Você também pode gostar
- The Biology of HomosexualityDocumento201 páginasThe Biology of HomosexualityIsis Bugia100% (1)
- An Overview of Chinas Fruit and Vegetables IndustryDocumento50 páginasAn Overview of Chinas Fruit and Vegetables IndustryAnonymous 45z6m4eE7pAinda não há avaliações
- Fertigation of TurmericDocumento37 páginasFertigation of TurmerictellashokAinda não há avaliações
- Vector-Borne Disease Management ProgrammesDocumento44 páginasVector-Borne Disease Management ProgrammesInternational Association of Oil and Gas Producers100% (1)
- Fundamentals of Agricultural Engineering PDFDocumento2 páginasFundamentals of Agricultural Engineering PDFpohza83% (6)
- Introduction To Agriculture: Esther S.lancitaDocumento25 páginasIntroduction To Agriculture: Esther S.lancitaEsther Suan-Lancita100% (1)
- International Code of Conduct on Pesticide Management: Guidelines on Good Labelling Practice for Pesticides (Revised) August 2015No EverandInternational Code of Conduct on Pesticide Management: Guidelines on Good Labelling Practice for Pesticides (Revised) August 2015Ainda não há avaliações
- Multiple Choice - Exam - Irrigation - 09 - 10Documento9 páginasMultiple Choice - Exam - Irrigation - 09 - 10Gemechu100% (1)
- Zuidberg Frontline Systems BV - Pricelist Valid From 01-01-2012Documento143 páginasZuidberg Frontline Systems BV - Pricelist Valid From 01-01-2012emmanolanAinda não há avaliações
- A Micropropagation System For Cloning of Hemp (Cannabis Sativa L.) by Shoot Tip CultureDocumento6 páginasA Micropropagation System For Cloning of Hemp (Cannabis Sativa L.) by Shoot Tip CultureFco Javier Navarta PiquetAinda não há avaliações
- Guidelines for Personal Protection When Handling and Applying Pesticides: International Code of Conduct on Pesticide ManagementNo EverandGuidelines for Personal Protection When Handling and Applying Pesticides: International Code of Conduct on Pesticide ManagementAinda não há avaliações
- Biodiesel From Micro AlgaeDocumento3 páginasBiodiesel From Micro Algaeraanja2Ainda não há avaliações
- He PhaseDocumento1 páginaHe PhasenimrguwahatiAinda não há avaliações
- Study of DDT (G6) PDFDocumento15 páginasStudy of DDT (G6) PDFNajihah JaffarAinda não há avaliações
- DDTDocumento2 páginasDDTManoloAinda não há avaliações
- Global Surveillance of DDT and Dde Levels in Human Tissues: Kushik Jaga and Chandrabhan DharmaniDocumento14 páginasGlobal Surveillance of DDT and Dde Levels in Human Tissues: Kushik Jaga and Chandrabhan DharmaniInstituto Pablo JamilkAinda não há avaliações
- Jurnal 4Documento6 páginasJurnal 4Asniar RAinda não há avaliações
- Dichlorodiphenyltrichloroethane (DDT) For IndoorDocumento15 páginasDichlorodiphenyltrichloroethane (DDT) For Indoorlilibeth paola duran plataAinda não há avaliações
- Al Amin 2020 PV 13 622Documento15 páginasAl Amin 2020 PV 13 622poonamAinda não há avaliações
- Do You Now Think That DDT Should Have Been Banned or Should Still Be UsedDocumento3 páginasDo You Now Think That DDT Should Have Been Banned or Should Still Be UsedJuan Manuel Herrera NavasAinda não há avaliações
- Journal of Global Antimicrobial ResistanceDocumento9 páginasJournal of Global Antimicrobial ResistancerehanaAinda não há avaliações
- Covid 19 Strategy UpdateDocumento19 páginasCovid 19 Strategy UpdateintellectualpseudoAinda não há avaliações
- Pesticide Residues in FoodsDocumento9 páginasPesticide Residues in FoodsderrickAinda não há avaliações
- 51523-Article Text-161459-1-10-20210120Documento2 páginas51523-Article Text-161459-1-10-20210120Azhar HussainAinda não há avaliações
