VOLUME 10, NUMBER 1, MARCH 1985
THE AMERICAN TINNITUS ASSOCIATION
ELECTRICAL STIMULATION
FOR TINNI TUS RELIEF:
("Old wine in new bottles"?)
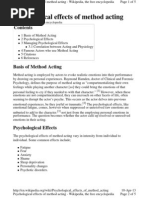
The 11ccomponying illustration
(reprinted from the Proceedings
of the II lntern11tionnl Tinnitus
Seminar) shows 11n elcctrical
stimulation device used by C.J.C.
Gropengiesser (1801) to delivel'
electrical current to the ears.
This issue of the Newsletter is
devoted to on explor11tion of the
concept of electrical stimulation
for the relief of tinnitus
in articles by three scientists
who are actively and presently
engaged in this work.
*
*
*
. '
! ~ d J 6
'I ;
. .....
* * * *
*
*
*
..
A REVIEW OF ATTEMPTS TO USE ELECTRICAL STIMULATION
TO PRODUCE SUPPRESSION OF TI NNITUS
All of us, patients and clinicians alike, constantly hope for more and better ways to relieve tinnitus. Since
tinnitus con arise from o. greo.t variety of c11uses it is not rensonable to expect any one treatment to be effective
in all or even most cases. What works well for one individuul or group of patients, moy hove no effect for another.
Thus, it is encumbent upon those working in this nreo to maintain the search for relief procedures.
Very early in the literature on tinnitus the use of electrical stimulation wos investigated by C. J. C.
Gropengiesser in Derlin, Germany. Vollo. hud reported on his own invention of the Volto.ric Cell, or the battery, in
1800 and in 1801 Grapengiesser published a book on the use of galvanic current (DC) provided by the battery in
attempts to cure a variety of diseases such as tinnitus . Some details of Gro.pengiesser's work may be seen on poge
123 o.nd 124 of P..I:.9..s:.e...e.Wns of l.hf! 11 lntetwltionol Tinnitus Seminar, which is avo.iloble through ATA. In summary,
Grapengiesser found that DC could be made to suppress tinnitus in some co.ses but he did not recommend It as a
relief procedure since it produced pain and nausea, as well. Looking bo.ck over Gropengiesser's work it now appears
most likely that it wo.s the manner by which he delivered the electrical current which produced the pa i n and nausea
rather thon the presence of the current itself. More about this later.
The next use of electrical stimuli on tinnitus patients was by three investigators, llatton, Erulkar ond
Rosenberg, working in Philadelphia, Pennsylvania, in 1960. These investigators observed that galvanic (DC)
stimulation which was routinely employed as a test for vestibular function (balance) olso altered the Intensity of
tinnitus in some cases. At about the same time Tasald and Fernandez had found that DC applied to guinea pigs
acted only on the audl tory receptors (the hair cells in the Inner ear) and not upon the nerve fibers or the higher
auditory centers in the brain. Thus Hatton et al. reasoned that perhaps DC could provide a test to distinguish
tinnitus due to peripheral causes from thot due to more centro! causes. They tested 33 tinnitus patients and found
15 for whom the DC applied to the ear had a positive effect. These i nvestigators revealed several Important
aspects of using electrical stimulation:
1. The intensity of the current was gradually increosed and gradually decreased; it was never suddenly turned on and off.
;;. Only anodal (posi live) stimulation produced the suppressiou effect. Cathodal (negative) stimula lion ei lher increased the
intensity of the tinnitus or produced an auditory sensation or both.
Page 2.
(continued from Page 1.)
3. When suppression of tinnnituss occurred it did so only so
long as the current was present. There was no aftereffect.
4. The DC which wos effective in depressing tinnitus did not
produce any alteration in hearing ability.
5. The majority of the 15 patients for whom electrical
stimulation suppressed the tinnitus also had severe hearing
losses. Those of us who try to use masking for the relief of
tinnitus were especially interested in this finding inasmuch as
patients with severe to profound hearing losses are often not
candidates for masking.
