Você também pode gostar
- Leishmaniasis 2Documento3 páginasLeishmaniasis 2b29jcqnfn9Ainda não há avaliações
- Infection in CancerDocumento34 páginasInfection in CancerSheikAinda não há avaliações
- WO No.10 Week 2Documento4 páginasWO No.10 Week 2ReginaJacobAinda não há avaliações
- Necrotizing FasciitisDocumento45 páginasNecrotizing FasciitisKuchai BaruAinda não há avaliações
- Ulcerated Lesions 5555555Documento11 páginasUlcerated Lesions 5555555ربيد احمد مثنى يحيى كلية طب الاسنان - جامعة عدنAinda não há avaliações
- Skin and Soft Tissue Infection InfoDocumento4 páginasSkin and Soft Tissue Infection InfoPresura Andreea IulianaAinda não há avaliações
- Artikan 3Documento1 páginaArtikan 3Rivan San JayaAinda não há avaliações
- Clostridia Gram Positive Bacilli InfectionsDocumento5 páginasClostridia Gram Positive Bacilli InfectionsUloko ChristopherAinda não há avaliações
- Bullous Pemphigoid and Pemphigus GuideDocumento22 páginasBullous Pemphigoid and Pemphigus GuideDanielAinda não há avaliações
- 00chloramphenicol: - People Who Survive May Suffer From Leukemia Later Life. An Excess DoseDocumento5 páginas00chloramphenicol: - People Who Survive May Suffer From Leukemia Later Life. An Excess DosealbeezieAinda não há avaliações
- Acute Infections Oral and Paraoral TissuesDocumento33 páginasAcute Infections Oral and Paraoral TissuesKarthik S'twinkles SAinda não há avaliações
- CC 48 AntifungalDocumento5 páginasCC 48 AntifungalFRANCES CHYLA QUELITANOAinda não há avaliações
- DR. GUPTA'S LECTURE ON FUNGAL INFECTIONSDocumento49 páginasDR. GUPTA'S LECTURE ON FUNGAL INFECTIONSAMIT GUPTAAinda não há avaliações
- Severe Necrotising Soft Tissue Infections: Other SstisDocumento4 páginasSevere Necrotising Soft Tissue Infections: Other SstisAkriti GuptaAinda não há avaliações
- Odessa National Medical University: Surgical InfectionsDocumento34 páginasOdessa National Medical University: Surgical InfectionsDrRajneesh ShastriAinda não há avaliações
- Sexually Transmmited Diseases: Presenter: Nyangara Rajabu Facilitator: Isaac U. MDocumento31 páginasSexually Transmmited Diseases: Presenter: Nyangara Rajabu Facilitator: Isaac U. MnyangaraAinda não há avaliações
- PneumoniaDocumento10 páginasPneumoniaAubrey PerezAinda não há avaliações
- Antimicrobial Drugs: Pharmacology Unit 2Documento20 páginasAntimicrobial Drugs: Pharmacology Unit 2Saima VictorAinda não há avaliações
- Damage To Cell MembraneDocumento7 páginasDamage To Cell MembraneEsteph CortesAinda não há avaliações
- Antibiotics in Oral and Maxillofacial SurgeryDocumento25 páginasAntibiotics in Oral and Maxillofacial Surgeryindian dental academyAinda não há avaliações
- Leishmaniasis: Dr. Kazi Shihab Uddin Mbbs MRCP (Uk) Associate Professor & HOD Department of Internal MedicineDocumento20 páginasLeishmaniasis: Dr. Kazi Shihab Uddin Mbbs MRCP (Uk) Associate Professor & HOD Department of Internal MedicineSHIHAB UDDIN KAZIAinda não há avaliações
- Mycobacterium General Properties: Mycobacteria Cell Wall StructureDocumento12 páginasMycobacterium General Properties: Mycobacteria Cell Wall StructureAhmed ExaminationAinda não há avaliações
- U1 P9 Antimicrobial Resistance Mechanism, What Is Wound HealingDocumento21 páginasU1 P9 Antimicrobial Resistance Mechanism, What Is Wound HealingSab almnalAinda não há avaliações
- Pseudomonas Aeruginosa InfectionsDocumento22 páginasPseudomonas Aeruginosa InfectionsMiguel RomeroAinda não há avaliações
- Management of Septic ShockDocumento33 páginasManagement of Septic ShockswatisinghnigeriaAinda não há avaliações
