disease, or diabetes), and people 65 years of age or older.
• Vaccination
o When seasonal flu vaccine is available, consider offering it to all employees who want to reduce the risk for becoming sick with flu. If possible, offer seasonal flu vaccination opportunities at the worksite. Employees at higher risk for 2009 H1N1 flu complications should be encouraged to receive the 2009 H1Nl flu vaccine when it becomes available.
• Plan how to maintain business operations with a reduced staff
o Plan to maintain business operations if a large number of employees are home sick or are staying home to care for sick family members or children dismissed from school.
o Make contingency plans for when a lot of employees will need to stay home from work; this could include cross-training employees and hiring temporary' workers.
Additional Steps Businesses Can Take When Flu Conditions are More Severe
• Check with employees who report to work
o At the beginning of the workday or with each new shift, ask employees if they have flu symptoms such as fever or chills and cough or sore throat during the last 24 hours. Other possible symptoms are runny nose, body aches, headache, tiredness, diarrhea, or vomiting. Workers with flu-like symptoms should be asked to go home.
o Continue to advise workers to check for any signs of illness before reporting to work each day.
o Encourage employees with underlying medical conditions (such as asthma, heart disease, or diabetes) or who are pregnant to contact their healthcare provider for advice about what to do if they become sick. If they become sick, they should seek care immediately.
o If flu conditions in your area become more severe, ask sick workers to stay at home for at least 7 days, even if their symptoms go away sooner. If they're still sick after 7 days, they should stay home at least 24 hours after symptoms have gone away.
• Social distancing to reduce the spread of the disease
3
o Consider letting employees who are at higher risk for flu complications work from home or stay home; if these options are not feasible, re-assign job duties so they have less contact with clients, customers, and other employees.
o If the outbreak is severe, employers should consider using some of these steps, if possible: cancel non-essential face-to-face meetings; cancel non-essential travel; space employees farther apart in the workplace or assign them to telework; and stagger shifts to allow fewer workers to be in the workplace at the same time.
4
Talking Points on CDC's Guidance for Businesses and Employers to Plan and Respond to the 2009-2010 Influenza Season
August 19,2009
Topline Messages
• CDC is releasing new guidance that recommends response and planning actions that non-healthcare employers can take now under current flu conditions. These actions will help promote a safer workplace environment for their employees and help maintain continuity in the workplace during the 2009-2010 flu season. The guidance also includes additional strategies to use if flu conditions become more severe.
• The new guidance provides recommendations on ways to decrease the spread of seasonal flu and 2009 BlNI flu in the workplace while making sure businesses can continue to operate as normally as possible.
• Employers should use this guidance to plan for flu now. This includes 1) developing a flexible flu response plan and related workplace policies, or reviewing and revising an existing pandemic flu plan; 2) making sure employees are involved in the development and review of the plan; and 3) testing key components of the plan.
• This guidance provides a menu of tools employers can use to fight flu, in coordination with local health officials-based on local flu conditions and based on what CDC and other public health organizations know about seasonal flu and are learning about the 2009 HINl flu virus.
• We know far more about the 2009 HINl flu virus than we did when it arrived in April. But we don't yet know what will happen with 2009 BlNI flu in the fall and winter. It could remain at levels similar to what we saw last spring and what has continued into the summer. It could go away entirely, or it could get worse.
• Given ongoing 2009 BINl flu activity this summer, in combination with circulating seasonal flu in the fall and winter, the CDC anticipates more flu cases, hospitalizations, and deaths.
• Because we can't predict how severe 2009-2010 flu season will be, given the impact of seasonal flu and 2009 HlNl flu, this guidance is designed to help employers plan for and respond to a continuation of the current flu situation and a more severe outbreak.
• There are things employers can do now to prevent the spread of flu in the workplace and keep their businesses operating as normally as possible. All people with flu-like symptoms should stay home and away from the workplace, hand washing and respiratory etiquette should be encouraged, and routine cleaning of commonly touched surfaces should be performed regularly.
• During a more severe outbreak, employers should take steps to keep people physically apart to reduce the spread of illness (called social distancing). This may include canceling business-related meetings or large gatherings, spacing workers farther apart in the workplace, canceling non-essential travel, and implementing work-from-home strategies.