These three investigators concluded that use of DC
applied to the head shQ.!ili1 UP!. be considered as a therapeutic
procedure, since it is known that DC can also produce tissue
damage. It is of interest to note that five years later
Hatton wrote a general article on tinnitus in which he did
not even mention his own earlier work using DC. In a
personal correspondence with Dr. Hatton he indicated to me
that he had not considered the use of DC as a viable relief
procedure for tinnitus since it had to be constantly present to
have an effect, and that kind of stimulation would surely
produce not only damage to hearing but possibly to the
vestibular (balance) system as well. Moreover, he repeated
that application of DC only worked in 15 of 33 (45%)
patients.
One final comment about the Hatton, et al. work. They
defined suppression of the tinnitus as complete elimination of
it and not merely a partial reduction in intensity. They
report that when a patient noticed the beginning of reduction
of tinnitus that it was then necessary to increase the
intensity of the DC by only 1 milliamp (rnA) or less to effect
complete elimination. The current strength necessary for
complete suppression varied from 1.5 rnA to 8.8 rnA according
to the patient. These are fairly high levels and possibly
capable of producing damage with sustained use.
The next set of studies of electrical suppression of
tinnitus were the result of a happy accident. Aran and
colleagues working in Bordeaux, France used an electrical
stimulation test to select candidates for the cochlear implant
operation. Routinely, they applied electrical stimulation to
the round window membrane of the inner ear, when they
accidentally discovered the reduction of tinnitus in one
patient. That discovery led to a series of studies of the
effect of electricity upon tinnitus. Aran and coworkers
obtained essentially the same results as did Hatton et al.,
that is:
1. Only anodal (positive) stimulation produced reduction of
tinnitus.
2. The suppression effect was proportional to the intensity
of the stimulating electrical current.
3. The suppression effect occurred only during the time the
current was present; there was no after affect.
Aran had more directly stimulated the inner ear than had
Hatton, and Aran's results were better. He obtained
complete relief of tinnitus in 60% of the cases tested. Aran
used a different form of stimulation. Hatton had utilized a
continuous stimulation, whereas Aran pulsed it in an effort to
reduce its damage potential. Like Hatton, however, Aran
concluded that electrical suppression of tinnitus was not a
proper or safe therapeutic procedure.
At about this time in the course of events electrical
stimuli began to be used to control pain. Intractable pain
was found to be controlled for many patients by what came
to be known as TENS units. TENS means Transcutaneous
Electrical Nerve Stimulation and it often employs repetitive
pulses of anodal Do-much the same as Aran had used for
tinnitus. The interesting thing about TENS is that not only
does it work for a large number of patients, but also it seems
to have produced no neural or tissue damage. According to
FDA, the TENS units are considered to be safe for control of
pain, but it must be indicated that in that application, the
current intensities are low.
The TENS literature stimulated a Parisian physician
named Chouard to try the same procedures on the ear for the
control of tinnitus. He proceeded to employ a great variety
of wave forms, all of which were pulsed. He used anodal,
cathodal, and biphasic forms of DC at a variety of pulse
rates; he also tried AC, which is like our household
electricity. It is a bit difficult to follow the report of all
the conditions used and results obtained, but all forms of
electrical stimulation seem to have produced relief in some
cases. The interesting and, perhaps, most significant aspect
of Chouard's work is that when relief was produced, it often
persisted well after the cessation of the electrical stimulus.
He demonstrated a positive aftereffect. This same effect
had also been demonstrated earlier by Hazell and Graham,
working in London, England, who had utilized AC stimulation.
It was common to both studies that the aftereffect lasted as
long as four hours.
At this point in the review of the literature, one could come
to the following conclusions:
1. Electrical stimulation in, perhaps, a variety of forms ts
capable of suppression of tinnitus to some degree.
2. The precise form for the best electrical stimulation and
the exact electrode placement are not known.
3, The extent or nature of potential tissue damage is
unknown.