- Infection & Specific Wound InfectionsDocumento39 páginasInfection & Specific Wound InfectionsAhmed ShorshAinda não há avaliações
- December 2013 What Is Necrotizing Fasciitis? What Are Its Causes? How Will You Manage Such A Case?Documento3 páginasDecember 2013 What Is Necrotizing Fasciitis? What Are Its Causes? How Will You Manage Such A Case?Vaibhav BharatAinda não há avaliações
- F01ddiabrtes and InfectionDocumento82 páginasF01ddiabrtes and InfectionAbdel-razek ElmelegiAinda não há avaliações
- Antibiotics Part II. Antimycobacteria Agents.Documento69 páginasAntibiotics Part II. Antimycobacteria Agents.inaAinda não há avaliações
- Micro Chapter 17Documento8 páginasMicro Chapter 17Ana AbuladzeAinda não há avaliações
- Diagnosing and Treating Necrotizing FasciitisDocumento1 páginaDiagnosing and Treating Necrotizing FasciitisAditya Riadi SyafeiAinda não há avaliações
- Septic Arthritis Characterized byDocumento55 páginasSeptic Arthritis Characterized byNdor BariboloAinda não há avaliações
- CROHNSDocumento2 páginasCROHNSAlvin Germo Pasuquin100% (1)
- Infectious Diseases NotesDocumento34 páginasInfectious Diseases NotesNuha AL-YousfiAinda não há avaliações
- Antifungal AgentsDocumento41 páginasAntifungal AgentsSami YGAinda não há avaliações
- Soft Tissue Infections English 3-Rd 2016Documento39 páginasSoft Tissue Infections English 3-Rd 2016Stefi GrAinda não há avaliações
- Case Study 1Documento27 páginasCase Study 1Athena Mae SantiagoAinda não há avaliações
- Lac 10&11 PPTDocumento16 páginasLac 10&11 PPTRaghdaAinda não há avaliações
- Meningococcemia: Neisseria Meningitidis - Is An EncapsulatedDocumento19 páginasMeningococcemia: Neisseria Meningitidis - Is An EncapsulatedcarolinecayasaAinda não há avaliações
- 4 U1.0 B978 1 4377 0755 7..00235 9..DOCPDFDocumento3 páginas4 U1.0 B978 1 4377 0755 7..00235 9..DOCPDFdisk_la_poduAinda não há avaliações
- PBL 3 CNSDocumento13 páginasPBL 3 CNSAbdullah SohailAinda não há avaliações
- Cutaneous Tuberculosis - StatPearls - NCBI BookshelfDocumento5 páginasCutaneous Tuberculosis - StatPearls - NCBI BookshelfLinuel Quetua TrinidadAinda não há avaliações
- Case ReportDocumento13 páginasCase ReportmarselamgeAinda não há avaliações
- Case-Study ParasitDocumento24 páginasCase-Study ParasitAthena Mae SantiagoAinda não há avaliações
- Rotar O.V. As - Prof. General Surgery, BSMUDocumento63 páginasRotar O.V. As - Prof. General Surgery, BSMUOleksandr RotarAinda não há avaliações
- Infections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumNo EverandInfections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumAinda não há avaliações
- Nephritic SyndromeDocumento15 páginasNephritic Syndrome76q88b4yrxAinda não há avaliações
- Agranulocytosis FinalDocumento17 páginasAgranulocytosis FinalsanthiyasandyAinda não há avaliações
- Prep 2015Documento358 páginasPrep 2015a alrabiaahAinda não há avaliações
- Role of Antibiotics in Orthopedic InfectionsDocumento31 páginasRole of Antibiotics in Orthopedic InfectionsRakesh KumarAinda não há avaliações
- SSJ TenDocumento5 páginasSSJ TenSelviana SudarmanAinda não há avaliações
- Common Bacterial Skin InfectionsDocumento6 páginasCommon Bacterial Skin InfectionsagusAinda não há avaliações
- Lee Et Al 2001 Case Report Meningococcal MeningitisDocumento3 páginasLee Et Al 2001 Case Report Meningococcal MeningitisAsmae OuissadenAinda não há avaliações
- Opportunistic MycosesDocumento31 páginasOpportunistic MycosesMaxamed Faarax XaashiAinda não há avaliações
- Acid Fast Bacteria: M. Tuberculosis, M. LepraeDocumento22 páginasAcid Fast Bacteria: M. Tuberculosis, M. LepraeelaAinda não há avaliações
