Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Anatomy of Research Scandals, by Carl ElliottDocumento1 páginaAnatomy of Research Scandals, by Carl ElliottMarkingsonCaseAinda não há avaliações
- The Plutonium Experiments: Fred SoursDocumento3 páginasThe Plutonium Experiments: Fred SoursMarkingsonCase100% (2)
- Condemned To Die For Science by Jack SlaterDocumento9 páginasCondemned To Die For Science by Jack SlaterMarkingsonCaseAinda não há avaliações
- A Comprehensive Update On Treatment of Dementia-2019Documento12 páginasA Comprehensive Update On Treatment of Dementia-2019Juan Paredes100% (1)
- Understanding Bipolar DisorderDocumento24 páginasUnderstanding Bipolar DisorderdoscribeAinda não há avaliações
- MH NotesDocumento28 páginasMH NotesNyein Nu Winn100% (2)
- Request For A Statue Honoring Civil Rights Leader Joseph A. de LaineDocumento3 páginasRequest For A Statue Honoring Civil Rights Leader Joseph A. de LaineMarkingsonCase100% (1)
- Request To Adrienne Baranauskas of Fairview To Investigate Conflicts of Interest Regarding David Adson in CAFE and CATIE StudiesDocumento3 páginasRequest To Adrienne Baranauskas of Fairview To Investigate Conflicts of Interest Regarding David Adson in CAFE and CATIE StudiesCarl ElliottAinda não há avaliações
- Using Poor, Uninsured Minorities To Test The Safety of Experimental DrugsDocumento4 páginasUsing Poor, Uninsured Minorities To Test The Safety of Experimental DrugsMarkingsonCaseAinda não há avaliações
- OHRP Response To Complaint About David Adson and IRB Oversight at University of MinnesotaDocumento3 páginasOHRP Response To Complaint About David Adson and IRB Oversight at University of MinnesotaMarkingsonCaseAinda não há avaliações
- Elyse Summers AAHRPP Email To Carl Elliott May 5 2014Documento1 páginaElyse Summers AAHRPP Email To Carl Elliott May 5 2014MarkingsonCaseAinda não há avaliações
- Involuntarily Committed Patients As Prisoners, Matt Lamkin and Carl Elliott, University of Richmond Law ReviewDocumento54 páginasInvoluntarily Committed Patients As Prisoners, Matt Lamkin and Carl Elliott, University of Richmond Law ReviewMarkingsonCaseAinda não há avaliações
- Institutional Pathology and The Death of Dan MarkingsonDocumento16 páginasInstitutional Pathology and The Death of Dan MarkingsonMarkingsonCaseAinda não há avaliações
- The Plutonium Experiments: Albert StevensDocumento10 páginasThe Plutonium Experiments: Albert StevensMarkingsonCaseAinda não há avaliações
- David Adson Pharmaceutical Industry Payments 2002-2010Documento12 páginasDavid Adson Pharmaceutical Industry Payments 2002-2010MarkingsonCaseAinda não há avaliações
- David Adson CVDocumento9 páginasDavid Adson CVMarkingsonCaseAinda não há avaliações
- Request To Adrienne Baranauskas of Fairview To Investigate Conflicts of Interest Regarding David Adson in CAFE and CATIE StudiesDocumento3 páginasRequest To Adrienne Baranauskas of Fairview To Investigate Conflicts of Interest Regarding David Adson in CAFE and CATIE StudiesCarl ElliottAinda não há avaliações
- The Plutonium Experiments: John MoussonDocumento4 páginasThe Plutonium Experiments: John MoussonMarkingsonCaseAinda não há avaliações
- Pamela Webb Research Compliance Office Response To Carl Elliott Regarding Robert Huber and Bifeprunox StudyDocumento2 páginasPamela Webb Research Compliance Office Response To Carl Elliott Regarding Robert Huber and Bifeprunox StudyMarkingsonCaseAinda não há avaliações
- FTI Consulting Report On Robert Huber CaseDocumento23 páginasFTI Consulting Report On Robert Huber CaseMarkingsonCaseAinda não há avaliações
- The Plutonium Experiments: Eda CharltonDocumento8 páginasThe Plutonium Experiments: Eda CharltonMarkingsonCaseAinda não há avaliações
- The Plutonium Experiments: Clyde AllenDocumento14 páginasThe Plutonium Experiments: Clyde AllenMarkingsonCaseAinda não há avaliações
- Letter From University of Minnesota Attorney Lori Ketola Regarding Release of Confidential Patient InformationDocumento2 páginasLetter From University of Minnesota Attorney Lori Ketola Regarding Release of Confidential Patient InformationMarkingsonCaseAinda não há avaliações
- Elyse Summers AAHRPP Email To Carl Elliott May 5 2014Documento1 páginaElyse Summers AAHRPP Email To Carl Elliott May 5 2014MarkingsonCaseAinda não há avaliações
- Faculty Consultative Committee of The University of Minnesota, Minutes of The Meeting of March 16 2016Documento9 páginasFaculty Consultative Committee of The University of Minnesota, Minutes of The Meeting of March 16 2016MarkingsonCaseAinda não há avaliações
- Signatories To "University of Minnesota Research Lapses Show Self-Reform Is Failing," Minneapolis Star Tribune, February 18, 2016Documento5 páginasSignatories To "University of Minnesota Research Lapses Show Self-Reform Is Failing," Minneapolis Star Tribune, February 18, 2016MarkingsonCaseAinda não há avaliações
