Você também pode gostar
- Pre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandPre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Premature Rupture of Membranes (Prom)Documento12 páginasPremature Rupture of Membranes (Prom)KABERA RENE50% (2)
- Premature Rupture of MembranesDocumento4 páginasPremature Rupture of MembranesNikko Pabico67% (3)
- Abruptio Placenta FullDocumento10 páginasAbruptio Placenta FullChester ManaloAinda não há avaliações
- Premature Rupture of Membranes (PROMDocumento15 páginasPremature Rupture of Membranes (PROMRima HajjarAinda não há avaliações
- Case Report - PromDocumento16 páginasCase Report - PromFauziyyahrAinda não há avaliações
- JMDocumento45 páginasJMDana Fajardo RezanoAinda não há avaliações
- Myoma: Causes of Uterine Fibroid or MyomaDocumento15 páginasMyoma: Causes of Uterine Fibroid or MyomaHannah Katrina Almoro AlmedaAinda não há avaliações
- NSVDDocumento48 páginasNSVDchiqui14100% (2)
- Abruptio PlacentaDocumento45 páginasAbruptio PlacentaJosef Kevin ArcillaAinda não há avaliações
- Ectopic Pregnancy Study GuideDocumento5 páginasEctopic Pregnancy Study GuideCarl Elexer Cuyugan Ano100% (1)
- Placenta Abruptio - Topic OverviewDocumento8 páginasPlacenta Abruptio - Topic OverviewLei AbellarAinda não há avaliações
- Case Study Placenta Previa This Is It 1Documento71 páginasCase Study Placenta Previa This Is It 1Homework Ping100% (1)
- Case Study PIHDocumento26 páginasCase Study PIHChen OmbrosaAinda não há avaliações
- H MoleDocumento7 páginasH MoleRaymond Christopher LimAinda não há avaliações
- Generic Name Brand Name Dosage Indications Mechanisms of Action Adverse Effects Nursing ResponsibilitiesDocumento10 páginasGeneric Name Brand Name Dosage Indications Mechanisms of Action Adverse Effects Nursing ResponsibilitiesJennalyn CasapaoAinda não há avaliações
- Incompetent CervixDocumento5 páginasIncompetent CervixNaidin Catherine De Guzman-Alcala100% (1)
- Neonatal Sepsis Case 2Documento81 páginasNeonatal Sepsis Case 2Joanne Bernadette Aguilar100% (1)
- Premature Rupture of MembranesDocumento33 páginasPremature Rupture of MembranesSarang Lee100% (1)
- Case Study PreeclampsiaDocumento3 páginasCase Study PreeclampsiaRima Christa Ulin SitepuAinda não há avaliações
- NCP Drug Study Group 1Documento21 páginasNCP Drug Study Group 1Cassandra Grace Muerong Dela CruzAinda não há avaliações
- Incomplete Abortion MINI CASE STUDY Group 3Documento23 páginasIncomplete Abortion MINI CASE STUDY Group 3Katrina TinapianAinda não há avaliações
- CP Hydatidiform MoleDocumento13 páginasCP Hydatidiform Molesweetheart_joannieAinda não há avaliações
- Case Study MiscariageDocumento14 páginasCase Study MiscariagesexiiimammaAinda não há avaliações
- Abruptio Placenta Mini Case StudyDocumento20 páginasAbruptio Placenta Mini Case StudyAira AlaroAinda não há avaliações
- Hyperemesis GravidarumDocumento3 páginasHyperemesis GravidarumAldrece Castroverde100% (1)
- CASE ANALYSIS Ectopic Pregnancy Part 1Documento10 páginasCASE ANALYSIS Ectopic Pregnancy Part 1Diane Celine SantianoAinda não há avaliações
- Case Study - Incomplete Abortion Related To APSDocumento8 páginasCase Study - Incomplete Abortion Related To APSRomeo ReyesAinda não há avaliações
- NSDDocumento44 páginasNSDabyssodeep100% (1)
- Case Study in ObwardDocumento6 páginasCase Study in Obwardcharles_florendo25100% (3)
- Placenta Previa Case StudyDocumento7 páginasPlacenta Previa Case StudyphearlieAinda não há avaliações
- Incomplete AbortionDocumento22 páginasIncomplete AbortionAJ Dalawampu100% (2)
- Incompetent CervixDocumento4 páginasIncompetent CervixCharm Arroyo100% (1)
- Evaluation of Fetal DeathDocumento9 páginasEvaluation of Fetal DeathVinisia TakaraiAinda não há avaliações