- Skin InfectionsDocumento22 páginasSkin InfectionsoktafAinda não há avaliações
- Phlegmon: Signs and SymptomDocumento4 páginasPhlegmon: Signs and SymptomFadly RizkyAinda não há avaliações
- PharmaDocumento16 páginasPharmaPaula Grace MorfeAinda não há avaliações
- Antibiotic Selection in SepsisDocumento4 páginasAntibiotic Selection in SepsisIndah AmisaniAinda não há avaliações
- Pharmacology 2 QuizDocumento3 páginasPharmacology 2 QuizAhmedAinda não há avaliações
- Intensive Course September 2019-3Documento9 páginasIntensive Course September 2019-3Fadhly SharimanAinda não há avaliações
- MCQ April2013 UpdateDocumento5 páginasMCQ April2013 UpdateFadhly SharimanAinda não há avaliações
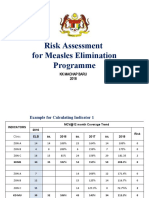
- Risk Assessment Measles 2018 KKMB - Final 3Documento17 páginasRisk Assessment Measles 2018 KKMB - Final 3Fadhly SharimanAinda não há avaliações
- Sba 1&2 Conjoint Exam Part II April 2017 Doc-1Documento21 páginasSba 1&2 Conjoint Exam Part II April 2017 Doc-1Fadhly SharimanAinda não há avaliações
- Compilation Questions of Theory Part One 04-1Documento34 páginasCompilation Questions of Theory Part One 04-1Rebecca WongAinda não há avaliações
- Histology of the Urinary System: Kidneys, Nephrons, and PassagewaysDocumento46 páginasHistology of the Urinary System: Kidneys, Nephrons, and PassagewaysAnonymous EzxZg4uQ63100% (1)
- General Principles of Antibiotic TherapyDocumento44 páginasGeneral Principles of Antibiotic TherapyFadhly SharimanAinda não há avaliações
- SBA Usm Aug 15Documento7 páginasSBA Usm Aug 15Fadhly SharimanAinda não há avaliações
- Case Presentation: Management of Newly Diagnosed Type 2 Diabetes MellitusDocumento7 páginasCase Presentation: Management of Newly Diagnosed Type 2 Diabetes MellitusFadhly SharimanAinda não há avaliações
- Sba Part Ii ConjointDocumento24 páginasSba Part Ii ConjointFadhly SharimanAinda não há avaliações
- Post-Operative Complications PresentationDocumento37 páginasPost-Operative Complications PresentationChrisNeop0% (1)
- Family Medicine - SC 2020Documento1 páginaFamily Medicine - SC 2020Fadhly SharimanAinda não há avaliações
- DR SharimanDocumento6 páginasDR SharimanFadhly SharimanAinda não há avaliações
- Necrotizing FasiitisDocumento30 páginasNecrotizing FasiitisFadhly SharimanAinda não há avaliações
- Necrotizing FasiitisDocumento30 páginasNecrotizing FasiitisFadhly SharimanAinda não há avaliações
- Principles of Safe LaparosDocumento28 páginasPrinciples of Safe Laparosolyviutza16Ainda não há avaliações
- Basic Abnormal ECG FadhlyDocumento55 páginasBasic Abnormal ECG FadhlyFadhly SharimanAinda não há avaliações
- Abnormal ECG Fadhly SharimanDocumento55 páginasAbnormal ECG Fadhly SharimanFadhly SharimanAinda não há avaliações
- 11-21-07 Necrotizing Fasciitis RavanosDocumento16 páginas11-21-07 Necrotizing Fasciitis RavanosFadhly SharimanAinda não há avaliações
- RMT Gout DR Blondina 2009Documento67 páginasRMT Gout DR Blondina 2009Fadhly SharimanAinda não há avaliações
- Osteoporosis: Blondina Marpaung Rheumatology Division Internal Department Medical Faculty USU - MedanDocumento47 páginasOsteoporosis: Blondina Marpaung Rheumatology Division Internal Department Medical Faculty USU - MedanFadhly SharimanAinda não há avaliações
- RMT OA DR Blondina 2009Documento41 páginasRMT OA DR Blondina 2009Fadhly SharimanAinda não há avaliações
- RMT RA DR Blondina 2009.Ppt EnglishDocumento61 páginasRMT RA DR Blondina 2009.Ppt EnglishFadhly SharimanAinda não há avaliações
- RMT KLSF DR Blondina 2009Documento21 páginasRMT KLSF DR Blondina 2009Fadhly SharimanAinda não há avaliações
