Você também pode gostar
- Adaps With Current or Anticipated Cost-Containment Measures, Including Waiting Lists, August 2012Documento4 páginasAdaps With Current or Anticipated Cost-Containment Measures, Including Waiting Lists, August 2012housingworksAinda não há avaliações
- ADAP Watch Update - 7.16.12Documento2 páginasADAP Watch Update - 7.16.12housingworksAinda não há avaliações
- ADAP Watch Update - 4.30.12Documento2 páginasADAP Watch Update - 4.30.12housingworksAinda não há avaliações
- Adap 9.14Documento2 páginasAdap 9.14housingworksAinda não há avaliações
- ADAP Watch Update - 5.4.12Documento2 páginasADAP Watch Update - 5.4.12housingworksAinda não há avaliações
- ADAP Watch December 17Documento3 páginasADAP Watch December 17housingworksAinda não há avaliações
- August 6Documento2 páginasAugust 6housingworksAinda não há avaliações
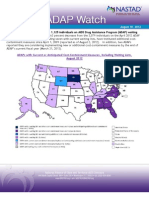
- Adaps With Waiting Lists (694 Individuals in 7 States, As of August 16, 2012)Documento2 páginasAdaps With Waiting Lists (694 Individuals in 7 States, As of August 16, 2012)anne_berk_1Ainda não há avaliações
- ADAP Watch Update - 2.17.12Documento2 páginasADAP Watch Update - 2.17.12housingworksAinda não há avaliações
- ADAP Watch Update - 4.6.12Documento2 páginasADAP Watch Update - 4.6.12housingworksAinda não há avaliações
- ADAP Watch Update - 3.2.12Documento2 páginasADAP Watch Update - 3.2.12housingworksAinda não há avaliações
- ADAP Watch Update - 2.3.12Documento2 páginasADAP Watch Update - 2.3.12housingworksAinda não há avaliações
- ADAP Watch 5.28.13Documento1 páginaADAP Watch 5.28.13anne_berk_1Ainda não há avaliações
- ADAP Watch Update - 12.2.11Documento2 páginasADAP Watch Update - 12.2.11housingworksAinda não há avaliações
- ADAP Jan 2013Documento2 páginasADAP Jan 2013housingworksAinda não há avaliações
- ADAP Watch Update - 8.18.11Documento2 páginasADAP Watch Update - 8.18.11housingworksAinda não há avaliações
- ADAP Watch Update - 8.5.11Documento2 páginasADAP Watch Update - 8.5.11housingworksAinda não há avaliações
- Adap Watch 4.15.13Documento1 páginaAdap Watch 4.15.13housingworksAinda não há avaliações
- ADAP Watch Update - 7.29.11Documento2 páginasADAP Watch Update - 7.29.11housingworksAinda não há avaliações
- ADAP Watch Update - 7.1.11Documento2 páginasADAP Watch Update - 7.1.11housingworksAinda não há avaliações
- ADAP Watch Update - 9.1.11Documento2 páginasADAP Watch Update - 9.1.11housingworksAinda não há avaliações
- NASTADADAPWatch June2010Documento2 páginasNASTADADAPWatch June2010api-24494082Ainda não há avaliações
- ADAP Watch - 2.11.11Documento2 páginasADAP Watch - 2.11.11housingworksAinda não há avaliações
- ADAP Watch Update - 11.4.11Documento2 páginasADAP Watch Update - 11.4.11housingworksAinda não há avaliações
- ADAP Watch Update - 10.7.11Documento2 páginasADAP Watch Update - 10.7.11housingworksAinda não há avaliações
- Adap Watch - 4.22.11Documento2 páginasAdap Watch - 4.22.11housingworksAinda não há avaliações
- ADAP Watch Update - 5.6.11Documento2 páginasADAP Watch Update - 5.6.11housingworksAinda não há avaliações
- ADAP Watch Update - 6.2.11Documento2 páginasADAP Watch Update - 6.2.11housingworksAinda não há avaliações
- Summative Health Policy CapstoneDocumento15 páginasSummative Health Policy Capstoneapi-354621238Ainda não há avaliações