- H Mole Case PresentationDocumento12 páginasH Mole Case PresentationjisooAinda não há avaliações
- The High Risk PregnancyDocumento23 páginasThe High Risk Pregnancynursereview100% (3)
- Managing Abruptio PlacentaDocumento29 páginasManaging Abruptio PlacentaAudrey DelfinAinda não há avaliações
- Discharge Care Plan Abruptio PlacentaDocumento4 páginasDischarge Care Plan Abruptio PlacentaJean nicole GaribayAinda não há avaliações
- Teaching Plan On Newborn ScreeningDocumento8 páginasTeaching Plan On Newborn ScreeningQueenie Sicco100% (1)
- Problems of the Passageway and Psyche Factors in LaborDocumento1 páginaProblems of the Passageway and Psyche Factors in LaborAirishAinda não há avaliações
- Uterine AtonyDocumento33 páginasUterine AtonyNonie 'Erni' HastiriniAinda não há avaliações
- Problems of The PassengerDocumento9 páginasProblems of The PassengerDanah Grace SanchezAinda não há avaliações
- Incompetent CervixDocumento29 páginasIncompetent CervixCyrelle Jen TorresAinda não há avaliações
- Excess Amniotic Fluid Causes and DiagnosisDocumento2 páginasExcess Amniotic Fluid Causes and DiagnosisAde Yonata100% (1)
- Uterine MYOMADocumento5 páginasUterine MYOMARoss Manalang100% (2)
- Normal Spontaneous Vaginal DeliveryDocumento11 páginasNormal Spontaneous Vaginal DeliveryKristine Valenton67% (3)
- Spontaneous AbortionDocumento17 páginasSpontaneous Abortionanon_985338331Ainda não há avaliações
- Abruptio PlacentaDocumento60 páginasAbruptio PlacentaSindhu JojoAinda não há avaliações
- Nursing Care of Hydatidiform MoleDocumento23 páginasNursing Care of Hydatidiform MoleKristel Rivamonte100% (1)
- CASE STUDY Acute Pain Related To Laceration 1Documento29 páginasCASE STUDY Acute Pain Related To Laceration 1Maria Jessica Dumdum100% (1)
- Nursing Care PlanDocumento3 páginasNursing Care PlanArvan James Cabugayan TalboAinda não há avaliações
- Abruptio PlacentaDocumento3 páginasAbruptio Placentachichilovesyou100% (1)
- Group 2. Ectopic PregnancyDocumento61 páginasGroup 2. Ectopic PregnancyIvan Laurentine Aceret100% (1)
- A Case Analysis OnDocumento27 páginasA Case Analysis Onbunso padillaAinda não há avaliações
- NCP Abruptio PlacentaDocumento2 páginasNCP Abruptio PlacentaCarson Birth100% (1)
- REFERAT - Ppt.pathophysiology of PROM-noviDocumento16 páginasREFERAT - Ppt.pathophysiology of PROM-noviFrisma Indah Permatasari100% (1)
- NCP Case 1Documento6 páginasNCP Case 1boomer SeargeAinda não há avaliações
- Incomplete AbortionDocumento18 páginasIncomplete AbortionAra DirganAinda não há avaliações
- Abortionsource 100605123737 Phpapp01Documento38 páginasAbortionsource 100605123737 Phpapp01Erina Erichan OtoAinda não há avaliações
- Preterm / Premature Labor: EtiologyDocumento8 páginasPreterm / Premature Labor: EtiologyCheney BalbuenaAinda não há avaliações
- STAGING For Cervical CADocumento1 páginaSTAGING For Cervical CASheena KunkelAinda não há avaliações
- Cervical CancerDocumento9 páginasCervical CancerSheena KunkelAinda não há avaliações
- Group2 SUMMARY OF CASESDocumento1 páginaGroup2 SUMMARY OF CASESSheena KunkelAinda não há avaliações
- Group 2 Ms ReportDocumento17 páginasGroup 2 Ms ReportSheena KunkelAinda não há avaliações
- TB MDR Ruth Putri-1510015071Documento16 páginasTB MDR Ruth Putri-1510015071Elizabeth SagalaAinda não há avaliações
- Diary Curriculum Map Subject: Mapeh-Health 8 Grade Level: 8 Teacher (S) : Jescil O. Mulit Junior High SchoolDocumento10 páginasDiary Curriculum Map Subject: Mapeh-Health 8 Grade Level: 8 Teacher (S) : Jescil O. Mulit Junior High SchoolJescil Oñez MulitAinda não há avaliações
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocumento1 páginaCertificate For COVID-19 Vaccination: Beneficiary Detailssoma GamerAinda não há avaliações
