Você também pode gostar
- NCPDocumento4 páginasNCPElbert Vierneza100% (2)
- Hypertension Nursing Care PlanDocumento3 páginasHypertension Nursing Care PlanAsylla PajijiAinda não há avaliações
- NCP For RS-HF (Cor PulmonaleDocumento5 páginasNCP For RS-HF (Cor PulmonaleMika Saldaña100% (1)
- Cues: Subjective/ Objective Background of The Disease Nursing Diagnosis Goal/ Objectives Intervention Rationale EvaluationDocumento3 páginasCues: Subjective/ Objective Background of The Disease Nursing Diagnosis Goal/ Objectives Intervention Rationale EvaluationMaria Margaret Macasaet0% (1)
- CHF NCPDocumento8 páginasCHF NCPZy Hallasgo100% (1)
- Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationsDocumento3 páginasAssessment Nursing Diagnosis Planning Interventions Rationale EvaluationsAjay SupanAinda não há avaliações
- Nursing Care Plan For CHFDocumento7 páginasNursing Care Plan For CHFRosemarie Carpio100% (5)
- NCP AnginaDocumento3 páginasNCP AnginaShie LA100% (1)
- Nursing Care Plan Congestive Heart FailureDocumento2 páginasNursing Care Plan Congestive Heart FailureRalph Dumawaa60% (5)
- Nursing Care Plan For Myocardial InfarctionDocumento7 páginasNursing Care Plan For Myocardial InfarctionjamieboyRN88% (8)
- NCP Heart FailureDocumento2 páginasNCP Heart FailureDayan Cabriga100% (1)
- NCP Myocardial InfarctionDocumento1 páginaNCP Myocardial InfarctionjamieboyRN88% (8)
- NCP Inffective Tissue PerfusionDocumento3 páginasNCP Inffective Tissue PerfusionPaul Cubacub0% (1)
- NURSING CARE PLAN For Myocardial InfarctionDocumento16 páginasNURSING CARE PLAN For Myocardial InfarctionFreisanChenMandumotan100% (1)
- NCP AfDocumento3 páginasNCP AfAngelica Mercado SirotAinda não há avaliações
- NCP For Mi PainDocumento2 páginasNCP For Mi PainKahMallariAinda não há avaliações
- Nursing Care Plans For Decreased Cardiac OutputDocumento4 páginasNursing Care Plans For Decreased Cardiac OutputCarmela Balderas Romantco80% (5)
- Decreased Cardiac OutputDocumento3 páginasDecreased Cardiac OutputTiffany Mathis100% (1)
- Impaired Physical MobilityDocumento8 páginasImpaired Physical MobilityKM78% (9)
- CKD NCPDocumento4 páginasCKD NCPArlene Macatangay100% (1)
- NCP #1 Acute Pain Related To Decreased Blood Supply Nursing Diagnosis Scientific Explanation Planning Interventions Rationale Expected OutcomeDocumento22 páginasNCP #1 Acute Pain Related To Decreased Blood Supply Nursing Diagnosis Scientific Explanation Planning Interventions Rationale Expected OutcomeAnnAinda não há avaliações
- Myocarditis NCP 2Documento8 páginasMyocarditis NCP 2astro_aaron117375% (4)
- Nursing Care Plan - Myocardial InfarctionDocumento3 páginasNursing Care Plan - Myocardial Infarctionderic80% (10)
- Heart Failure Nursing Care Plans - 15 Nursing Diagnosis - NurseslabsDocumento13 páginasHeart Failure Nursing Care Plans - 15 Nursing Diagnosis - NurseslabsJOSHUA DICHOSOAinda não há avaliações
- NURSING CARE PLAN Decreased Cardiac Output FnaDocumento2 páginasNURSING CARE PLAN Decreased Cardiac Output FnaAce Dioso Tubasco100% (1)
- Decreased Cardiac OutputDocumento3 páginasDecreased Cardiac OutputRizalyn QuindipanAinda não há avaliações