4. The duration of any electrical suppression is unknown, but
there is the strong suggestion of the possibility of an
aftereffect.
5. The possibility of the use of electrical suppression for
tinnitus needs further study.
It was at about this point that we at Kresge Laboratory
decided to initiate some studies of the electrical suppression
effect. Support for these studies was provided by ATA and
The Murdock Charitable Trust, for which we are most
grateful.
We decided essentially to repeat the work of Chouard,
in that a variety of forms of stimulation would be utilized.
Most of our differing forms were provided by TENS units.
The one exception was a special wave form which, in human
brain tissue, had demonstrated the capacity to effect
stimulation while at the same time producing the least amount
of tissue damage. This particular wave form can be
illustrated accordingly:
+
0
Note that the positive (anodal) portion of each pulse is of
greater magnitude (intensity) than the negative (cathodal)
portion. On the other hand, the duration of the positive
portion is much less than that of the negative portion. These
two values, intensity and duration, are so arranged that their
product (intensity x duration) yields the same result in both
cases. Such an arrangement should provide sufficient positive
current to effect electrical suppresion of tinnitus, while at
the same time, providing sufficient negative current to cancel
the damaging effects of the positive portion.
Page 3.
(continued from Page 2.)
We tested a total of 50 patients and, much like
the Chouard, found that every form of stimulation
produced a suppressive effect in some patients. We
defined suppression as being a reduction in the intensity
of the tinnitus by 40% or more. We only found 14
patients out of the 50 (28%) who met the criteria of
tinnitus reduction by 40% or more.
The most effective forms of stimulation were the
special wave form described above, and another biphasic
wave form which was fairly similar to it. This finding
seemed to indicate that it was not essential to use only
an anodal stimulus, as indicated by Hatton and by Aran.
It seemed to say that a wave form which was
potentially less damaging to tissue was effective in
suppression of tinnitus.
We also found the suppressive effect to extend
beyond the time of current passage. In some cases, the
effect lasted well over five hours after stimulation, and
the duration of stimulation had been only 5 minutes.
There were no detectable alterations in hearing ability
at any of the audiometric frequencies.
We initiated our study with a placebo trial, which
was carefully arranged to properly "fool" the patient.
Only two of the 50 patients (4%) perceived any change
in their tinnitus during the placebo trials. This is
similar to the placebo findings of Chouard and suggests
that tinnitus patients are not susceptible to the placebo
effect.
Our data are discouraging, in that we were able
to find electrical suppression in only 28% of the cases
tested . On the other hand, we are encouraged to
continue the search in that the suppressive effect, when
produced, tended to be long lasting and we found no
evidence of negative effects. Moreover, when
questioned as to whether they would prefer masking or
electrical stimulation, assuming equal and good
effectiveness, 54% of the patients indicated a
preference for an electrical device. Responses of that
sort are not hard to understand--after all, with the
proper version of an electrical device, one does not
experience anything but relief, whereas masking
provided the constant presence of the substituted sound.
Our present thinking about electrical suppression
is this: The success rate is low, according to most
investigators: Hatton--45%, Aran--40% with one
arrangement and 60%, with another, Chouard--from 25%
to 45% and Kresge Study--28%. That success rate,
however, must depend, at least in part, upon the
current path. That is, can the electrical current be
made to pass either through or near the inner ea1 (not
the outside ear) or parts of the higher auditory
centers? In most of the above studies, the electrodes
were placed on the skin either behind or in front of
the external ear. It is highly likely that the main
current path traveled immediately below the skin from
one electrode to the other with little or no current
into the inner ear. For those who obtained tinnitus
suppression, perhaps the effect was produced by an
indirect field effect. Let me hasten to add that these
comments about probable current path are pure
supposition and based on no measurable observations.
