Você também pode gostar
- Manual G Ingles - V6Documento68 páginasManual G Ingles - V6Phùng Thế Kiên50% (2)
- NCM 102 SyllabusDocumento1 páginaNCM 102 SyllabusrosanowardAinda não há avaliações
- Effectivness of PNF Stretching and Self Stretching in Patients With Adhesive Capsulitis - A Comparative Study Pag 53Documento300 páginasEffectivness of PNF Stretching and Self Stretching in Patients With Adhesive Capsulitis - A Comparative Study Pag 53Francisca Lidia Jujihara100% (1)
- C+F-Intracranial Pressure in Dogs and CatsDocumento13 páginasC+F-Intracranial Pressure in Dogs and Catstaner_soysuren100% (2)
- Infectious Diseases in CamelidsDocumento404 páginasInfectious Diseases in CamelidsEloisa Zúñiga100% (4)
- AWP 4A Syllabus Fall 2021 (Misinformation)Documento11 páginasAWP 4A Syllabus Fall 2021 (Misinformation)camAinda não há avaliações
- Augusta Issue 1145 - The Jail ReportDocumento24 páginasAugusta Issue 1145 - The Jail ReportGreg RickabaughAinda não há avaliações
- 43 Best Passive Income Streams & OpportunitiesDocumento7 páginas43 Best Passive Income Streams & OpportunitiesEri Nur Sofa50% (2)
- AS Film Production Lesson.Documento13 páginasAS Film Production Lesson.MsCowanAinda não há avaliações
- Advances in Veterinary Antimicrobial Therapy and Forensic ToxicologyDocumento230 páginasAdvances in Veterinary Antimicrobial Therapy and Forensic ToxicologySunilAinda não há avaliações
- Ijmrhs Vol 3 Issue 3Documento271 páginasIjmrhs Vol 3 Issue 3editorijmrhsAinda não há avaliações
- Montina L TabletDocumento10 páginasMontina L TabletKrish Yemkay100% (1)
- Bayer A1CNow HCP Product InsertDocumento11 páginasBayer A1CNow HCP Product InsertLindsay YooAinda não há avaliações
- Guidelines For The Use of Fresh-Frozen Plasma, CryoprecipitateDocumento18 páginasGuidelines For The Use of Fresh-Frozen Plasma, CryoprecipitatemelaniefarahdillaAinda não há avaliações
- المختصر الجم في فحص الدمDocumento116 páginasالمختصر الجم في فحص الدمmanni1001Ainda não há avaliações
- C 17Documento12 páginasC 17Tammie Gore100% (1)
- Lab Exercises Intro To MicrobiologyDocumento71 páginasLab Exercises Intro To MicrobiologyAygul RamankulovaAinda não há avaliações
- Sonic and Ultrasonic ScalersDocumento10 páginasSonic and Ultrasonic ScalersAhmad Abd El-GhaniAinda não há avaliações
- Unpaid Free JournalsDocumento426 páginasUnpaid Free JournalsNonihal Chavhan HappylifeAinda não há avaliações
- Botox, CalfDocumento5 páginasBotox, Calfneat77Ainda não há avaliações
- Modul1Documento11 páginasModul1Joni Witzi0% (2)
- COVID-19 - The Nursing Home DiseaseDocumento13 páginasCOVID-19 - The Nursing Home DiseaseJon DeckerAinda não há avaliações
- HASTING CENTER The Privacy Rule That's NotDocumento11 páginasHASTING CENTER The Privacy Rule That's NotIon Arrieta ValeroAinda não há avaliações
- Declaration HelsinkiDocumento4 páginasDeclaration HelsinkiHemant Bhansali0% (1)
- International Journal of Engineering Research and Development (IJERD)Documento3 páginasInternational Journal of Engineering Research and Development (IJERD)IJERDAinda não há avaliações
- NANDA DX NI, NODocumento165 páginasNANDA DX NI, NOKerry Brown100% (1)