- NCP Format 3 CKD Chronic Kidney Disease DM Diabetes Mellitus NephropathyDocumento3 páginasNCP Format 3 CKD Chronic Kidney Disease DM Diabetes Mellitus NephropathyAngie MandeoyaAinda não há avaliações
- Decreased Cardiac OutputDocumento2 páginasDecreased Cardiac OutputEdrianne J.100% (2)
- NCP IcuDocumento12 páginasNCP IcuHazel Palomares50% (2)
- Acute Pain Related To Tissue Trauma and InjuryDocumento4 páginasAcute Pain Related To Tissue Trauma and Injuryprickybiik50% (2)
- Ineffective Tissue PerfusionDocumento1 páginaIneffective Tissue PerfusionEuanne Orellano85% (13)
- NCP For CHF 3 Activity IntoleranceDocumento2 páginasNCP For CHF 3 Activity IntoleranceAngelyn ArdinesAinda não há avaliações
- Ineffective Renal Tissue PerfusionDocumento2 páginasIneffective Renal Tissue PerfusionHendra Tanjung100% (4)
- NCP - Excess Fluid Volume (Aortic Stenosis)Documento3 páginasNCP - Excess Fluid Volume (Aortic Stenosis)Daniel Vergara Arce100% (3)
- Decrease Cardiac OutputDocumento6 páginasDecrease Cardiac OutputGerardeanne ReposarAinda não há avaliações
- NCP Impaired Cerebral Tissue PerfussionDocumento4 páginasNCP Impaired Cerebral Tissue PerfussionYvonne Ronamae100% (2)
- NCP - Risk For InfectionDocumento2 páginasNCP - Risk For InfectionJet Bautista100% (1)
- NCP For StrokeDocumento4 páginasNCP For StrokeJASON OGALESCOAinda não há avaliações
- Nursing Care of CHF (Congestive Heart Failure)Documento25 páginasNursing Care of CHF (Congestive Heart Failure)Irwan100% (2)
- NCP For Acute Coronary SyndromeDocumento3 páginasNCP For Acute Coronary Syndromesarahtot75% (4)
- NCP For CHFDocumento2 páginasNCP For CHFMayet De Castro Lejano100% (1)
- Decreased Cardiac Output NCPDocumento2 páginasDecreased Cardiac Output NCPbaba69baba100% (1)
- NCP Ineffective Tissue Perfusion and Self Care DeficitDocumento5 páginasNCP Ineffective Tissue Perfusion and Self Care DeficitFrances Anne Pasiliao100% (3)
- NCP Chest PainDocumento2 páginasNCP Chest PainLinsae Troy50% (2)
- NCP CVDDocumento5 páginasNCP CVDaejel1889% (9)
- B. Inggris PPT NCP Kel. 6Documento9 páginasB. Inggris PPT NCP Kel. 6Emi LestariAinda não há avaliações
- NCP Sa Sinus Tachycardia FinalDocumento13 páginasNCP Sa Sinus Tachycardia FinalMYKRISTIE JHO MENDEZAinda não há avaliações
- Identify Non-Modifiable and Modifiable Risk Factors For HypertensionDocumento3 páginasIdentify Non-Modifiable and Modifiable Risk Factors For HypertensionwokorowAinda não há avaliações
- Tabije, Arvie Jayselle PDocumento6 páginasTabije, Arvie Jayselle PJayselle ArvieAinda não há avaliações
- 1-!nursing Diagnosis:: Myocardial Infarction As Evidenced by Reports of Chest Pain With Radiation in Bilateral ArmDocumento3 páginas1-!nursing Diagnosis:: Myocardial Infarction As Evidenced by Reports of Chest Pain With Radiation in Bilateral Armون توAinda não há avaliações
- Hypertension Nursing Care PlanDocumento3 páginasHypertension Nursing Care Plangeng gengAinda não há avaliações
- Actual Nursing Care Plan #1: Deficient Fluid VolumeDocumento7 páginasActual Nursing Care Plan #1: Deficient Fluid VolumeAubrey SungaAinda não há avaliações
- Nursing Care PlanDocumento4 páginasNursing Care Planmanu_gutierrez0891% (11)
