Você também pode gostar
- Primary Trauma CareDocumento48 páginasPrimary Trauma CareKABERA RENEAinda não há avaliações
- Trauma OverviewDocumento48 páginasTrauma OverviewFrancescoBarbero100% (1)
- ATLS ProtocoloDocumento21 páginasATLS Protocoloedgarjavier65100% (2)
- ATLSDocumento15 páginasATLSsouthstar9989% (9)
- Approach For Poly-Trauma PatientDocumento63 páginasApproach For Poly-Trauma PatientPrince Jeyaraj100% (1)
- Approach To Trauma: UNC Emergency Medicine Medical Student Lecture SeriesDocumento54 páginasApproach To Trauma: UNC Emergency Medicine Medical Student Lecture SeriesAhmed Tawfig GamalAinda não há avaliações
- Abdominal TraumaDocumento60 páginasAbdominal Traumaapi-19916399Ainda não há avaliações
- Abdominal TraumaDocumento60 páginasAbdominal Traumamel_chakAinda não há avaliações
- Approach To TruamaDocumento29 páginasApproach To TruamaIbsa ShumaAinda não há avaliações
- Initial Assessment and Management: Dr. Yunus, Sp. BSDocumento20 páginasInitial Assessment and Management: Dr. Yunus, Sp. BSputrinurulapriliaAinda não há avaliações
- Approach For Poly-Trauma PatientDocumento63 páginasApproach For Poly-Trauma PatientvadimmadanAinda não há avaliações
- TNCC Study GuideDocumento4 páginasTNCC Study Guidernbsntestbanks90% (10)
- TNCC Study GuideDocumento4 páginasTNCC Study Guidescroasdell83% (6)
- Principles of Trauma ManagementDocumento60 páginasPrinciples of Trauma ManagementDrArish Mahmood100% (1)
- Trauma Resuscitation Acute Care Emerg MedDocumento67 páginasTrauma Resuscitation Acute Care Emerg MedsyasyaAinda não há avaliações
- Of The Multiply Injured PatientDocumento29 páginasOf The Multiply Injured PatientAjay DherwaniAinda não há avaliações
- W1L1 - Initial Assessment For Trauma - 2Documento44 páginasW1L1 - Initial Assessment For Trauma - 2Baihaqi SaharunAinda não há avaliações
- General Management of Trauma: Dr. Ho Ngoc PhatDocumento34 páginasGeneral Management of Trauma: Dr. Ho Ngoc PhatarcadyAinda não há avaliações
- Initial Assessment AND ManagementDocumento30 páginasInitial Assessment AND ManagementSikaAinda não há avaliações
- Polytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaDocumento57 páginasPolytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaAbuhafezbaka100% (1)
- (Advanced Trauma Life Support) Moderator: Dr. Deepak S: Ganesh Kumar VIII TermDocumento20 páginas(Advanced Trauma Life Support) Moderator: Dr. Deepak S: Ganesh Kumar VIII Termabhaymalur100% (1)
- Care of Trauma Patient: Nursing Process & Critical Thinking IVDocumento54 páginasCare of Trauma Patient: Nursing Process & Critical Thinking IVMarten HumphreyAinda não há avaliações
- Chest Trauma: Annet Mary Mathew Anu Krishna Arathi.KDocumento60 páginasChest Trauma: Annet Mary Mathew Anu Krishna Arathi.KAsif AbbasAinda não há avaliações
- Emergency Medicine كتاب ايمرجنسي مفيد للروتيترز الجدد وملخص مفيدDocumento46 páginasEmergency Medicine كتاب ايمرجنسي مفيد للروتيترز الجدد وملخص مفيدSri PoopaseAinda não há avaliações
- ATLSDocumento92 páginasATLSRendi MuflihAinda não há avaliações
- Emergency Medical Care For Trauma at The Pre-Hospital StageDocumento125 páginasEmergency Medical Care For Trauma at The Pre-Hospital StageAkash KumarAinda não há avaliações
- IntroductionDocumento5 páginasIntroductionFarhan YulmiadiAinda não há avaliações
- ATLSDocumento42 páginasATLSAlessandro MuderevuAinda não há avaliações
- Maxilofacial Trauma: Presenter: - Wisnu Adiputra (07120080072) - Nofilia Citra Candra (07120090066)Documento97 páginasMaxilofacial Trauma: Presenter: - Wisnu Adiputra (07120080072) - Nofilia Citra Candra (07120090066)Nofilia Citra CandraAinda não há avaliações
- Trauma and AneurysmDocumento5 páginasTrauma and AneurysmOmar Khalif Amad Pendatun100% (1)
