Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- (Problem Books in Mathematics) Antonio Caminha Muniz Neto - An Excursion Through Elementary Mathematics, Volume III - Discrete Mathematics and Polynomial Algebra (2018, Springer)Documento647 páginas(Problem Books in Mathematics) Antonio Caminha Muniz Neto - An Excursion Through Elementary Mathematics, Volume III - Discrete Mathematics and Polynomial Algebra (2018, Springer)Anonymous iH6noeaX7100% (2)
- Economics Exam Technique GuideDocumento21 páginasEconomics Exam Technique Guidemalcewan100% (5)
- Post Renaissance Architecture in EuropeDocumento10 páginasPost Renaissance Architecture in Europekali_007Ainda não há avaliações
- Reaction PaperDocumento3 páginasReaction PaperLois DolorAinda não há avaliações
- JMC MSDS Puraspec 1173 (GB)Documento10 páginasJMC MSDS Puraspec 1173 (GB)Benny Samsul B.Ainda não há avaliações
- BarricadeDocumento6 páginasBarricadeJithu PappachanAinda não há avaliações
- 16 - Ocean Currents & Salinity Interactive NotebookDocumento23 páginas16 - Ocean Currents & Salinity Interactive NotebookRaven BraymanAinda não há avaliações
- Actron Vismin ReportDocumento19 páginasActron Vismin ReportSirhc OyagAinda não há avaliações
- Legrand Price List-01 ST April-2014Documento144 páginasLegrand Price List-01 ST April-2014Umesh SutharAinda não há avaliações
- Zero Tolerance 2010Documento16 páginasZero Tolerance 2010Adrian KozelAinda não há avaliações
- Thermal Physics Lecture 1Documento53 páginasThermal Physics Lecture 1Swee Boon OngAinda não há avaliações
- Bagian AwalDocumento17 páginasBagian AwalCitra Monalisa LaoliAinda não há avaliações
- UG ENGLISH Honours PDFDocumento59 páginasUG ENGLISH Honours PDFMR.Shantanu SharmaAinda não há avaliações
- Peanut AllergyDocumento4 páginasPeanut AllergyLNICCOLAIOAinda não há avaliações
- Monitor 14sepDocumento2 páginasMonitor 14sepabhaymvyas1144Ainda não há avaliações
- A Project On "Automatic Water Sprinkler Based On Wet and Dry Conditions"Documento28 páginasA Project On "Automatic Water Sprinkler Based On Wet and Dry Conditions"Srínívas SrínuAinda não há avaliações
- Concise Selina Solutions Class 9 Maths Chapter 15 Construction of PolygonsDocumento31 páginasConcise Selina Solutions Class 9 Maths Chapter 15 Construction of Polygonsbhaskar51178Ainda não há avaliações
- Pepsico SDM ProjectDocumento6 páginasPepsico SDM ProjectJemini GanatraAinda não há avaliações
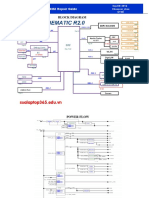
- Asus x453Documento5 páginasAsus x453Rhiry Ntuh AthryAinda não há avaliações
- Acceptable Use Policy 08 19 13 Tia HadleyDocumento2 páginasAcceptable Use Policy 08 19 13 Tia Hadleyapi-238178689Ainda não há avaliações
- SCIENCE 11 WEEK 6c - Endogenic ProcessDocumento57 páginasSCIENCE 11 WEEK 6c - Endogenic ProcessChristine CayosaAinda não há avaliações
- You Can't Blame A FireDocumento8 páginasYou Can't Blame A FireMontana QuarterlyAinda não há avaliações
- Fuentes v. Office of The Ombudsman - MindanaoDocumento6 páginasFuentes v. Office of The Ombudsman - MindanaoJ. JimenezAinda não há avaliações
- Quotation - 1Documento4 páginasQuotation - 1haszirul ameerAinda não há avaliações
- 2015 NSPC Proposed Changes Book PDFDocumento268 páginas2015 NSPC Proposed Changes Book PDFMichelle Pinohermoso JabatAinda não há avaliações
- Eng Notes2Documento10 páginasEng Notes2Arti KapurAinda não há avaliações
- Canon I-SENSYS MF411dw Parts CatalogDocumento79 páginasCanon I-SENSYS MF411dw Parts Catalogmarian100% (1)
- Dist - Propor.danfoss PVG32Documento136 páginasDist - Propor.danfoss PVG32Michal BujaraAinda não há avaliações
- Linux ProgramDocumento131 páginasLinux ProgramsivashaAinda não há avaliações
- Properties of WaterDocumento23 páginasProperties of WaterNiken Rumani100% (1)