- Blue Writing Is What I Added To These Notes: RadiographyDocumento46 páginasBlue Writing Is What I Added To These Notes: Radiographybjpalmer100% (2)
- 15-17 - 7-PDF - Community Medicine With Recent Advances - 3 PDFDocumento3 páginas15-17 - 7-PDF - Community Medicine With Recent Advances - 3 PDFdwimahesaputraAinda não há avaliações
- June NP2Documento18 páginasJune NP2Rem YrizAinda não há avaliações
- Mirtazapine As An Appetite Stimulant and Anti-Emetic in Cats With Chronic Kidney Disease: A Masked Placebo-Controlled Crossover Clinical TrialDocumento5 páginasMirtazapine As An Appetite Stimulant and Anti-Emetic in Cats With Chronic Kidney Disease: A Masked Placebo-Controlled Crossover Clinical TrialWilliam ChandlerAinda não há avaliações
- Artificial Red Blood Cells RBC Using NanotechnologyDocumento11 páginasArtificial Red Blood Cells RBC Using NanotechnologyNikky Nair100% (3)
- Scope of Nle1109Documento376 páginasScope of Nle1109ericAinda não há avaliações
- Journal of Allergy and Clinical ImmunologyDocumento265 páginasJournal of Allergy and Clinical Immunologydod_nurAinda não há avaliações
- Reseau Pass24Documento7 páginasReseau Pass24maxleproAinda não há avaliações
- Brachial Plexus InjuriesDocumento345 páginasBrachial Plexus Injuriesmohamedwhatever100% (2)
- Stem Cell Research - For The Benefit of Today and TomorrowDocumento4 páginasStem Cell Research - For The Benefit of Today and Tomorrowjustasm100% (11)
- Antidepressants For The Treatment of InsomniaDocumento8 páginasAntidepressants For The Treatment of Insomniaapi-19853437Ainda não há avaliações
- Community and Public HealthDocumento36 páginasCommunity and Public HealthRamel Yen CerantesAinda não há avaliações
- Lecture 1-Introduction To Dental CariesDocumento4 páginasLecture 1-Introduction To Dental CariesAli Al-Qudsi100% (2)
- Guidelines - Psy Aspects Malnutrition - MSF OCBDocumento31 páginasGuidelines - Psy Aspects Malnutrition - MSF OCBDiego MercadoAinda não há avaliações
- Endocrine and Metabolic EmergenciesDocumento320 páginasEndocrine and Metabolic EmergenciesReem Ben Omran100% (1)
- Journal of International Medical Research 1986 Busson 53 62Documento10 páginasJournal of International Medical Research 1986 Busson 53 62Eureka HimitsuAinda não há avaliações
- Sporlac MonographDocumento84 páginasSporlac Monographavs1123100% (2)
- DuaventDocumento9 páginasDuaventAjurs UrsabiaAinda não há avaliações
- Elements in Human New PerspectivesDocumento32 páginasElements in Human New PerspectivesSahar SalahAinda não há avaliações
- Neurobiology of Disease: ReviewDocumento8 páginasNeurobiology of Disease: ReviewIsyana KhaerunisaAinda não há avaliações
- SiegenthalerDocumento5 páginasSiegenthalerHeinz Purwadi Gunawan-SchoeckAinda não há avaliações
- Unit-I. Epidemiology IntroductionDocumento60 páginasUnit-I. Epidemiology IntroductionAny OneAinda não há avaliações
- Chiropractic PDFDocumento19 páginasChiropractic PDFConstantinescu RasvanAinda não há avaliações
- As 2437-1987 Flusher Sanitizers For Bed Pans and Urine BottlesDocumento8 páginasAs 2437-1987 Flusher Sanitizers For Bed Pans and Urine BottlesSAI Global - APACAinda não há avaliações