- Wound Healing SchwartzDocumento37 páginasWound Healing SchwartzCarla Putri Chandra100% (1)
- Out 6Documento9 páginasOut 6restu anindityaAinda não há avaliações
- Migraine and Cluster HeadacheDocumento24 páginasMigraine and Cluster HeadachekhemamettaAinda não há avaliações
- Flopamfo 4490Documento15 páginasFlopamfo 4490sabapahty chettiyarAinda não há avaliações
- Guidelines Antibiotic Step-Down TherapyDocumento1 páginaGuidelines Antibiotic Step-Down TherapyGayle GreyAinda não há avaliações
- Gout and Hyperuricemia: PathophysiologyDocumento1 páginaGout and Hyperuricemia: Pathophysiologyسمرة طايبAinda não há avaliações
- February 4, 2015Documento12 páginasFebruary 4, 2015The Delphos HeraldAinda não há avaliações
- USCG EMS Skill Sheets and NREMT Exam GuideDocumento13 páginasUSCG EMS Skill Sheets and NREMT Exam GuideJeffTaborAinda não há avaliações
- Jack Poylangada - Copy of Stamper Self-Care JournalDocumento8 páginasJack Poylangada - Copy of Stamper Self-Care Journalapi-503633296100% (3)
- Emily Morgan - ResumeDocumento2 páginasEmily Morgan - Resumeapi-283578734Ainda não há avaliações
- AWWA Alt Disnfec Fro THM RemovalDocumento264 páginasAWWA Alt Disnfec Fro THM RemovalsaishankarlAinda não há avaliações
- Hospital Waste Water TreatmentDocumento5 páginasHospital Waste Water TreatmentNP100% (1)
- Chronic Limb IschemiaDocumento29 páginasChronic Limb IschemiaSadia NaveedAinda não há avaliações
- Drug Abuse Seminar ProposalDocumento2 páginasDrug Abuse Seminar ProposalNaimul Kader67% (3)
- Premature Rupture of MembranesDocumento5 páginasPremature Rupture of MembranesJoselyn San MiguelAinda não há avaliações
- HemorrhageDocumento15 páginasHemorrhageMariegreat Piscos BisnarAinda não há avaliações
- Repertory: Information On Health Concerns in A Health DirectoryDocumento17 páginasRepertory: Information On Health Concerns in A Health DirectoryShalinta Dubey SharmaAinda não há avaliações
- OLFU Intesive Post Test 50 ItemsDocumento5 páginasOLFU Intesive Post Test 50 ItemsmonmonAinda não há avaliações
- Analgezia Si Anestezia in Obstetrica. Analgezia IN Travaliu: IndicatiiDocumento31 páginasAnalgezia Si Anestezia in Obstetrica. Analgezia IN Travaliu: IndicatiiAlex GrigoreAinda não há avaliações
- Twins Bootcamp StudyDocumento5 páginasTwins Bootcamp Studyandi dirhanAinda não há avaliações
- Doping in SportsDocumento9 páginasDoping in Sportsursvenki4ever3793Ainda não há avaliações
- Abutments in Fixed Partial DenturesDocumento19 páginasAbutments in Fixed Partial DenturesKashish08Ainda não há avaliações
- Monoclonal Antibodies The Next Generation April 2010Documento10 páginasMonoclonal Antibodies The Next Generation April 2010Al ChevskyAinda não há avaliações
- AHA ACLS Provider Manual $45Documento2 páginasAHA ACLS Provider Manual $45Jigar GandhiAinda não há avaliações
- English Iii: University of Guayaquil Facultad Piloto de OdontologíaDocumento4 páginasEnglish Iii: University of Guayaquil Facultad Piloto de OdontologíaDianitaVelezPincayAinda não há avaliações
- Patient Progress Note ProtocolDocumento8 páginasPatient Progress Note ProtocolVito Wilfredo100% (1)
- Nutr 510 - Counseling Session 2Documento4 páginasNutr 510 - Counseling Session 2api-240740872Ainda não há avaliações
- Valium drug guide for nursesDocumento2 páginasValium drug guide for nursesRhea Liza Comendador-TjernmoenAinda não há avaliações
- Who Trs 993 Web FinalDocumento284 páginasWho Trs 993 Web FinalAnonymous 6OPLC9UAinda não há avaliações
- Ethics in GeriatricDocumento22 páginasEthics in GeriatricCessie GutzAinda não há avaliações