Nevertheless, we intend to utilize this brand of thinking
for our next study using electrical stimuli. The highest
success rate, (60%), was found by Aran when he used
one electrode directly upon the round window membrane
of the inner ear. In this manner, he was assured that
the current path would primarily run through at least
part of the ear. Aran utilized an acute demonstration,
whereas, if one is to consider a chroni c implanted
electrode, the technical problems increase greatly. In
order to implant a round window electrode, it is
necessary to reflect
approximately half the eardrum in order to gain access
to the middle ear space and while this is a routine part
of the operation in the surgical treatment of
otosclerosis, it nevertheless is an involved procedure.
Aran also placed an electrode on the bony wall of
the inner ear called the promontory, which was the
arrangement giving 40% success. The placement of that
electrode was achieved by sticking a needle (the
electrode) through the eardrum, which was considerably
less involved than turning a large flap in the eardrum.
We plan to use a similar procedure with some
modifications so that an electrode larger than that of
the point of a needle will be the effective stimulating
surface. The electrode will be passed through a small
slit in the eardrum so as to contact the promontory. A
slit in the eardrum is a routine procedure used to place
ventilation tubes in the eardrums of children who suffer
with middle ear infection. It is a simple operation
performed under local anesthesia and is the most
frequently performed operation on humans. If this
proposed procedure produces a sufficiently high success
rate to recommend it as a therapeutic procedure, it will
then be necessary to obtain permission from FDA to
conduct clinical trials in order to demonstrate the
worth and safety of the procedure. Please remember,
gentle reader, such things take time.
Respectfully submitted,
Jack Vernon, Ph.D.
Kresge Hearing Research Labor a tory
*
POSSIBLE AlD FOR TINNITUS SUFFERERS
by Marvin Engelberg, Ph.D.
*
On January 12, 1985, at the Triological Society
Meeting in New Orleans, William Bauer, M.D., presented
the results of a study he and Marvin Engelberg, Ph.D.
conducted at the Cleveland Veterans Administration
Medical Center on Transcutaneous Electrical Stimulation
for Tinnitus. There were two experiments to this
study: the first experiment was designed to evaluate the
effectiveness of the stimulation without adhering to a
strict research protocol. The second experiment
utilized a single blind protocol. The 30 subjects in the
two experiments were primarily adult male, their ages
ranging from 23 to 74 years. The duration of the
t i nnitus ranged from one week to 40 years. Probable
etiologies of the tinnitus included ideopathic, noise,
diving barotrauma, heredity, endolymphatic hydrops,
dental restoration, head trauma, and hypertension.
The stimulation was administered from the Alpha
Stirn 2000 pulse generator instrument, utilizing an
electrical stimulus consisting of a square DC biphasic
pulse with a low frequency, low current intensity, for
24 seconds to two minute stimulation, applied to 13
specific sites on the auricle ipsilateral to the tinnitus.
These 13 sites were selected for their low electrical
resistance levels.
The results of experiment #1 defined improvement
as either a complete remission of the tinnitus or a
decrease in the tinnitus frequency. The results of
experiment #2 revealed that 82% of the 33 ears with
t i nnitus ( 20 subjects) showed improvement. Test-retest
tinnitus frequency measurement appeared to be as large
as 22%. The permanence of the improvement ranged
from as short as 20 minutes to as long as at least six
months (last contact with the investigators). There
were no adverse side effects from the stimulation. The
authors discussed the numerous variables associated with
this procedure and the need for additional
experimentation. A complete account of this study will
be published in The
Page 4.
EXTERNAL ELECTRICAl, STlMULATlON--TINNlTUS
CONTROL--A PROGRESS REPORT
by Abraham Shulman, M. D.
External Electrical Stimulation (EES)--Tinnitus
Controi--(TC) represents the application of high
technology to attempt to control the symptom of
tinnitus . The results at this time represent a
re-introduction of an old modality--that is, electrical
stimulation for tinnitus control. Any and all results
related to EES need to be interpreted in relation to the
device used and Its specifications. Also to consider the
results not In terms of 'cure' but rather 'control'. This
distinction reflects the diversity and complex! ty of the
symptom of tinnitus in each particular tinnitus patient.