- Ohio MCPDocumento4 páginasOhio MCPseppun1Ainda não há avaliações
- Literature Review DialysisDocumento14 páginasLiterature Review DialysisAnneAinda não há avaliações
- Medicare-Medicaid Enrollee State ProfileDocumento11 páginasMedicare-Medicaid Enrollee State ProfileJames LindonAinda não há avaliações
- SHADAC Brief 43: ChurningDocumento8 páginasSHADAC Brief 43: ChurningSHADACAinda não há avaliações
- A Primer On Medicaid and Its Expansion in 2014Documento2 páginasA Primer On Medicaid and Its Expansion in 2014Kiana TehraniAinda não há avaliações
- StateProgramsReform REPORTDocumento59 páginasStateProgramsReform REPORTkirs0069Ainda não há avaliações
- Payers & Providers National Edition - Issue of February 2012Documento8 páginasPayers & Providers National Edition - Issue of February 2012PayersandProvidersAinda não há avaliações
- State Medicaid Program Issues: Preferred Drug Lists, 2003Documento8 páginasState Medicaid Program Issues: Preferred Drug Lists, 2003National Pharmaceutical CouncilAinda não há avaliações
- StateDataSpotlight RI Jan2012Documento3 páginasStateDataSpotlight RI Jan2012SHADACAinda não há avaliações
- Amputations Attributed To DiabetesDocumento17 páginasAmputations Attributed To Diabetesapi-418237167Ainda não há avaliações
- Policy PaperDocumento22 páginasPolicy Paperapi-412575008Ainda não há avaliações
- 2002 GAO PDMP StudyDocumento27 páginas2002 GAO PDMP StudyKOMU NewsAinda não há avaliações
- Portion Medical Primary Care Health CentersDocumento21 páginasPortion Medical Primary Care Health CenterssdardaAinda não há avaliações
- Your Guide to Health Care and Food Benefits in WisconsinDocumento56 páginasYour Guide to Health Care and Food Benefits in Wisconsinesesmith108Ainda não há avaliações
- Hooker Nicholson Journal ArticleDocumento11 páginasHooker Nicholson Journal ArticleJeff Nicholson PhD, PA-CAinda não há avaliações
- Disease Management Reduce CostDocumento13 páginasDisease Management Reduce CostSaleem RajabiAinda não há avaliações
- Probing Addiction Treatment During An Opioid EpidemicDocumento2 páginasProbing Addiction Treatment During An Opioid EpidemicABC News PoliticsAinda não há avaliações
- NutritionDocumento44 páginasNutritionapi-240122097Ainda não há avaliações
- Dallas County Community Health DashboardDocumento41 páginasDallas County Community Health DashboardTed HillAinda não há avaliações
- ACA Presentation For Community Forum Dec 10 2013Documento61 páginasACA Presentation For Community Forum Dec 10 2013Todd GroveAinda não há avaliações
- Oregon Health Care Delivery Systems ReportDocumento14 páginasOregon Health Care Delivery Systems ReportfrendirachmadAinda não há avaliações
- 10 Letters From State Medicaid ProgramsDocumento28 páginas10 Letters From State Medicaid ProgramsSHFWireAinda não há avaliações
- CHV20 Unit 2 CulminatingDocumento9 páginasCHV20 Unit 2 Culminatingtongeaiden1Ainda não há avaliações
- USHC ReviewDocumento119 páginasUSHC ReviewArman DhillonAinda não há avaliações
- State Efforts To Combat OpioidsDocumento62 páginasState Efforts To Combat OpioidsNational Press FoundationAinda não há avaliações
- Yu 2020Documento9 páginasYu 2020Epigmenio Díaz CruzAinda não há avaliações