- Ethical Dilemma Applied in Pesticide DDTDocumento9 páginasEthical Dilemma Applied in Pesticide DDTichablubsAinda não há avaliações
- 0902 Reversion Fo ResistranceDocumento3 páginas0902 Reversion Fo ResistranceVibhaMalikAinda não há avaliações
- DDT Case StudyDocumento9 páginasDDT Case Studymaheswari.kumar2784Ainda não há avaliações
- Science of The Total EnvironmentDocumento20 páginasScience of The Total EnvironmentharshAinda não há avaliações
- Policy Guidance On Drug-Susceptibility Testing (DST) of Second-Line Antituberculosis DrugsDocumento20 páginasPolicy Guidance On Drug-Susceptibility Testing (DST) of Second-Line Antituberculosis DrugsrehanaAinda não há avaliações
- Public Health in Outbreak of Covid and ManagementDocumento16 páginasPublic Health in Outbreak of Covid and ManagementMuhammad JavedAinda não há avaliações
- Vector 001 To 004Documento4 páginasVector 001 To 004Jin SiclonAinda não há avaliações
- WHO HCWM Policy Paper 2004Documento2 páginasWHO HCWM Policy Paper 2004Heri PermanaAinda não há avaliações
- FDA Guidance DILs and PAGs For Food ContaminationDocumento59 páginasFDA Guidance DILs and PAGs For Food ContaminationDorje PhagmoAinda não há avaliações
- DdtpersuasiveessayDocumento3 páginasDdtpersuasiveessayapi-269169613Ainda não há avaliações
- Implementation and Challenge in Dealing With The BMW Disposal Guidelines and LegislationsDocumento14 páginasImplementation and Challenge in Dealing With The BMW Disposal Guidelines and LegislationsIJAR JOURNALAinda não há avaliações
- Tugas Jurnal 2Documento12 páginasTugas Jurnal 2RahmaAinda não há avaliações
- International Code of Conduct Om Pesticides 2013Documento32 páginasInternational Code of Conduct Om Pesticides 2013Naku MosesAinda não há avaliações
- Effectiveness of The Most Commonly Used Mosquitoes Repellent in Households in Niameycity (Niger)Documento10 páginasEffectiveness of The Most Commonly Used Mosquitoes Repellent in Households in Niameycity (Niger)IJAR JOURNALAinda não há avaliações
- Preprints202307 1828 v1Documento16 páginasPreprints202307 1828 v1Shandana QasimAinda não há avaliações
- Laboratory Biorisk ManagementDocumento18 páginasLaboratory Biorisk ManagementAni IoanaAinda não há avaliações
- Implications of The COVID-19 Pandemic On Eliminating Trachoma As A Public Health ProblemDocumento17 páginasImplications of The COVID-19 Pandemic On Eliminating Trachoma As A Public Health ProblemZahra Kesturi RifandariAinda não há avaliações
- TDR Ide Den 03.1Documento40 páginasTDR Ide Den 03.1fabio.fagundes6986Ainda não há avaliações
- Guide Handling Cytoxic Drugs Related Waste PDFDocumento89 páginasGuide Handling Cytoxic Drugs Related Waste PDFDewi Ratna SariAinda não há avaliações
- Bourguet & Guillemaud Sustainable Agriculture Review 2016-1Documento87 páginasBourguet & Guillemaud Sustainable Agriculture Review 2016-1azhariAinda não há avaliações
- Gens 102 Assignment 2Documento4 páginasGens 102 Assignment 2mirabelle LovethAinda não há avaliações
- Traditional Medicines: An Alternative Preferencial Remedy For Covid-19 ControlDocumento15 páginasTraditional Medicines: An Alternative Preferencial Remedy For Covid-19 ControlMOULIANNA8949Ainda não há avaliações
- Articulo 3Documento9 páginasArticulo 3nataliameloAinda não há avaliações
- ARMSTRONG JW Fruit Fly Disinfestation Strategies Beyond Methyl BromideDocumento14 páginasARMSTRONG JW Fruit Fly Disinfestation Strategies Beyond Methyl BromideDwik RachmantoAinda não há avaliações