Since 1983 our group (Downstate Medical Center)
has been using a device called the Tinnitus Suppressor
(TS). It was designed by Richard Dugot of the Audimax
Corporation, South Hackensack, New Jersey. A basic
prototype was used from February, 1983 to June 30,
1984. The definitive unil, designed as a head set, has
been used since July, 1984. To date, approximately 40
patients have attempted to use the TS. The trials of
TS have continued on two levels, (a) investigational,
and (b) clinical tinnitus patients for TC. In the general
tinnitus population an overall success rate is projected
to be approximately 2 5 ~ . However, in selected cases, a
higher degree of success of 40% or better has been
achieved. We have measured 'success' in terms of
tinnitus control not tinnitus cure. In an attempt to
evaluate the efficacy of this method (i.e. EES for TC)
it has been found necessary lo establish clinical
correlates bet ween the parameters of the electrical
stimulus being used, and the parameters of the tinnitus
before, during, and following stimulation. Electrical
tinnitus suppression refers to the reduction of intensity
of tinnitus. It is necessary to distinguish the reduction
of intensity of tinnitus during the electrical stimulation
from the continued absence of the tinnitus following
cessation of the stimulation. The parameters of the
electrical stimulus are specified with respect to its
latency, intensity, quality, and duration. Tinnitus
suppression pnrameters are now compared to the original
tinnitus parameters prior to EES. The parameters of
tinnitus are its quality, location, intensity, and
duration. A 'Tinnitus lntensi ty Index' (Til) is kept by
the professional, and by the patient emphasizing the
parameter of tinnitus intensity. On a scale of 0-7
1
where 7 is the worst possible tinnitus, and 0 the
absence of tinnitus, n numerical designation is assigned
to each of the parameters of the tinnitus as well as to
associated complaints of hear i ng difficulty, ear
blockage, and vertigo. In this manner, an evaluation
can be made comparing the situation before, duri ng, nnd
after EES. In general, the highest rate of success has
been obtained in patients Identified as having the
symptom of tinnitus arising from the peripheral portions
of the auditory system ("end organ"), and not the head,
("central"). An index designation of 3 is considered TC
at this time.
Proper patient selection is considered critical for
optimum results. The medical-audiologic evaluation for
tinnitus attempts to properly select patients and
includes a general medical evaluation, neurotologic
evaluation, and assessment of the function of the
auditory nerve for its cochlear and vestibular
components. The tinnitus is analysed with respect to
its parameters of location, intensity, quality, and
duration. The team approach of neurotologist and
audiologist provides a medical-audiolog ic basis for
patient selection and monitoring of the errect(s) of EES
for TC. The most successful cases are patients who
complete the medical-audlologic evaluation and
demonstrate a peripheral 'site of lesion' of the tinnitus;
the tinnitus could be masked; absence of active ear
disease, with particular attention to adequate aeration
of the middle ear and absence of i nner ear diseas e such
as endolymphatic hydrops.
In summary, the patients for whom EES is
successful are those in which the following key
elements have been realized:
a. A neurotologic evaluation correlated with the
general medical evaluation.
b. A cochleo-vestibular evaluation of nerve
function of the ear, which has attempted to
establish the site of lesion of the tinnitus.
c. 1\ tinnitus evaluation by on audiologist, in
which the tinnitus has been identified in relation
to its parameters prior to EES, and in which it
hns been determined whether or not that patient's
tinnitus can be masked.
d. A medical-audiological team evaluation of the
clinical history and of the
neurotological-audiological test results for
patterns of response that can be identified for
both 'site of lesion' as well as etiology of the
tinnitus symptom.
e. Adequate control of active ear disease with
particular attention to the existence of
satisfactory aerat i on of the middle ear, and
absence of endolymphatic hydrops of the inner
ear .
(. Anxiety control is critical.