- Assessmen T Diagnosis Planning Intervention Rationale EvaluationDocumento3 páginasAssessmen T Diagnosis Planning Intervention Rationale EvaluationPeter Emmil GonzalesAinda não há avaliações
- Dizziness and Loss of Consciousness: Cardiovascular CausesDocumento4 páginasDizziness and Loss of Consciousness: Cardiovascular CausesMohammedAinda não há avaliações
- Nursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveDocumento2 páginasNursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveFreisanChenMandumotanAinda não há avaliações
- Risk For Decreased Cardiac Output: Nursing DiagnosisDocumento4 páginasRisk For Decreased Cardiac Output: Nursing DiagnosisRiska RamadaniAinda não há avaliações
- Decreased Cardiac Output Related To Decreased Myocardial Contractility Secondary To CardiomyopathyDocumento2 páginasDecreased Cardiac Output Related To Decreased Myocardial Contractility Secondary To CardiomyopathySoniaMarieBalanayAinda não há avaliações
- Group 1 - VITALS SIGNS and INTERVENTIONSDocumento19 páginasGroup 1 - VITALS SIGNS and INTERVENTIONSTrishAinda não há avaliações
- Decreased Cardiac Output Related To Decreased Myocardial Contractility Secondary To CardiomyopathyDocumento2 páginasDecreased Cardiac Output Related To Decreased Myocardial Contractility Secondary To Cardiomyopathywen_pil75% (8)
- NCP CaseDocumento34 páginasNCP CaseIsobel Mae JacelaAinda não há avaliações
- Nursing Process of A Client With CholelithiasisDocumento21 páginasNursing Process of A Client With Cholelithiasisapi-3822508100% (6)
- Term Paper On MOTIVATION THEORIESDocumento30 páginasTerm Paper On MOTIVATION THEORIEScoolhotim81% (32)
- A 20 Year Old Man Suffered From A Spinal Cord Injury at The C2 To C3 Level As The Result of A Motorcycle AccidentDocumento4 páginasA 20 Year Old Man Suffered From A Spinal Cord Injury at The C2 To C3 Level As The Result of A Motorcycle AccidentqingwenAinda não há avaliações
- Pulmonary HypertensionDocumento10 páginasPulmonary HypertensionqingwenAinda não há avaliações
- Periodization and Progress PDFDocumento28 páginasPeriodization and Progress PDFtpAinda não há avaliações
- FM-HS-240-01.7 Full Mob For Use Rev4Documento5 páginasFM-HS-240-01.7 Full Mob For Use Rev4VZAinda não há avaliações
- The Lecture About Middle Meridan From Pang LaoshiiDocumento8 páginasThe Lecture About Middle Meridan From Pang LaoshiiEliud ArmandAinda não há avaliações
- Neurologic NCLEX Practice Test Part 1Documento18 páginasNeurologic NCLEX Practice Test Part 1Hasan A AsFourAinda não há avaliações
- RRL NotesDocumento5 páginasRRL NotesAndrea LeonorAinda não há avaliações
- The Diagnosis of Fibromyalgia Syndrome Guidelines - 1 - 0Documento57 páginasThe Diagnosis of Fibromyalgia Syndrome Guidelines - 1 - 0Firstiafina TiffanyAinda não há avaliações
- Stress and Job Performance of Secretaries in An OrganizationDocumento6 páginasStress and Job Performance of Secretaries in An OrganizationWilliam NjeruAinda não há avaliações
- Disorders of Integrative Function 2 - 2020Documento15 páginasDisorders of Integrative Function 2 - 2020Cres Padua QuinzonAinda não há avaliações
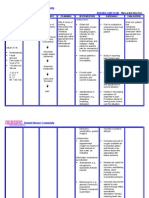