- Neglected Tropical Diseases - Progress Towards Addressing The Chronic PandemicDocumento14 páginasNeglected Tropical Diseases - Progress Towards Addressing The Chronic PandemicVivi AlvarezAinda não há avaliações
- Hygiene Response COVID19 V4Documento70 páginasHygiene Response COVID19 V4Mustafa AdelAinda não há avaliações
- JurnalDocumento4 páginasJurnalAnonymous pfHZusnAinda não há avaliações
- Guidelines For PMDT in India - Dec 11 (Final)Documento199 páginasGuidelines For PMDT in India - Dec 11 (Final)manishwceAinda não há avaliações
- Review: David H Molyneux, Lorenzo Savioli, Dirk EngelsDocumento15 páginasReview: David H Molyneux, Lorenzo Savioli, Dirk EngelsYosia KevinAinda não há avaliações
- TELEDERDocumento7 páginasTELEDERSajin AlexanderAinda não há avaliações
- International Journal of Infectious DiseasesDocumento4 páginasInternational Journal of Infectious DiseasesPedro MalikAinda não há avaliações
- Indoor Residual Spray - 5Documento12 páginasIndoor Residual Spray - 5srinivasthAinda não há avaliações
- An Ethical Risk Management Approach For MedicalDocumento9 páginasAn Ethical Risk Management Approach For Medicalpievee27102004Ainda não há avaliações
- Tele 2Documento10 páginasTele 2Sajin AlexanderAinda não há avaliações
- Current Research in Pharmacology and Drug DiscoveryDocumento10 páginasCurrent Research in Pharmacology and Drug Discoverydev darma karinggaAinda não há avaliações
- DTT&MalariaDocumento3 páginasDTT&MalariaAKARSH RAOAinda não há avaliações
- Who Guidelines TB Ro 2019 PDFDocumento104 páginasWho Guidelines TB Ro 2019 PDFrima melliaAinda não há avaliações
- DDTDocumento5 páginasDDThuyarchitect89Ainda não há avaliações
- Covid Strategy Update 13april2020Documento18 páginasCovid Strategy Update 13april2020garuda unriAinda não há avaliações
- From Concept To Action: A United, Holistic and One Health Approach To Respond To The Climate Change CrisisDocumento7 páginasFrom Concept To Action: A United, Holistic and One Health Approach To Respond To The Climate Change CrisisAndrew FincoAinda não há avaliações
- Abdullahi Muhammad Musa PCC AssignmentDocumento2 páginasAbdullahi Muhammad Musa PCC AssignmentAbdullahi Muhammad MusaAinda não há avaliações
- Covid-19 Prevention StrategiesDocumento6 páginasCovid-19 Prevention StrategiesJackson PaulAinda não há avaliações
- Human Health: and PesticidesDocumento26 páginasHuman Health: and PesticidesLaney SommerAinda não há avaliações
- Agreement of Sanitary and Phytosanitary MeasuresDocumento10 páginasAgreement of Sanitary and Phytosanitary MeasuresShazaf KhanAinda não há avaliações
- 2021 New Trend in The Extraction of Pesticides Applying MicroextractionDocumento28 páginas2021 New Trend in The Extraction of Pesticides Applying MicroextractionSITI NUR AFIQAH MAHAZANAinda não há avaliações
- WHO Dengue Guidelines 2013Documento160 páginasWHO Dengue Guidelines 2013Jason MirasolAinda não há avaliações
- How To Wrtie The Perfect Data Analysis EvaluationDocumento1 páginaHow To Wrtie The Perfect Data Analysis EvaluationIsis BugiaAinda não há avaliações
- Melton Transforming Cookbook LabsDocumento11 páginasMelton Transforming Cookbook LabsIsis BugiaAinda não há avaliações
- Structure Based Drug Design - Muya PDFDocumento831 páginasStructure Based Drug Design - Muya PDFIsis BugiaAinda não há avaliações
- Brooker CH 6 SampleDocumento20 páginasBrooker CH 6 SampleIsis BugiaAinda não há avaliações
- Vector Control Saving LivesDocumento13 páginasVector Control Saving LivesIsis BugiaAinda não há avaliações
- ProteinFolding Dynamics - PDFDocumento29 páginasProteinFolding Dynamics - PDFIsis BugiaAinda não há avaliações