- Trauma Overview: Mark E. Armstrong, M.DDocumento49 páginasTrauma Overview: Mark E. Armstrong, M.DTimothy OneilAinda não há avaliações
- Primary and Secondary SurveyDocumento14 páginasPrimary and Secondary SurveyUma SankarAinda não há avaliações
- Ottawa Handbook of Emergency Medicine 5th EditionDocumento70 páginasOttawa Handbook of Emergency Medicine 5th EditionBilalAinda não há avaliações
- Pulmonary EmbolismDocumento19 páginasPulmonary EmbolismIbrahimAinda não há avaliações
- Medical and Surgical Emergencies Karen BallDocumento62 páginasMedical and Surgical Emergencies Karen Ballapi-195799092Ainda não há avaliações
- Introduction To Trauma: LSU Medical Student Clerkship, New Orleans, LADocumento31 páginasIntroduction To Trauma: LSU Medical Student Clerkship, New Orleans, LAnandangAinda não há avaliações
- Penetrating Abdominal TraumaDocumento67 páginasPenetrating Abdominal TraumarizkaAinda não há avaliações
- ATLS - Initial AssessmentDocumento6 páginasATLS - Initial AssessmentJessie E. Gee93% (14)
- Primary and Secondary SurveyDocumento10 páginasPrimary and Secondary SurveyBernadeth Meily100% (1)
- Abdominal TraumaDocumento66 páginasAbdominal Traumaofficial.drjainAinda não há avaliações
- Emergency Airway Management: Pat Melanson, MDDocumento47 páginasEmergency Airway Management: Pat Melanson, MDFarida IntanAinda não há avaliações
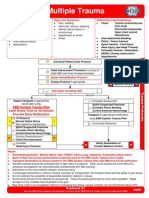
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDocumento1 páginaMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonAinda não há avaliações
- Multiple Trauma ManagementDocumento1 páginaMultiple Trauma ManagementSetiawan Arif WibowoAinda não há avaliações
- EN Primary SurveyDocumento32 páginasEN Primary SurveythoriqAinda não há avaliações
- Laryngeal: Obstruction Relieved by PantingDocumento3 páginasLaryngeal: Obstruction Relieved by PantingIndah D. RahmahAinda não há avaliações
- Emergency MedicineDocumento46 páginasEmergency MedicinekararobeedAinda não há avaliações
- Ottawas Clerkship GuideDocumento44 páginasOttawas Clerkship GuideHugo LuceroAinda não há avaliações
- Initial Assessment and ManagementDocumento8 páginasInitial Assessment and ManagementAlvin De LunaAinda não há avaliações
- Trauma ZaiTDocumento5 páginasTrauma ZaiTmolhamgaaferAinda não há avaliações
- Immediate Life Support - NewDocumento67 páginasImmediate Life Support - NewTalhaAinda não há avaliações
- امتحان مهم كاردياك سيرجاريDocumento15 páginasامتحان مهم كاردياك سيرجاريIbrahim Barham50% (2)
- Basic TraumaDocumento33 páginasBasic TraumaErna SallyAinda não há avaliações
- Redbook - ASSESSMENT AND MANAGEMENT OF TRAUMA PDFDocumento323 páginasRedbook - ASSESSMENT AND MANAGEMENT OF TRAUMA PDFrizka100% (1)
- Primary SurveyDocumento34 páginasPrimary SurveyTausif HaqueAinda não há avaliações
- Emergency Point-of-Care UltrasoundNo EverandEmergency Point-of-Care UltrasoundJames A. ConnollyAinda não há avaliações
- Monitoring Mechanical Ventilation Using Ventilator WaveformsNo EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsAinda não há avaliações
- Atlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosNo EverandAtlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosAinda não há avaliações
- Is 13779 1999 PDFDocumento46 páginasIs 13779 1999 PDFchandranmuthuswamyAinda não há avaliações
- Brochure - Digital Banking - New DelhiDocumento4 páginasBrochure - Digital Banking - New Delhiankitgarg13Ainda não há avaliações
- Conversation Between God and LuciferDocumento3 páginasConversation Between God and LuciferRiddhi ShahAinda não há avaliações
- 19 Amazing Benefits of Fennel Seeds For SkinDocumento9 páginas19 Amazing Benefits of Fennel Seeds For SkinnasimAinda não há avaliações