- Cues Nursing Diagnosis Background Knowledge Goal and Objective Nursing Interventions & Rationale EvaluationDocumento4 páginasCues Nursing Diagnosis Background Knowledge Goal and Objective Nursing Interventions & Rationale Evaluationtherese BAinda não há avaliações
- Rule Book: Kickstarter Version 1.0Documento34 páginasRule Book: Kickstarter Version 1.0Maschem0% (2)
- Genmath 11 q1 w4 Mod10Documento9 páginasGenmath 11 q1 w4 Mod10Barez Fernandez ZacAinda não há avaliações
- NURSING CARE PLAN - SuicidalactDocumento4 páginasNURSING CARE PLAN - SuicidalactJennifer ArdeAinda não há avaliações
- Analisis Kelelahan Mahasiswa Teknik Industri Reguler B Di Universitas Widyatama Menggunakan Fatigue AssesmentDocumento7 páginasAnalisis Kelelahan Mahasiswa Teknik Industri Reguler B Di Universitas Widyatama Menggunakan Fatigue AssesmentREG.A/40521190006/DEDE FALAHAinda não há avaliações
- Endocrine System Assessment.Documento30 páginasEndocrine System Assessment.ramoli1988100% (2)
- Toward A Consensus Description of Vocal Effort, Vocal Load, Vocal Loading, and Vocal FatigueDocumento25 páginasToward A Consensus Description of Vocal Effort, Vocal Load, Vocal Loading, and Vocal FatigueChris100% (1)
- Driving Core CBLM UC2 - NEW FinalDocumento36 páginasDriving Core CBLM UC2 - NEW FinalRomally Antonette TagnipezAinda não há avaliações
- Healy Program DescriptionsDocumento7 páginasHealy Program DescriptionsCyndi McKennaAinda não há avaliações
- MSCAT - One Page FormatDocumento1 páginaMSCAT - One Page FormatGeorge Espejo100% (1)
- Basic Fatigue Management Training: Prepared For B Otaş - BTC, Feb.-2004Documento37 páginasBasic Fatigue Management Training: Prepared For B Otaş - BTC, Feb.-2004Rauf HuseynovAinda não há avaliações
- Crystal Healing Power PDFDocumento36 páginasCrystal Healing Power PDFrkamundimuAinda não há avaliações
- Jurnal Intra Dial ExercseDocumento70 páginasJurnal Intra Dial ExercseSutiknosaja CukupAinda não há avaliações
- Hydration PaperDocumento7 páginasHydration PaperJosh PilipovskyAinda não há avaliações
- Fatigue ManagementDocumento40 páginasFatigue Managementnaing kyawAinda não há avaliações
- Cues Nursing Diagnosis Scientific Basis Objectives Nursing Intervention Rationale EvaluationDocumento11 páginasCues Nursing Diagnosis Scientific Basis Objectives Nursing Intervention Rationale Evaluationjoyrena ochondraAinda não há avaliações
- Uncorrected Author Proof: Split-Shift Work in Relation To Stress, Health and Psychosocial Work Factors Among Bus DriversDocumento8 páginasUncorrected Author Proof: Split-Shift Work in Relation To Stress, Health and Psychosocial Work Factors Among Bus DriversAkbarAinda não há avaliações
- Water Therapy Manual: by Vance FerrellDocumento114 páginasWater Therapy Manual: by Vance FerrellShoshannah100% (6)
- HomeopathyDocumento32 páginasHomeopathyavidmasterAinda não há avaliações
- FibromyelgiaDocumento3 páginasFibromyelgiaTapash NathAinda não há avaliações
- Burnout PPT (1) (1) FINALDocumento15 páginasBurnout PPT (1) (1) FINALrabia khalidAinda não há avaliações
- Using Power Data For Assessing Relative Endurance and Stamina in Runners: Fatigue Resistance MetricsDocumento6 páginasUsing Power Data For Assessing Relative Endurance and Stamina in Runners: Fatigue Resistance MetricsmaorpeAinda não há avaliações