- Approved State Plans Section 2703 Health HomesDocumento35 páginasApproved State Plans Section 2703 Health HomesiggybauAinda não há avaliações
- Understanding and Addressing "Hot Spots" Critical To Bending The Medicaid Cost CurveDocumento8 páginasUnderstanding and Addressing "Hot Spots" Critical To Bending The Medicaid Cost CurvePartnership to Fight Chronic DiseaseAinda não há avaliações
- 2020 08 22 20179903v1 Full PDFDocumento17 páginas2020 08 22 20179903v1 Full PDFJuensAinda não há avaliações
- Running Head: MILESTONE # 4 1Documento9 páginasRunning Head: MILESTONE # 4 1Corie SpadaroAinda não há avaliações
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNo EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsAinda não há avaliações
- Housing Works "What's Your Voting Plan?!" Sheet 2018Documento1 páginaHousing Works "What's Your Voting Plan?!" Sheet 2018housingworksAinda não há avaliações
- Housing Works Get Out The Vote, Election Day 2018 Fact SheetDocumento1 páginaHousing Works Get Out The Vote, Election Day 2018 Fact SheethousingworksAinda não há avaliações
- End AIDS NY 2020 Coalition, World AIDS Day 2018 Resources ListingDocumento3 páginasEnd AIDS NY 2020 Coalition, World AIDS Day 2018 Resources ListinghousingworksAinda não há avaliações
- NYC LGBT Solidarity Rally Flyer For 2 4 17 ExternalDocumento1 páginaNYC LGBT Solidarity Rally Flyer For 2 4 17 ExternalhousingworksAinda não há avaliações
- New York State Ending The AIDS Epidemic Blueprint Summary One-SheetDocumento2 páginasNew York State Ending The AIDS Epidemic Blueprint Summary One-SheethousingworksAinda não há avaliações
- Housing Works Get Out The Vote Election Day 2017Documento1 páginaHousing Works Get Out The Vote Election Day 2017housingworksAinda não há avaliações
- 2018 NYC LGBT March Route MapDocumento1 página2018 NYC LGBT March Route MaphousingworksAinda não há avaliações
- Housing Works April 2017 Town Hall Call-to-ActionDocumento2 páginasHousing Works April 2017 Town Hall Call-to-ActionhousingworksAinda não há avaliações
- NYC World AIDS Day 2015 Coalition Event SaveTheDate Flyer EnglishDocumento1 páginaNYC World AIDS Day 2015 Coalition Event SaveTheDate Flyer EnglishhousingworksAinda não há avaliações
- May 2016 AIDS Advocates Consensus Policy Paper W EndorsersDocumento17 páginasMay 2016 AIDS Advocates Consensus Policy Paper W EndorsershousingworksAinda não há avaliações
- Civil Society and Communities Declaration To End HIV: Human Rights Must Come FirstDocumento7 páginasCivil Society and Communities Declaration To End HIV: Human Rights Must Come FirsthousingworksAinda não há avaliações
- AIDS - Free USA 2025 Indiv Sign-On Petition For 2016 Prez Candidates (Download Copy)Documento2 páginasAIDS - Free USA 2025 Indiv Sign-On Petition For 2016 Prez Candidates (Download Copy)housingworksAinda não há avaliações
- Hillary Clinton Agenda and Meeting Notes 5.12.16Documento9 páginasHillary Clinton Agenda and Meeting Notes 5.12.16Housing WorksAinda não há avaliações
- DOHMH Notes On Gov Exec Budget, 2.8.17Documento2 páginasDOHMH Notes On Gov Exec Budget, 2.8.17housingworksAinda não há avaliações
- Nigerian LGBTers Invite To 1/12/15 Veil of Silence Doc ScreeningDocumento1 páginaNigerian LGBTers Invite To 1/12/15 Veil of Silence Doc ScreeninghousingworksAinda não há avaliações