- Strokescenarioinindia Isp 170727022013Documento10 páginasStrokescenarioinindia Isp 170727022013Ajjugal SushmajaAinda não há avaliações
- Inbound 6622251263463521221Documento2 páginasInbound 6622251263463521221Haji Ehsan Ullah EhsanAinda não há avaliações
- Promoting Reproductive and Sexual HealthDocumento20 páginasPromoting Reproductive and Sexual HealthShiela Marie BanggotAinda não há avaliações
- Effectiveness of reflex zone stimulation on lactation post-C-sectionDocumento30 páginasEffectiveness of reflex zone stimulation on lactation post-C-sectionAGERI PUSHPALATHAAinda não há avaliações
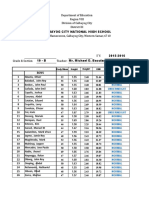
- SF 8 Learner's Basic Health and Nutrition ReportDocumento2 páginasSF 8 Learner's Basic Health and Nutrition ReportKenneth Jay BagandoAinda não há avaliações
- 02 Pnemococal Pnemonia Vaccine For Elderly During Covid 19 PandemicDocumento46 páginas02 Pnemococal Pnemonia Vaccine For Elderly During Covid 19 PandemicVera YuwanaAinda não há avaliações
- Ipc 2018Documento6 páginasIpc 2018abdullah sahibAinda não há avaliações
- Rujukan: Kempen Cara Hidup Sihat 1997. Kementerian Kesihatan MalaysiaDocumento1 páginaRujukan: Kempen Cara Hidup Sihat 1997. Kementerian Kesihatan MalaysiaArif MuhdAinda não há avaliações
- Dengue Hero-PcpDocumento27 páginasDengue Hero-PcpRomina Mae FajardoAinda não há avaliações
- Roadside Urination and Public Sanitation Facilities in Dhaka, BangladeshDocumento10 páginasRoadside Urination and Public Sanitation Facilities in Dhaka, BangladeshSimanta Kumar SahaAinda não há avaliações
- Pointers in Mapeh 10Documento2 páginasPointers in Mapeh 10HARLEY L. TANAinda não há avaliações
- FMEA 2016-Penyuluhan SingkatDocumento97 páginasFMEA 2016-Penyuluhan Singkatsari rezekiAinda não há avaliações
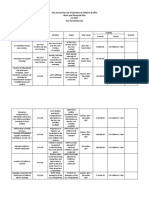
- 2017 CCPC Work and Financial PlanDocumento7 páginas2017 CCPC Work and Financial PlanPatrick Jorge SibayanAinda não há avaliações
- Primary Health CareDocumento41 páginasPrimary Health CareKailash NagarAinda não há avaliações
- Burton's Microbiology For The Health Sciences: Section VIII. Major Infectious Diseases of HumansDocumento29 páginasBurton's Microbiology For The Health Sciences: Section VIII. Major Infectious Diseases of HumansCarmela Laraya Alayon25% (4)
- 3.disease OccuranceDocumento50 páginas3.disease Occurancetatha youngAinda não há avaliações
- Georgia Association of Educators Suit Against StateDocumento51 páginasGeorgia Association of Educators Suit Against StateJonathan RaymondAinda não há avaliações
- Vector ControlDocumento19 páginasVector ControlCalvin CalvinAinda não há avaliações
- Lesson Plan in Health 8Documento4 páginasLesson Plan in Health 8Rhenevoi Bastiero NonatoAinda não há avaliações
- Referencias Bibliográficas: Poliomielitis Paralítica Causada Por La Vacuna Oral Sabin: ¿Tiempo de Cambiar de Vacuna?Documento3 páginasReferencias Bibliográficas: Poliomielitis Paralítica Causada Por La Vacuna Oral Sabin: ¿Tiempo de Cambiar de Vacuna?RoeAinda não há avaliações
- School Water Sanitation PlanDocumento3 páginasSchool Water Sanitation PlanNoican Leira Tnecniv Luap100% (1)
- The Oral-Systemic Disease Connection PDFDocumento2 páginasThe Oral-Systemic Disease Connection PDFJing XueAinda não há avaliações
- Etiology of Cancer PDFDocumento2 páginasEtiology of Cancer PDFWilliam0% (2)
- Job-Specification - House Officer PDFDocumento2 páginasJob-Specification - House Officer PDFIndika2323Ainda não há avaliações
- Callo, John Andrei D. (Regarding Kronos)Documento3 páginasCallo, John Andrei D. (Regarding Kronos)andrei CalloAinda não há avaliações
- BMIDocumento20 páginasBMIMichael Dulza BaculantaAinda não há avaliações
- MDS Course Regulations 1983Documento22 páginasMDS Course Regulations 1983Latest Laws TeamAinda não há avaliações