- Manual-5 0Documento312 páginasManual-5 0Isis BugiaAinda não há avaliações
- Practica-III-2 - Um Curso Laboratorial em Química Medicinal Introduzindo A Modelagem MolecularDocumento24 páginasPractica-III-2 - Um Curso Laboratorial em Química Medicinal Introduzindo A Modelagem MolecularIsis BugiaAinda não há avaliações
- Tutorial - Molecular Simulation Methods With GromacsDocumento12 páginasTutorial - Molecular Simulation Methods With GromacsIsis BugiaAinda não há avaliações
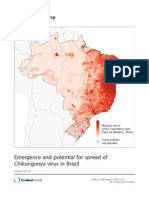
- Emergence and Potential For Spread of Chikungunya Virus in Brazil - FinishedDocumento11 páginasEmergence and Potential For Spread of Chikungunya Virus in Brazil - FinishedIsis BugiaAinda não há avaliações
- (Dufour, Castets,..) Lu. LongipalpisDocumento7 páginas(Dufour, Castets,..) Lu. LongipalpisIsis BugiaAinda não há avaliações
- Visceral Leishmaniasis TreatmentDocumento9 páginasVisceral Leishmaniasis TreatmentIsis BugiaAinda não há avaliações
- FT Baked Beans Tomate Heinz 420gDocumento3 páginasFT Baked Beans Tomate Heinz 420gNuno LeãoAinda não há avaliações
- Of Tribes, Hunters and Barbarians - Forest Dwellers in The Mauryan PeriodDocumento20 páginasOf Tribes, Hunters and Barbarians - Forest Dwellers in The Mauryan PeriodZaheen AkhtarAinda não há avaliações
- FAO Fisheries & Aquaculture - Fishery and Aquaculture Country Profiles - The Republic of GhanaDocumento15 páginasFAO Fisheries & Aquaculture - Fishery and Aquaculture Country Profiles - The Republic of Ghana최두영Ainda não há avaliações
- Kankana Ey SummaryDocumento1 páginaKankana Ey Summarychristian ifurungAinda não há avaliações
- Agricultural Sector in PakistanDocumento4 páginasAgricultural Sector in PakistanimranramdaniAinda não há avaliações
- Classic Cocktails Via ClementDocumento2 páginasClassic Cocktails Via ClementJason McCoolAinda não há avaliações
- Honeybee ProposalDocumento3 páginasHoneybee Proposalapi-284387524Ainda não há avaliações
- ClaydenDocumento52 páginasClaydenapi-194319130Ainda não há avaliações
- The Opportunities of Investing in Costa Rica Farm For Sale1Documento25 páginasThe Opportunities of Investing in Costa Rica Farm For Sale1pinki mollick-17 204 LaptopAinda não há avaliações
- Geo Chapter 4 Class 8 Extra QuestionDocumento6 páginasGeo Chapter 4 Class 8 Extra QuestionJivitesh MangalAinda não há avaliações
- BCS Brochure 2016Documento40 páginasBCS Brochure 2016TractorDiésel100% (1)
- Rural EconomicsDocumento8 páginasRural EconomicssaravananAinda não há avaliações
- History of NasugbuDocumento4 páginasHistory of NasugbuChristian Rey Sandoval DelgadoAinda não há avaliações
- The Imperial Vs The Metric SystemDocumento15 páginasThe Imperial Vs The Metric Systemapi-250910942Ainda não há avaliações
- tmp3397 TMPDocumento7 páginastmp3397 TMPFrontiersAinda não há avaliações
- Final ProposalDocumento29 páginasFinal Proposalgusto koAinda não há avaliações
- Morphology and Life Cycle of Puccinia and The Symptoms of SmutsDocumento21 páginasMorphology and Life Cycle of Puccinia and The Symptoms of SmutsRuchika PokhriyalAinda não há avaliações
- Jess 104Documento14 páginasJess 104ScoutAinda não há avaliações
- Estimating Soil Losses Using Universal Soil Loss Equation (USLE)Documento31 páginasEstimating Soil Losses Using Universal Soil Loss Equation (USLE)Walter F SilvaAinda não há avaliações
- Rice Sector ReportDocumento2 páginasRice Sector ReportHakam DaderAinda não há avaliações
- Chemicals JogiDocumento12 páginasChemicals JoginormanwillowAinda não há avaliações