- Whatever Happened To Human Experimentation?Documento4 páginasWhatever Happened To Human Experimentation?MarkingsonCaseAinda não há avaliações
- October 5, 2015 Letter To Senator Terri BonoffDocumento2 páginasOctober 5, 2015 Letter To Senator Terri BonoffBill GleasonAinda não há avaliações
- Pamela Webb Research Compliance Office Response To Carl Elliott Regarding Robert Huber and Bifeprunox StudyDocumento2 páginasPamela Webb Research Compliance Office Response To Carl Elliott Regarding Robert Huber and Bifeprunox StudyMarkingsonCaseAinda não há avaliações
- Traci Johnson Cymbalta SuicideDocumento10 páginasTraci Johnson Cymbalta SuicideMarkingsonCaseAinda não há avaliações
- Letter From Leigh Turner To Senator Terri Bonoff October 19 2015Documento3 páginasLetter From Leigh Turner To Senator Terri Bonoff October 19 2015MarkingsonCaseAinda não há avaliações
- Email From Sen. Terri Bonoff To UMN Professor Leigh Turner Sept 30 2015Documento1 páginaEmail From Sen. Terri Bonoff To UMN Professor Leigh Turner Sept 30 2015MarkingsonCaseAinda não há avaliações
- Letter From Leigh Turner To Sen. Terri Bonoff and Other Legislators Regarding Psychiatric Clinical Trials and The Recruitment of Involuntarily Held PatientsDocumento3 páginasLetter From Leigh Turner To Sen. Terri Bonoff and Other Legislators Regarding Psychiatric Clinical Trials and The Recruitment of Involuntarily Held PatientsMarkingsonCaseAinda não há avaliações
- Update On Therapeutics: Shehan Williams and Thilini RajapakseDocumento3 páginasUpdate On Therapeutics: Shehan Williams and Thilini RajapakseAnjula KumarasingheAinda não há avaliações
- AZN-GLOBAL-Annual Report - FullYear 2006 PDFDocumento184 páginasAZN-GLOBAL-Annual Report - FullYear 2006 PDFMurad EltaherAinda não há avaliações
- 4 5891148413604464740Documento26 páginas4 5891148413604464740kelid IbrahimAinda não há avaliações
- New Psychiatric MedicationsDocumento60 páginasNew Psychiatric MedicationsDrima EdiAinda não há avaliações
- Case No. 8 Nicholas SheffDocumento5 páginasCase No. 8 Nicholas SheffMARIA ANTIONETTE LAMERAinda não há avaliações
- Quick Reference BWDocumento2 páginasQuick Reference BWmcbermudezAinda não há avaliações
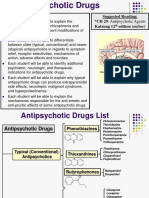
- Anti Psychotic DrugsDocumento2 páginasAnti Psychotic DrugscalfornianursingacadAinda não há avaliações
- The Presentation, Recognition and Management of Bipolar Depression in Primary CareDocumento9 páginasThe Presentation, Recognition and Management of Bipolar Depression in Primary CareJuan PerezAinda não há avaliações
- Antipsychotic Drugs - Wafa Bin ShamlanDocumento8 páginasAntipsychotic Drugs - Wafa Bin ShamlanSara AbdoAinda não há avaliações
- Antipsychotic Drugs in EpilepsyDocumento5 páginasAntipsychotic Drugs in EpilepsyAttaufiq IrawanAinda não há avaliações
- Nami Understanding Psychosis BookletDocumento59 páginasNami Understanding Psychosis BookletSalma KarimahAinda não há avaliações
- Mental Health and Psychiatric Nursing: Vernalin B. Terrado, RNDocumento35 páginasMental Health and Psychiatric Nursing: Vernalin B. Terrado, RNverna100% (1)
- Rapid Cycling Bipolar Disorder in Adults - Treatment of Mania and Hypomania PDFDocumento12 páginasRapid Cycling Bipolar Disorder in Adults - Treatment of Mania and Hypomania PDFdreamingAinda não há avaliações
- Asmal Et Al-2013-Cochrane Database of Systematic ReviewsDocumento196 páginasAsmal Et Al-2013-Cochrane Database of Systematic ReviewsAngel ArmasAinda não há avaliações
- About This List DosingDocumento15 páginasAbout This List DosingAla AbushehabAinda não há avaliações
- Rapid Tranquillisation Training PresentationDocumento42 páginasRapid Tranquillisation Training PresentationmindpinkAinda não há avaliações
- Tardive DyskinesiaDocumento2 páginasTardive Dyskinesiajhonny12321Ainda não há avaliações
- Quiz 5Documento28 páginasQuiz 5YAinda não há avaliações
- Antipsychotics and SeizuresDocumento3 páginasAntipsychotics and SeizuresAttaufiq IrawanAinda não há avaliações
- Biquelle XL 50mg, 150mg, 200mg, 300mg, 400mg Prolonged-Release TabletsDocumento2 páginasBiquelle XL 50mg, 150mg, 200mg, 300mg, 400mg Prolonged-Release TabletsAdam ToddAinda não há avaliações
- SeroquelDocumento2 páginasSeroqueldanaAinda não há avaliações
- Appendix BDocumento133 páginasAppendix BmuksedAinda não há avaliações
- Lecture 3 PsychopharmacologyDocumento99 páginasLecture 3 PsychopharmacologyPavan chowdaryAinda não há avaliações
- AntipsychoticsDocumento29 páginasAntipsychoticsTyler Lawrence Coye100% (5)
- (Peter M. Haddad, Serdar Dursun, Bill Deakin) Adve (BookFi) PDFDocumento335 páginas(Peter M. Haddad, Serdar Dursun, Bill Deakin) Adve (BookFi) PDFFrancesca Ruiz100% (1)
- False Positive in Urine Drug TestDocumento11 páginasFalse Positive in Urine Drug Testhenry omacheAinda não há avaliações
- Formularium Pertamina 2017 PDFDocumento51 páginasFormularium Pertamina 2017 PDFyohanAinda não há avaliações