The advantages of the system of EES for TC have
been:
a. No external sound introduction to the patient
b. Minimal side effects
c. Lack of Interference with the occupation
ond/or activities of the patient while stimulation
is in progress
d. Hearing unchanged; (questionable improvement
reported by a few patients)
The disadvantages include reports of occasional
increased intensity of tinnitus, and/or a change in the
quality of the tinnitus. These effects have been of
short duration and have been followed by return of the
tinnitus to its original natural course within 24-48 hours
of cessation of EES.
In summary, EES for TC using the TS has resulted
in a significant incidence of tinnitus control. Proper
patient selection is considered critical for optimum
results. Lastly, monitoring of the patient during
electrical stimulation Is necessary under professional
supervision.
1he American Tinnitus Association is a member of the
National Voluntary Health Agencies for the Combined
Federal Gi ving Campaign. Please, if you are a Federal
worker, designate ATA to receive all or part of your
yearly charitable contribution. If you are acquainted
with a Federal worker you can help ATA by reminding
them that we qualify for participation in thei r annual
campaign.
NEW TINNITUS RESEARCH PROJECT FUNDED BY ATA
We are pleased to announce that a substantial donation
has been given by an ATA member and designated for
the purpose of allowing Dr. Jack Vernon to continue his
work on the development of electrical stimulation
techniques for the suppression of tinnitus. This
generous donation for research benefits all of us who
hove tinnitus by bringing ever closer that day when we
will be nble to turn of( head noises . On behalf of all
of us with tinnitus , THANK YOU!!
Page 5
TRIBUTES
The ATA tribute fund is designated 100% for research. Thank
you to all those people listed below for sharing your memorable
occasions in this helpful way. Contributions to the tribute fund nre
tax deductible and will be promptly acknowledged with an appropriate
card for the occasion. The amount of the gift is never disclosed.
- -----
I N M F1110llY
1
OF
catherine R. Williams
Bessie Gitlelson
Bernyce Sherman
Wa I t e r We I I s
Dr.Abraham Seidel
Derne.rd Drown
carmen J . CUgglano
Iris Kindred
Ila r r i e t M i I I e r
1/aig Soghomonlan
Phillip C. Keefer
Dr. Joseph Freeman
Helen Beattie Thorp
Etta Hayman
Edgar Schu I tz
Douglas Polivka
llarold Wrightington
Jimmy Feurer
Joseph Ce.rtaxo
Fanny Munter
May Panas
Hilda Creighton
Sophie Cllier
David Leeson
Richard Pieser
Richard Myszka
Alan Stein
Veronica Marcincok
Josephine Schmidt
Harry Cassel
IN HONOR OE
Speedy recovery
Dr. Robert Johnson
50th Anniversary
Mr.& Mrs .Jack llorwi tz
Ret I remenf
Renee &. Michael Stone
Engagement
Jonathan Stone
New Grandaughter
CDliilllill.l.IDR
Mr.& Mrs. Hobert Woiste
Mr.& Mrs. Efrom Abramson
Mr.&. Mt s. Ef rom Abramson
Mr.& Mrs. Henry Adams
Mrs . Anne Seidel
Mrs. Detty Abbott Brown
Ms. Chester Diangelo
Mr. Gi !bert Simons
Irene M. Stockdale
llenry &. Doris Adams
Mrs. Norma Mae f{eefer
Jean & Joe Wolfson
Joseph Alam &. Trudy Drucker
Burton Zitkin
Jake De Young
Jake De Young
Brendan & Dorothy Greene
Brendan & Dorothy Greene
Joseph Alam & Trudy Drucker
Sam &. Sylvia Eisenberg
Mr.& Mrs .Howard llorwi tz
Aram & Rosemary Cartozian & F.
1\lr .&. Mrs. Efrom Abramson
Mr.& Mrs . Efrom Abramson
Mr.& Mrs. Efrom Abramson
Anthony J . Myszka
Bob llocks
Bob & Lois Brickhouse
Rose & Joe Kempf
Trudy Drucker &. Joseph Alam
Q)lilli.Bll.ID.Il
IIi s friends at ATA
Mr .1'1 Mrs .Howard tlorwl tz
Joseph Alam &. Trudy Drucker
Joseph A! am &. Trudy Drucker
WORDS OF WISDOM FROM OUR READERS
l..ti.llOOQlLQE
Ruth Kromer
Sandy
Sandy
Sandy
Sandy
Sandy
Anna Strom
Esther l<aplan
JoN. Alexander
Robert Guinto et al.