• CDC and its partners will continue to monitor the spread of flu, the severity of the illness it's causing, and whether the virus is changing. We will provide updates on any changes, revise guidance as needed, and provide further advice to state and local agencies on steps to take.
• Because the 2009-2010 flu season could change rapidly, CDC recommendations may be revised quickly. Employers should make sure they have access to timely and accurate information so that they are aware of changes to the recommendations and can promptly implement any additional measures as a result.
Steps Businesses Can Take Now for Current Flu Conditions
• People who are sick or become sick with flu-like symptoms
o Advise workers to check themselves for any signs of sickness before reporting to work each day; this includes healthy employees with a family member at home with flu.
o People with flu-like symptoms should be separated from other employees and sent home promptly. They should stay home until at least 24 hours after they are free of fever (100 degrees Fahrenheit or 38 degrees Celsius) or signs of a fever (have chills, feel very warm, have a flushed appearance, or are sweating), without the use of fever-reducing medicines.
o Review sick-leave policies and consider making them flexible and consistent with public health recommendations. Make sure employees are well-aware of these policies.
o Try to provide flexible workplace and leave policies for workers who may need to stay home to care for sick family members or care for children if schools are dismissed.
o Provide information to employees overseas about what to do if they become sick.
• Hygiene/respiratory etiquette
o Employees should wash their hands often with soap and water, especially after coughing or sneezing; alcohol-based hand cleaners can be used if soap and water are not available.
o Employees should cover coughs and sneezes with a tissue; if possible,
o Employers should provide tissues and no-touch disposal receptacles for employees.
o If no tissues are available, encourage employees to cough or sneeze into their arm or sleeve.
• Routine cleaning
o Frequently clean all commonly touched surfaces in the workplace, such as workstations, countertops, and doorknobs.
o Use the cleaning agents that are usually used in these areas and follow the directions on the label. No additional disinfection beyond routine cleaning is recommended.
• Take measures to protect people at higher risk of flu complications
o Employees at higher risk of complications from flu should check with their healthcare provider for advice or if they become sick; early treatment with antiviral medicines can prevent hospitalizations and deaths. People at higher risk include pregnant women; children under 5 years of age; adults and children with chronic medical conditions (such as asthma, heart disease, or diabetes), and people 65 years of age or older.
• Vaccination
o When seasonal flu vaccine is available, consider offering it to all employees who want to reduce the risk for becoming sick with flu. If possible, offer seasonal flu vaccination opportunities at the worksite. Employees at higher risk for 2009 HINI flu complications should be encouraged to receive the 2009 HINI flu vaccine when it becomes available.
• Plan how to maintain business operations with a reduced staff
o Plan to maintain business operations if a large number of employees are home sick or are staying home to care for sick family members or children dismissed from school.
o Make contingency plans for when a lot of employees will need to stay home from work; this could include cross-training employees and hiring temporary workers.
Additional Steps Businesses Can Take When Flu Conditions are More Severe
• Check with employees who report to work
o At the beginning of the workday or with each new shift, ask employees if they have flu symptoms such as fever or chills and cough or sore throat during the last 24 hours. Other possible symptoms are runny nose, body aches, headache, tiredness, diarrhea, or vomiting. Workers with flu-like symptoms should be asked to go home.
o Continue to advise workers to check for any signs of illness before reporting to work each day.
o Encourage employees with underlying medical conditions (such as asthma, heart disease, or diabetes) or who are pregnant to contact their healthcare provider for advice about what to do if they become sick. If they become sick, they should seek care immediately.
o If flu conditions in your area become more severe, ask sick workers to stay at home for at least 7 days, even if their symptoms go away sooner. If they're still sick after 7 days, they should stay home at least 24 hours after symptoms have gone away.
• Social distancing to reduce the spread of the disease
o Consider letting employees who are at higher risk for flu complications work from home or stay home; if these options are not feasible, re-assign job duties so they have less contact with client'>, customers, and other employees.
o If the outbreak is severe, employers should consider using some of these steps, if possible: cancel non-essential face-to-face meetings; cancel non-essential travel; space employees farther apart in the workplace or assign them to telework; and stagger shifts to allow fewer workers to be in the workplace at the same time.