- Final Presentation BANK OF BARODA 1Documento8 páginasFinal Presentation BANK OF BARODA 1Pooja GoyalAinda não há avaliações
- Annexure 8: Medical Certificate (To Be Issued by A Registered Medical Practitioner) General ExpectationsDocumento1 páginaAnnexure 8: Medical Certificate (To Be Issued by A Registered Medical Practitioner) General ExpectationsMannepalli RamakrishnaAinda não há avaliações
- Public International Law Green Notes 2015Documento34 páginasPublic International Law Green Notes 2015KrisLarr100% (1)
- (Dan Stone) The Historiography of The HolocaustDocumento586 páginas(Dan Stone) The Historiography of The HolocaustPop Catalin100% (1)
- Contents Serbo-Croatian GrammarDocumento2 páginasContents Serbo-Croatian GrammarLeo VasilaAinda não há avaliações
- Lesson Plan Pumpkin Moon SandDocumento3 páginasLesson Plan Pumpkin Moon Sandapi-273177086Ainda não há avaliações
- British Citizenship Exam Review TestDocumento25 páginasBritish Citizenship Exam Review TestMay J. PabloAinda não há avaliações
- Hercules Industries Inc. v. Secretary of Labor (1992)Documento1 páginaHercules Industries Inc. v. Secretary of Labor (1992)Vianca MiguelAinda não há avaliações
- Lista Verbelor Regulate - EnglezaDocumento5 páginasLista Verbelor Regulate - Englezaflopalan100% (1)
- GRADE 1 To 12 Daily Lesson LOG: TLE6AG-Oc-3-1.3.3Documento7 páginasGRADE 1 To 12 Daily Lesson LOG: TLE6AG-Oc-3-1.3.3Roxanne Pia FlorentinoAinda não há avaliações
- Finding The NTH Term of An Arithmetic SequenceDocumento3 páginasFinding The NTH Term of An Arithmetic SequenceArdy PatawaranAinda não há avaliações
- Childbirth Self-Efficacy Inventory and Childbirth Attitudes Questionner Thai LanguageDocumento11 páginasChildbirth Self-Efficacy Inventory and Childbirth Attitudes Questionner Thai LanguageWenny Indah Purnama Eka SariAinda não há avaliações
- Prepositions French Worksheet For PracticeDocumento37 páginasPrepositions French Worksheet For Practiceangelamonteiro100% (1)
- Oxford Reading Circle tg-4 2nd EditionDocumento92 páginasOxford Reading Circle tg-4 2nd EditionAreeb Siddiqui89% (9)
- Java ReviewDocumento68 páginasJava ReviewMyco BelvestreAinda não há avaliações
- Reith 2020 Lecture 1 TranscriptDocumento16 páginasReith 2020 Lecture 1 TranscriptHuy BuiAinda não há avaliações
- Diploma Pendidikan Awal Kanak-Kanak: Diploma in Early Childhood EducationDocumento8 páginasDiploma Pendidikan Awal Kanak-Kanak: Diploma in Early Childhood Educationsiti aisyahAinda não há avaliações
- Calendar of Cases (May 3, 2018)Documento4 páginasCalendar of Cases (May 3, 2018)Roy BacaniAinda não há avaliações
- Bakhtin's Chronotope On The RoadDocumento17 páginasBakhtin's Chronotope On The RoadLeandro OliveiraAinda não há avaliações
- Joshua 24 15Documento1 páginaJoshua 24 15api-313783690Ainda não há avaliações
- Fundamental Rights-Right To Equality, Prohibition of Discrimination, Right To Equality of OpportunityDocumento76 páginasFundamental Rights-Right To Equality, Prohibition of Discrimination, Right To Equality of OpportunityutkarshAinda não há avaliações
- Reflection On Harrison Bergeron Society. 21ST CenturyDocumento3 páginasReflection On Harrison Bergeron Society. 21ST CenturyKim Alleah Delas LlagasAinda não há avaliações
- Gandhi Was A British Agent and Brought From SA by British To Sabotage IndiaDocumento6 páginasGandhi Was A British Agent and Brought From SA by British To Sabotage Indiakushalmehra100% (2)
- Mathematics: Quarter 3 - Module 6Documento15 páginasMathematics: Quarter 3 - Module 6Ray Phillip G. Jorduela0% (1)
- SUBSET-026-7 v230 - 060224Documento62 páginasSUBSET-026-7 v230 - 060224David WoodhouseAinda não há avaliações
- Viva QuestionsDocumento3 páginasViva QuestionssanjayshekarncAinda não há avaliações