- NY State Trans Healthcare Regulation Dec. 2014Documento4 páginasNY State Trans Healthcare Regulation Dec. 2014housingworksAinda não há avaliações
- Task Force End of AIDS NYS, Opening Remarks, 10.14.14, CKingDocumento3 páginasTask Force End of AIDS NYS, Opening Remarks, 10.14.14, CKinghousingworksAinda não há avaliações
- 2014 IBJ JusticeMakers Award Applications LetterDocumento2 páginas2014 IBJ JusticeMakers Award Applications LetterhousingworksAinda não há avaliações
- NYC World AIDS Day Coalition Program, 12-1-14, Harlem's World Famous ApolloDocumento4 páginasNYC World AIDS Day Coalition Program, 12-1-14, Harlem's World Famous ApollohousingworksAinda não há avaliações
- Housing Works World AIDS Day 2014 CoalitionEvent FlyerSaveTheDate, EnglishDocumento1 páginaHousing Works World AIDS Day 2014 CoalitionEvent FlyerSaveTheDate, EnglishhousingworksAinda não há avaliações
- O'Connell and Feldman - Manhattan ONAP Presentation 8.7.14Documento9 páginasO'Connell and Feldman - Manhattan ONAP Presentation 8.7.14housingworksAinda não há avaliações
- Housing Works Trans Day of Rememberance 2014 Event FlyerDocumento1 páginaHousing Works Trans Day of Rememberance 2014 Event FlyerhousingworksAinda não há avaliações
- Media Advisory 10.27 AIDS Community Press Conf RE Cuomo Ebola Quarantine FINALDocumento1 páginaMedia Advisory 10.27 AIDS Community Press Conf RE Cuomo Ebola Quarantine FINALhousingworksAinda não há avaliações
- #ICantBreathe/ Dec. 2014-Jan. 2015 Calls-to-Action Flyer, Housing Works Advocacy ActionsDocumento2 páginas#ICantBreathe/ Dec. 2014-Jan. 2015 Calls-to-Action Flyer, Housing Works Advocacy ActionshousingworksAinda não há avaliações
- Housing Works World AIDS Day 2014 CoalitionEvent FlyerSaveTheDate, SpanishDocumento1 páginaHousing Works World AIDS Day 2014 CoalitionEvent FlyerSaveTheDate, SpanishhousingworksAinda não há avaliações
- Undetectables Project September 2014 2Documento11 páginasUndetectables Project September 2014 2housingworksAinda não há avaliações
- Harrison - Brooklyn ONAP Presentation 8.8.14Documento15 páginasHarrison - Brooklyn ONAP Presentation 8.8.14housingworksAinda não há avaliações
- Harrison - Brooklyn ONAP Presentation 8.8.14Documento15 páginasHarrison - Brooklyn ONAP Presentation 8.8.14housingworksAinda não há avaliações
- Quarantine - Leadership Letter FINAL 10 26 14Documento6 páginasQuarantine - Leadership Letter FINAL 10 26 14housingworksAinda não há avaliações
- Braking AIDS Ride 2014. 9/12-9/14, Cheering Stations GuideDocumento1 páginaBraking AIDS Ride 2014. 9/12-9/14, Cheering Stations GuidehousingworksAinda não há avaliações
- Medical Mnemonics 4 PrintDocumento65 páginasMedical Mnemonics 4 Printanne0521100% (1)
- Parameters of Mechanics of BreathingDocumento16 páginasParameters of Mechanics of BreathingKaioAinda não há avaliações
- CAP Protocol-2016 Thyroid - HighlightedDocumento8 páginasCAP Protocol-2016 Thyroid - Highlightedpath2016Ainda não há avaliações
- Soal SBMPTN 2018 - Bahasa Inggris Paket 2Documento5 páginasSoal SBMPTN 2018 - Bahasa Inggris Paket 2Sholihin IkhwanAinda não há avaliações
- PDFDocumento70 páginasPDFPaul Benjomin AgregadoAinda não há avaliações