Honold W. Ce.rye
Charlotte J. Snyder
B. I.R.11ID.AY
Mike Mi lis, 65th
Carolyn Traver
Trudy Drucker
Trudy Drucl<er
Tnrdy Drucker
Trudy Drucker
Trudy Drucker
Eve Show
Arlene Levy
Trudy Drucker
Helen Thorp
Jacqueline Doyle
Bill lluott
Dr . Max M. Novlch
Nino Novich
Joyce E. Koehler
Jomes P. Doyle
Pamela Trover
John G. Alam, Jr.
Trudy Drucker
Trudy Drucker
Trudy Drucker
CON'ffi I BIUDR
Sylvia Otown
Mr.& Mrs. John Schleter
Poye Schleter
Faye Schleter
Faye Schleter
Foye Schleter
Janice Virkler
Stanley J. Kaplan
Dovid M. Alexander
Bergen County Self-help Grp.
Jim Whitlock , M.D.
Rose & Alfred Polen
CDN'Illl BUIDR
Sylvia O r o ~ ~ & Ben Mills
Joe Alam & Trudy Drucker
The Trover Forni ly
Love--Yusuf
Mabel llopper
Mary & Patrick Tully
Eve D. Show
Alam & Drucker
Alam & Drucker
Ms . A. B. Alam
Alam & Drucker
AI am & Drucker
Alam & Drucker
Alam & Drucker
AI am & Drucker
J. Alam & T. Drucker
Alam & Drucker
Alam & Drucker
Alarn & Drucker
Jules II. Drucker
Mary & Gll cassel
ller friends at ATA
(For those of you who don't belong to a tinnitus self-help group these letters and writings are a way of sharing the
feelings that are common to so many tinnitus sufferers. \Ve hope that these words help you to better understand
the woy tinnitus can change one's life.
I am a tinnitus sufferer and have been for some years now. I am a member of ATA and receive the ATA
Newsletter. In the Vol.9, Number 2, October 1984 issue I came across an article on page 2: "Another
View"--(Excerpts from a letter written by a former musician to his fellow players. )
For some reason this article really impressed me, so much so, that I took it in and read it to my wife. After
I was through reading it to her, she said thnt the article described me exactly. I thought about it and decided she
wos right. I guess the difference is that I do most of the things that he can't because I wear a molded ear plug in
my right ear and a noise breaker in my left eor. I hove taken a lot of ribbing f rom the fellows at work ond once
in a while people will give me on odd tool< -- people who don't suffer from this malady can't really understand what
it is like to be hypersensitive to sound -- but I soy "to heck with them, if wearing this protection all the time will
give me and my family a somewhat normal life- do It!!" These plugs let me do most of the activities that the
former musician listed tho t he couldn't do. For some of the noisier activities I will wear double protection. The
noise that chain saws and rock concerts generate (incidentally, I do think of these two types of noise as the same)
is just too much for me to cope with, even with extra hearing protection.
Just as the ex-musician, there are certain things In my early life that I would change If I could. \Vhen I was
growing up, hearing, and a person's ears were really not a thing to consider. Seeing how far you could make a
person jump by producing a very loud noise, was quite acceptable. Now the cog has turned and people are very
much tuned in to hcnl'ing nod problems relnted to it. I guess one of the most Important things we con do at this
point is to spread the word to our children and friends do that they won't have to suffer and go through the pain
tlltd we, my ftmily uucl I, live with evcry dfly. Yours truly, nove Creighton
Page 6.
WORDS OF WISDOM FROM OUR READERS
(continued from Page 5,)
To whom it may make feel better about having a
problem with ringing in your ears called "Tinnitus."