- IIHI Ministers Report 170912 FinalDocumento220 páginasIIHI Ministers Report 170912 FinalPanos ZarogoulidisAinda não há avaliações
- Rheumatology Nursing: A Creative ApproachNo EverandRheumatology Nursing: A Creative ApproachJackie HillAinda não há avaliações
- Molecular Hydrogen for Medicine: The Art of Ancient Life RevivedNo EverandMolecular Hydrogen for Medicine: The Art of Ancient Life RevivedAinda não há avaliações
- The Nurse Practitioner in UrologyNo EverandThe Nurse Practitioner in UrologyMichelle LajinessAinda não há avaliações
- CLUSTERS LIST - (CHNCS) GO-209Documento45 páginasCLUSTERS LIST - (CHNCS) GO-209Gadde Srinivasarao67% (3)
- 2010HMF MS294Documento3 páginas2010HMF MS294Gadde SrinivasaraoAinda não há avaliações
- Rural Health Care System in IndiaDocumento22 páginasRural Health Care System in IndiaSumit Singhal58% (12)
- Guidelines For Distt Hospitals - Indian Public Health StandardsDocumento124 páginasGuidelines For Distt Hospitals - Indian Public Health StandardsTejinder SinghAinda não há avaliações
- CHNCDocumento94 páginasCHNCv.srinivasa MurthyAinda não há avaliações
- UPHC Guideliens - UpdatedDocumento34 páginasUPHC Guideliens - Updatedradhe sharmaAinda não há avaliações
- HCDSDocumento35 páginasHCDSKrishnaveni MurugeshAinda não há avaliações
- Sub District Sub-Divisional HospitalDocumento102 páginasSub District Sub-Divisional HospitalVineet Verma100% (1)
- Job Responsibilities of Different Health People PDFDocumento114 páginasJob Responsibilities of Different Health People PDFRuben Paul C RajAinda não há avaliações
- Sub District Sub Divisional HospitalDocumento102 páginasSub District Sub Divisional HospitalGanesh SoniAinda não há avaliações
- PRC New Special Grades Scales 6,12,18,24 YearsDocumento11 páginasPRC New Special Grades Scales 6,12,18,24 YearsSEKHARAinda não há avaliações
- NEW HRA Government of Andhra Pradesh 11-04-2011Documento2 páginasNEW HRA Government of Andhra Pradesh 11-04-2011SEKHARAinda não há avaliações
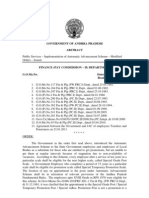
- Go - Ms.no 93 - General TransfersDocumento5 páginasGo - Ms.no 93 - General TransfersGadde Srinivasarao50% (2)
- CLUSTERS LIST - (CHNCS) GO-209Documento45 páginasCLUSTERS LIST - (CHNCS) GO-209Gadde Srinivasarao67% (3)
- Go 92Documento22 páginasGo 92Gadde SrinivasaraoAinda não há avaliações
- CLUSTERS LIST - (CHNCS) GO-209Documento45 páginasCLUSTERS LIST - (CHNCS) GO-209Gadde Srinivasarao67% (3)
- 2010HMF MS297Documento2 páginas2010HMF MS297Gadde SrinivasaraoAinda não há avaliações
- Coding of PostsDocumento167 páginasCoding of PostsGadde SrinivasaraoAinda não há avaliações
- ACCOUNTS FOR 2010-2011: I-IncomeDocumento29 páginasACCOUNTS FOR 2010-2011: I-IncomeGadde SrinivasaraoAinda não há avaliações
- 2010HMF MS294Documento3 páginas2010HMF MS294Gadde SrinivasaraoAinda não há avaliações
- Cas Provisional Seniority List (24.02.2010)Documento42 páginasCas Provisional Seniority List (24.02.2010)Gadde Srinivasarao100% (1)
- Orchid Group of Companies Company ProfileDocumento3 páginasOrchid Group of Companies Company ProfileAngelica Nicole TamayoAinda não há avaliações