Norris, Katherine S. (Taffy) (CDC/OCOO/OD)
From:
Pippin, Roger L. (CDC/CCHIS/NCHM) (CTR) on behalf of CDC IMS JIC Public Health Workforce
Friday, September 04,200912:12 PM
Basket, Michelle (CDC/OSELS/NCHM); Harrison, James R. (CDC/CCID/NCIRD); Hill, Antonette Y. (CDC/OID/OD); Janssen, Alan (CDC/OSELS/NCHM); 'Kim, Phyllis'; Lennon, Tanya (CDC/OID/NCIRD); McCauley, Mary (CDC/OSELS}NCHM); Smith, Jean Clare (CDC/OID/NCIRD); 'Talbot, Melissa'; 'Bob Davis'; Buschick, Jennifer (HHS/OPHS); CDC IMS Chief Of Staff; Cohen, Mitchell L. (CDC/OID/OD); 'Ellen Kasari'; EOC Report (CDC); Fauci, Anthony (NIH/NIAID) [E]; Gomez, Thomas M. (CDC/OID/NCZVED); 'Griffin, Lyndsay'; Hall, Bill (HHS}ASPA); 'Heath, Stan'; Helfand, Rita (CDC/OID/NCPDCID); Kane, Eileen (HHS}ASPR[OPSP); 'Korslund, John'; Krull, Andrea (HHS/OPHS); 'Lautner, Elizabeth'; Marshall, Stephanie (HHS); Mayfield, Evan D. (CDC/OCOO/OD); Michael, Gretchen (HHS/ASPR/OPSP); 'Migliaccio, Kate'; Moreno, Julie (HHS/OS); 'national JIC'; 'Patricia Foley'; Pickering, Larry (CDC/OID/NCIRD); Smith, Amanda (HHS/ASPR/OPSP); Sosin, Dan (CDC/OPHPR/OD); 'Wood, Chad'; Zaza, Stephanie (CDC/OPHPR/OD); 'ASTHO info center'; Bhatt, Achal (CDC/OID/NCIRD); 'Buchanan, Anna'; Burns, Erin (CDC/OID/NCIRD); CDC IMS State Health Department Branch Director(CDC); Evans, Victoria (CDC/OID}NCIRD); Lemmings, Jennifer (CDC cste.org); Kan, Lilly (CDC naccho.org); Kilgus, Duane (CDC/OID/NCIRD); McConnon, Patrick (CDC cste.org); 'Paul Etkind'; PSC Jennifer Joseph; 'Richard Hughes'; Robinson, LaKesha (CDC cste.org); Fasano, Nancy (CDC/OID/NCIRD); Harton, Elizabeth (CDC/OID/NCPDCID); NCIRD Immunization Grantee Mailbox (CDC); Pope, Kristin (CDC/OID/NCIRD); Rodewald, Lance (CDC[OID/NCIRD); Whitehead, Cynthia (CDC/OID/NCIRD); Blythe, David (Maryland) (CDC dhmh.state.md.us); 'David Carney'; 'David Paulson'; 'Frances Phillips'; 'Heather Hauck'; 'John Healy'; 'Karen Black'; 'Lauren Mendes'; 'Lucy Wilson'; 'Mimi Morgan'; 'Rene Milligan'; 'Sean Smith'; 'Yasamine Richardson'
Updated CDC key points for Sept 4,2009
Sent:
To:
Subject:
Good Afternoon Partners. Below you will find both the CDC FluView and Updated Key paints for this week. Enjoy your holiday weekend.
F0934 CDC FluView Updated Key Points
Aug 29 2009.... Sept 4 2009 ...
What's New and Updated Today Sept.4, 2009
• Each week CDC analyzes information about influenza disease activity in the United States and publishes findings of key flu indicators in a report called FluView.
• During the week of August 23-29, 2009, a review of these key indictors found that influenza activity increased in the United States.
• Current visits to doctors for influenza-like illness are down from April, but are higher than what is expected in the summer. Visits to doctors for influenza-like illness (Il.I) were highest in February during the 2008-09 flu season, but rose again in April 2009 after the new 2009 H1Nl virus emerged ..
