Você também pode gostar
- Mortal Kombat XDocumento24 páginasMortal Kombat XMindSpaceApocalypseAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Session 2 - 01 (Energy Efficiency Potential Assessment of Chandrapura TPS, DVC)Documento52 páginasSession 2 - 01 (Energy Efficiency Potential Assessment of Chandrapura TPS, DVC)pkumarAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Apples-to-Apples in Cross-Validation Studies: Pitfalls in Classifier Performance MeasurementDocumento9 páginasApples-to-Apples in Cross-Validation Studies: Pitfalls in Classifier Performance MeasurementLuis Martínez RamírezAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Ems Accounting Term 2Documento39 páginasEms Accounting Term 2Paballo KoopediAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Metric MIL-STD-1504C (USAF) 01 March 2007 Supersedes MIL-STD-1504B 8 June 1989Documento11 páginasMetric MIL-STD-1504C (USAF) 01 March 2007 Supersedes MIL-STD-1504B 8 June 1989HenryAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Boarding PassDocumento1 páginaBoarding PassFajarAinda não há avaliações
- Ansi MV Techtopics75 enDocumento2 páginasAnsi MV Techtopics75 enjobpei2Ainda não há avaliações
- Adaptation Fom Squirrels GamesDocumento2 páginasAdaptation Fom Squirrels GamesDenny Boy MochranAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Depreciation Is A Term Used Reference To TheDocumento14 páginasDepreciation Is A Term Used Reference To TheMuzammil IqbalAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Business PlanDocumento11 páginasBusiness PlanIsaac ManarinAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- AttitudeDocumento24 páginasAttitudeisratazimAinda não há avaliações
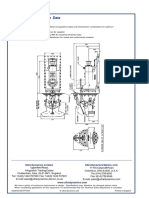
- Ultrajet 376 Installation Data: Ultra Dynamics Marine, LCC Ultra Dynamics LimitedDocumento2 páginasUltrajet 376 Installation Data: Ultra Dynamics Marine, LCC Ultra Dynamics LimitedhaujesAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Process and Inter-Process Systems For All Industries.: Cleaning Validation: An Overall PerspectiveDocumento7 páginasProcess and Inter-Process Systems For All Industries.: Cleaning Validation: An Overall PerspectiveDesarrollo de Colecciones IVIC-BMRAinda não há avaliações
- OS Lab ManualDocumento37 páginasOS Lab ManualVenkatanagasudheer ThummapudiAinda não há avaliações
- Talk - Data Quality FrameworkDocumento30 páginasTalk - Data Quality FrameworkMatthew LawlerAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Virtual Asset Insurance Risk Analysis - OneDegreeDocumento3 páginasVirtual Asset Insurance Risk Analysis - OneDegreeShaarang BeganiAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- A Flight Plan in 10 StepsDocumento4 páginasA Flight Plan in 10 StepsThar LattAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Top 50 World Pharma 2001Documento11 páginasTop 50 World Pharma 2001Juraj KubáňAinda não há avaliações
- Revised Procedural Manual On Hazardous Waste Management (Revised DAO 04-36) I CONTENTS Chapter Page PDFDocumento53 páginasRevised Procedural Manual On Hazardous Waste Management (Revised DAO 04-36) I CONTENTS Chapter Page PDFdennisAinda não há avaliações
- WabimalunoxowevefoDocumento3 páginasWabimalunoxowevefoChitmin KhantAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Reemployment Assistance Application EngDocumento6 páginasReemployment Assistance Application EngMelissa RatliffAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Teit Cbgs Dmbi Lab Manual FH 2015Documento60 páginasTeit Cbgs Dmbi Lab Manual FH 2015Soumya PandeyAinda não há avaliações
- Autodesk Inventor Practice Part DrawingsDocumento25 páginasAutodesk Inventor Practice Part DrawingsCiprian Fratila100% (1)
- HYD CCU: TICKET - ConfirmedDocumento2 páginasHYD CCU: TICKET - ConfirmedRahul ValapadasuAinda não há avaliações
- 3-DatAdvantage Advanced Installation For NAS and Linux Platforms 8.6Documento47 páginas3-DatAdvantage Advanced Installation For NAS and Linux Platforms 8.6yaritzaAinda não há avaliações
- Bonus 6 - Mastering ASP - NET Core SecurityDocumento147 páginasBonus 6 - Mastering ASP - NET Core SecurityDark Shadow100% (1)
- Natural Gas ENgineering - Jann Rune Ursin PDFDocumento361 páginasNatural Gas ENgineering - Jann Rune Ursin PDFDanitza Pamela Quisbert100% (1)
- SCADA Generic Risk Management FrameworkDocumento49 páginasSCADA Generic Risk Management FrameworkAnak PohonAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Saraswathi 2018Documento4 páginasSaraswathi 2018Daniel CoronelAinda não há avaliações
- Test Help StatDocumento18 páginasTest Help Statthenderson22603Ainda não há avaliações