- Journal of Ethnopharmacology: Shashank Tiwari, Sandeep Kumar Gupta, Anklesh Kumar PathakDocumento8 páginasJournal of Ethnopharmacology: Shashank Tiwari, Sandeep Kumar Gupta, Anklesh Kumar PathakMichael Kohlberger, BSc MScAinda não há avaliações
- Solution Manual For The Basic Practice of Statistics 8th Edition David S MooreDocumento13 páginasSolution Manual For The Basic Practice of Statistics 8th Edition David S MooreAudreyRayqowjd100% (77)
- Practice Questions For Hepatic Disorders - NURS 1028 Nursing TheoryDocumento2 páginasPractice Questions For Hepatic Disorders - NURS 1028 Nursing TheoryNicholas ObasiAinda não há avaliações
- FNCPDocumento2 páginasFNCPIrish MejiaAinda não há avaliações
- MaqasidDocumento5 páginasMaqasidDidi FirdausAinda não há avaliações
- KAP Anthrax and Animal Care A Case-Control StudyDocumento11 páginasKAP Anthrax and Animal Care A Case-Control StudyAsmi AsmuAinda não há avaliações
- Elbow Joint ConditionsDocumento3 páginasElbow Joint ConditionsMarilia FarensenaAinda não há avaliações
- Ave Lox TabsDocumento5 páginasAve Lox Tabslrdn_ghrcAinda não há avaliações
- Diabetic KetoacidosisDocumento7 páginasDiabetic KetoacidosisetengAinda não há avaliações
- Perspective: New England Journal MedicineDocumento3 páginasPerspective: New England Journal MedicineEmanuel LayonAinda não há avaliações
- BQ - Medical Writing Assignment-1Documento1 páginaBQ - Medical Writing Assignment-1Sumeet GurnaniAinda não há avaliações
- Camca Prelim Reviewer 2Documento11 páginasCamca Prelim Reviewer 2Danna MedranaAinda não há avaliações
- Blood Agar Base (Infusion Agar) : Intended Use Summary and ExplanationDocumento2 páginasBlood Agar Base (Infusion Agar) : Intended Use Summary and ExplanationSarehElizabetAinda não há avaliações
- Medical Surgical NursingDocumento38 páginasMedical Surgical NursingTripti PunAinda não há avaliações
- Essay On AidsDocumento6 páginasEssay On AidsBharat SinghAinda não há avaliações
- Critical Events in the COVID-19 Timeline in the PhilippinesDocumento3 páginasCritical Events in the COVID-19 Timeline in the PhilippinesChris Wilfred Estrada100% (5)
- Deciduous Forest BiomeDocumento22 páginasDeciduous Forest BiomeArlanosaurus100% (2)
- Preventing Mosquito BitesDocumento1 páginaPreventing Mosquito BitesmkumAinda não há avaliações
- A Global Resource For Genomic Predictions of Antimicrobial Resistance and Surveillance of Salmonella Typhi at PathogenwatchDocumento12 páginasA Global Resource For Genomic Predictions of Antimicrobial Resistance and Surveillance of Salmonella Typhi at PathogenwatchOkeke UcheeAinda não há avaliações
- The Neuro Metabolic Summit - TranscriptsDocumento35 páginasThe Neuro Metabolic Summit - TranscriptsIONUT GRIGOROVAinda não há avaliações
- Economic Analysis of Cucumber ProductionDocumento20 páginasEconomic Analysis of Cucumber ProductionMajesty100% (1)
- Narrative TextDocumento20 páginasNarrative Textdika grayAinda não há avaliações
- Insoluble Ions EssayDocumento2 páginasInsoluble Ions EssayDarshan Meghji100% (1)
- Integrated Cardiovascular Physiology: A Laboratory ExerciseDocumento70 páginasIntegrated Cardiovascular Physiology: A Laboratory ExercisefireworkrwAinda não há avaliações
- Rpms Lesson PlanDocumento6 páginasRpms Lesson PlanEric John VegafriaAinda não há avaliações