• Total influenza hospitalization rates for adults and children are similar to or lower than seasonal influenza hospitalization rates depending on age group.
• The proportion of deaths attributed to pneumonia and influenza (P&I) was low and within the bounds of what is expected in the summer.
• Six states (Alabama, Alaska, Florida, Georgia, Mississippi, and South Carolina) and PUerto Rico are reporting widespread influenza activity at this time.
• Any reports of widespread influenza activity in August are very unusual.
• Almost all of the influenza viruses identified were the new 2009 H iN 1 influenza A viruses.
• These 2009 H1Nl viruses remain similar to the viruses chosen for the 2009 HiNl vaccine, and remain susceptible to antiviral drugs (oseltamivir and zanamivir) with rare exception.
• CDC continues to report 2009 H1Nl hospitalizations and deaths.
• As of September 4, 2009, 9,079 total 2009 H1Nl influenza hospitalizations, and 593 total deaths have been reported to CDC by state and local public health departments since midApril.
• During Week 34 (the week ending August 29, 2009), one influenza-associated pediatric death was reported to CDC.
• This death occurred in New York and was associated with 2009 H1Nl virus infection.
• This death occurred between June 14 and June 20, 2009.
• Since September 28, 2008, CDC has received 111 reports of laboratory confirmed. influenza-associated pediatric deaths that occurred during the 2008-09 influenza season, 43 of which were due to 2009 HiNl influenza virus infections.
• CDC anticipates that 2009 H 1N 1 influenza viruses will co-circulate with regular seasonal influenza viruses over our influenza season.
• The timing, spread and severity of 2009 H1Nl virus - in addition to our regular seasonal influenza viruses - are uncertain.
I
2
·lnfh.lenza
2008~2009 Influenza Season Week 34 ending August 29, 2009
All data are preliminary and may change as more reports are received.
Synopsis: During week 34 (August 23-29, 2009), influenza activity increased in the United States.
o Since mid-April to August 30, 2009, a total of 9,079 hospitalizations and 593 deaths associated with 2009 influenza A (H1 N1) viruses have been reported to CDC an increase from 8,843 hospitalizations and 556 deaths from the prior week.
o During week 34:
o 1,109 (17.3%) specimens tested by U.S. World Health Organization (WHO) and National Respiratory and Enteric Virus Surveillance System (NREVSS) collaborating laboratories and reported to CDC/Influenza Division were positive for influenza.
o 97% of all subtyped influenza A viruses being reported to CDC were 2009 influenza A (H1 N1) viruses.
o One human infection with a novel influenza A virus was reported.
o The proportion of deaths attributed to pneumonia and influenza (P&I) was below the epidemic threshold.
o One influenza-associated pediatric death was reported and was associated with a 2009 influenza A (H1 N1) virus infection.
o The proportion of outpatient visits for influenza-like illness (Ill) was below the national baseline, Region IV reported III above its region-specific baseline.