- Prepared by M Suresh Kumar, Chief Manager Faculty, SBILD HYDERABADDocumento29 páginasPrepared by M Suresh Kumar, Chief Manager Faculty, SBILD HYDERABADBino JosephAinda não há avaliações
- Lesson Plan 2 BasketballDocumento3 páginasLesson Plan 2 Basketballapi-313716520100% (1)
- Partnership For Sustainable Textiles - FactsheetDocumento2 páginasPartnership For Sustainable Textiles - FactsheetMasum SharifAinda não há avaliações
- Food Product Innovation PDFDocumento35 páginasFood Product Innovation PDFDidik HariadiAinda não há avaliações
- Transcendental Meditaton ProgramDocumento3 páginasTranscendental Meditaton Programacharyaprakash0% (3)
- Explicit Lesson PlanDocumento10 páginasExplicit Lesson PlanBanjo De Los SantosAinda não há avaliações
- Tcs IntroDocumento12 páginasTcs IntroRomi.Roy1820 MBAAinda não há avaliações
- 1623 Asm2Documento21 páginas1623 Asm2Duc Anh nguyenAinda não há avaliações
- 3rd Year. PunctuationDocumento14 páginas3rd Year. PunctuationmawarAinda não há avaliações
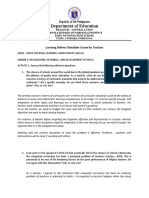
- Department of Education: Republic of The PhilippinesDocumento6 páginasDepartment of Education: Republic of The PhilippinesLalaine QuitoAinda não há avaliações
- Mindset For IELTS Level 1 Student's Book PDF English As A Second or Foreign Language International English Language TestinDocumento1 páginaMindset For IELTS Level 1 Student's Book PDF English As A Second or Foreign Language International English Language TestinhiAinda não há avaliações
- EASA CS-22 Certification of SailplanesDocumento120 páginasEASA CS-22 Certification of SailplanessnorrigAinda não há avaliações
- Tata Motors - Strategic ManagementDocumento16 páginasTata Motors - Strategic ManagementVaishakh MenonAinda não há avaliações
- Chapter 4Documento20 páginasChapter 4Vandan GundaleAinda não há avaliações
- Lorenzo JDocumento2 páginasLorenzo Japi-528402595Ainda não há avaliações
- Mucic Acid Test: PrincipleDocumento3 páginasMucic Acid Test: PrincipleKrizzi Dizon GarciaAinda não há avaliações
- EvoFox Katana-X Mechanical Gaming Keyboard With Outemu Blue Switches Vivid Rainbow Lighting With 13 Preset Effects DedicatedDocumento1 páginaEvoFox Katana-X Mechanical Gaming Keyboard With Outemu Blue Switches Vivid Rainbow Lighting With 13 Preset Effects Dedicatedsaqibdar7051236186Ainda não há avaliações
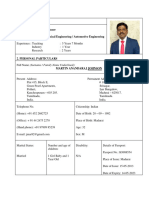
- CV (Martin A Johnson)Documento7 páginasCV (Martin A Johnson)kganesanAinda não há avaliações
- Wincam TornoDocumento3 páginasWincam Tornocaballerillo100% (1)
- Sow and Learning ObjectivesDocumento14 páginasSow and Learning ObjectivesEhsan AzmanAinda não há avaliações
- Simulado InglesDocumento6 páginasSimulado InglesWandercleyson da SilvaAinda não há avaliações
- 1778 3557 1 SM PDFDocumento4 páginas1778 3557 1 SM PDFjulio simanjuntakAinda não há avaliações
- 5EMA BB Dem&Sup VW Bu&Se - 2.35&48&PDDocumento13 páginas5EMA BB Dem&Sup VW Bu&Se - 2.35&48&PDkashinath09Ainda não há avaliações
- GSM Sniffing - Telegraph+Documento9 páginasGSM Sniffing - Telegraph+Sridhar PAinda não há avaliações