o Six states and Puerto Rico reported geographicaUy widespread influenza activity, 13 states reported regional influenza activity, 10 states and the District of Columbia reported local influenza activity, 19 states reported sporadic influenza activity, two states reported no influenza activity, and Guam and the U.S. Virgin Islands did not report,
ationa and Regional Summary of Select Surveillance omponents
Data for current week Data cumulative for the season
Number of A
HHS Out- % jurisdictions A (Subty-
Surveillance patient positive reporting A (Hi) A 2009 A (unable ping B Pediatric
Regions* fLIt fer flu:!: regional or (H3) (H1 N1) to sub- not Deaths
widespread type)¥ perter-
activity§ med)
Nation Normal 17.3% 20 of 54 8,211 4,026 38,112 830 19,997 10,821 111
Region I Normal 8.3% o of6 585 305 2,933 13 1,706 820 4
Region II Normal 2.9% 2 of 4 297 228 1,831 21 2,391 714 20
Region III Normal 15.7% 2of6 1,251 220 4,378 20 1,045 1,363 10
Region IV Elevated 19,9% 8of8 910 444 4,850 84 3,530 1,298 10
Region V Normal 12.0% o of6 1,661 212 8,365 199 884 1,422 18
Region VI Normal 24.6% 2 of 5 830 309 3,698 7 5,013 2,667 16
Region VII Normal 15.4% 1of4 537 86 1,149 118 553 537 0
Region VIII Normal 13.8% 1of6 540 219 1,569 80 1,784 503 9
Region IX Normal 24.3% 3 of 5 1,210 1,679 6,681 74 2,559 806 . 21
Region X Normal 20.6% 1of4 390 324 2,658 214 532 691 3
. N
c
HHS regions (Region I. CT. ME, MA, NH. RI, VT, Region II. NJ, NY, Puerto RIco. US Virgin Islands: Region II!: DE, DC, MD, PA, VA, WV, Region IV. AL, FL, GA, KY, MS, NC • SC, TN; Region V: Il, IN, MI. MN, OH, W; Region VI: AR, LA, NM, OK, TX; Region VII: IA. KS, MO, NE; Region VIII: CO, MT, ND, SD, UT, WY; Region IX: Al, CA, Guam, HI, NV; and Region X: AK, ID, OR, WA)
t Elevated means the % of visits for III is at or above the national or region-specific baseline :j: National data are for current week; regional data are for the most recent three weeks
§ Includes all 50 states, the District of Columbia, Guam, Puerto Rico. and U.S. Virgin Islands
¥ The majority of influenza A viruses that cannot be suo-typed as seasonal infiuen~a viruses are 2009 A (Hi Nil influenza viruses upon further testing
U.S. Virologic Surveillance: WHO and NREVSS collaborating laboratories located in all 50 states and Washington D.C. report to CDC the number of respiratory specimens tested for influenza and the number positive by influenza type and subtype. The results of tests performed during the current week are summarized in the table below.
Week 34
No. of specimens tested 6A10
No. of positive specimens (%) 1,109 (17,3%)
Positive specimens by type/subtype
Influenza A 1,105 (99.6%)
A (2009 H1 N1) 756 (68.3%)
A (subtyping not performed) 311 (28,1%)
A (unable to subtype) 18 (1.6%)
A (H3) 11(1.0%)
A (H1) 10 (0,9%)
Influenza B 4 (0.4%) During week 34, seasonal influenza A (Hi) and A (H3) and B viruses co-circulated at low levels with 2009 influenza A (H1N1) viruses. 97% of all subtyped influenza A viruses being reported to CDC this week were 2009 influenza A (Hi N1) viruses.
The unusually high percentage of specimens testing positive for influenza by WHO and NREVSS collaborating laboratories remained higher during week 34 than is typically seen this time of year, and may be due to a combination of factors including higher than normal circulation of influenza in the summer with the emergence of the 2009 Hi N1 virus, changes in testing practices by health care providers, triaging of specimens by public health laboratories, an increase in the number of specimens collected from outbreaks, and other factors.
As of September 4,2009,9,079 hospitalizations and 593 deaths (16 deaths in individuals 0-4 years, 93 deaths in individuals 5-24 years, 249 deaths in' adults 25-49 years, 171 deaths in adults 50-64 years,57 deaths in adults age 65 and older, and 7 deaths for which age was no reported) associated with 2009 infl uenza A (H 1 N 1) virus have been identified by CDC and state and local public health departments (http://www.cdc.gov/hin1flu/update.htm).
2008-2009 Influenza Season - Week 34, ending August 29.2009
2
Você também pode gostar
- 2017-01-06 Final ResponseDocumento2 páginas2017-01-06 Final ResponseCREWAinda não há avaliações
- 2016 12 30 Responsive DocumentsDocumento15 páginas2016 12 30 Responsive DocumentsCREWAinda não há avaliações
- 2017-01-06 Documents Produced 1Documento365 páginas2017-01-06 Documents Produced 1CREWAinda não há avaliações
- 2016 12 28 Final ResponseDocumento2 páginas2016 12 28 Final ResponseCREWAinda não há avaliações
- 2017-01-06 Documents Produced 2Documento36 páginas2017-01-06 Documents Produced 2CREWAinda não há avaliações
- Via Electronic Mail OnlyDocumento2 páginasVia Electronic Mail OnlyCREWAinda não há avaliações
- New York Office of The Attorney General (Trump Foundation Investigation) Request 9-14-16Documento2 páginasNew York Office of The Attorney General (Trump Foundation Investigation) Request 9-14-16CREWAinda não há avaliações
- 2016 12 16 FOIA RequestDocumento3 páginas2016 12 16 FOIA RequestCREWAinda não há avaliações
- 2016-12-21 FOIA Request (Documents To Congress)Documento3 páginas2016-12-21 FOIA Request (Documents To Congress)CREWAinda não há avaliações
- 2016 12 16 FOIA RequestDocumento3 páginas2016 12 16 FOIA RequestCREWAinda não há avaliações
- 2016 12 16 FOIA RequestDocumento3 páginas2016 12 16 FOIA RequestCREWAinda não há avaliações
- Plaintiffs' Memorandum in Support of Motion For Temporary InjunctionDocumento6 páginasPlaintiffs' Memorandum in Support of Motion For Temporary InjunctionCREWAinda não há avaliações
- 2016-12-21 FOIA Request (Communications With Trump and Congress)Documento3 páginas2016-12-21 FOIA Request (Communications With Trump and Congress)CREWAinda não há avaliações
- Florida Office of The Attorney General (Daily Schedules and Travel) Request 9-14-16Documento5 páginasFlorida Office of The Attorney General (Daily Schedules and Travel) Request 9-14-16CREWAinda não há avaliações
- FBI Denial 11-29-2016Documento1 páginaFBI Denial 11-29-2016CREWAinda não há avaliações
- FOIA Request - OGE (Trump Transition) 12-7-16Documento3 páginasFOIA Request - OGE (Trump Transition) 12-7-16CREWAinda não há avaliações
- FBN Materials 422.15Documento64 páginasFBN Materials 422.15CREWAinda não há avaliações
- FBI Denial 12-1-2016Documento2 páginasFBI Denial 12-1-2016CREWAinda não há avaliações
- Final Response Letter 10-17-2016Documento2 páginasFinal Response Letter 10-17-2016CREWAinda não há avaliações
- Final Installment 10-17-2016Documento47 páginasFinal Installment 10-17-2016CREWAinda não há avaliações
- FBI (Congress Communications Re Comey Letter) 11-22-16Documento3 páginasFBI (Congress Communications Re Comey Letter) 11-22-16CREWAinda não há avaliações
- FBI (Kallstrom Communications) 11-22-16Documento3 páginasFBI (Kallstrom Communications) 11-22-16CREWAinda não há avaliações
- FBI (Giuliani Communications) 11-22-16Documento3 páginasFBI (Giuliani Communications) 11-22-16CREWAinda não há avaliações
- FOIA Request - OGE (Trump Tweets) 12-6-16Documento3 páginasFOIA Request - OGE (Trump Tweets) 12-6-16CREWAinda não há avaliações
- FBI Denial 12-1-2016Documento2 páginasFBI Denial 12-1-2016CREWAinda não há avaliações
- Memorandum in Opposition To Plaintiffs' Motion For Temporary Injunction and Declaration of Amy Frederick With ExhibitsDocumento19 páginasMemorandum in Opposition To Plaintiffs' Motion For Temporary Injunction and Declaration of Amy Frederick With ExhibitsCREWAinda não há avaliações
- Plaintiffs' Reply in Support of Motion For Preliminary InjunctionDocumento2 páginasPlaintiffs' Reply in Support of Motion For Preliminary InjunctionCREWAinda não há avaliações
- Second Declaration of James L. MartinDocumento9 páginasSecond Declaration of James L. MartinCREWAinda não há avaliações
- Amended Complaint For Declaratory Judgment, Temporary, and Permanent InjunctionDocumento22 páginasAmended Complaint For Declaratory Judgment, Temporary, and Permanent InjunctionCREWAinda não há avaliações
- Complaint For Declaratory Judgment, Temporary and Permanent InjunctionDocumento8 páginasComplaint For Declaratory Judgment, Temporary and Permanent InjunctionCREWAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)