While in the hospital I met this very nice person
and she asked me something and I didn't hear her . I
was trying not to be rude, but I had turned my masking
hearing aids down in hearing volume and the maskers
up. After I adjusted it so I could hear her I asked
_she had and explained that I was' sitting
hstemng to the ram. She said again what she said, but
looked at me with a very puzzled face. She said "I
don't mean to confuse you, but it's sunny outside!"
Then I thought about what J said and later decided
to write this so you may escape into the comfort that
at times I enjoy. Only have this special ability.
The sun may be shining outside and yet you nay feel
the need for relaxa tlon inside.
I thank God, Dear Abby, ATA, and Mr. and Mrs.
for helping. me a_nd I hope that after reading
this first, then read1ng L.U..t.e.n to the rain next, that
you may feel more comfort in wearing your aids and
like (listening to the rain,) you too will feel very
special.
Sincerely,
John Burleigh
LISTEN TO THE RAIN
Life is often so busy and noisy, that people never
listen to the comforts of life. God created birds
for their music, children for their laughter, but
also rain for its beauty.
Often people get depressed with rain. It does much
damage, but it does much creative work also. It
creates beautiful flowers, beautiful landscapes,
but to me, it creates beautiful music.
I think of times when I'm at camp or even at home
when the rain is beating on the roof. Never in the
same rhythm, and that's what makes it unique.
The rain is like music. Like a great symphony in
concert, every song comes pouring out ei thee soft
and gently that relaxes you or like the symphony
beating down at times so hard it brings your
adrenaline rushing through your body.
It's a shame that thunder has to come with the rain
because it often steals the beauty of rain,
somewhat like a person who talks and interrupts
the beauty of music.
But when the thunder stops and the rain continues
"for the sake of your ears and best of all your
heart," thats the time to 'listen to the rain'.
MORE WORDS ...
Not all tinnitus patients are as comfortable as the man
who wrote the gentle words you just read. Here is
another point of view. This unsigned piece is from a
man who has has helped numerous tinnitus sufferers
through_ his untiring efforts on their behalf, through his
compasstonate underst anding, and through his willingness
to put personal cares aside and render his services to
fellow citizens.
I can't see you , you unrelenting animal , You
th_at's always there. You're in my hair, you're on my
mtnd, you are lurking every where all the time. Don't
you ever give up? Don't you ever quit? What do you
You have my body, you have my every waking
m1nute, you have my every sleepless night. Even when
I do fall asleep from frustration or exhaustion, I still
know you are there. You have become more to me than
my family. Did I ever think in my wildest dream I
could ever say that?
You, you beastly godless creature, you spend more
time in my thought than do my wife and children. You
have robbed me of my soul. You have taken away my
waking thoughts. All of this and more you own. What
do you want? Do you want me to die for you? I have
given up all for you. My job, my kids, my laughter, my
dreams. All this you own, and you never have enough.
You know why I hate you even more? Nobody
knows about you. You stay hidden away where only a
few people know about you. You don't come out in the
open where others can see you, so they think I'm nuts.
People feel sad for me but not sorry. They think I'm
sick, maybe a little crazy. They don't know you,
doctors don' t know. How could they?
You are sleazy, you are slimy, you disgust me.
You want all of me. Professional people tell me to
live with it, They say "You get used to it." You
know what? I haven't been able to. But let me tell
you this, I ain't quittin'. I'm gonna bite you, kick you,
never let you know how you treat me.
. not giving in. There has to be a way. I
Will f1nd It, And do you know what the biggest pity
is? Very few know your name. I know doctors that
never even heard of you. But I have . You are
TINNITUS and I will find a way to rid you of me.
Don't worry, I' m flOinfl to win.
MORE WORDS ...
I would like you to know how much 1 appreciate
your Newsletter. I have had tinnitus for eight years
now and unless you've gone through this affliction it's
hard to understand the suffering and depression one has
with it. Just knowing that other people understand is
such a great help . Reading your Newsletter is
something I look forward to. lt's like talking to an old
friend who understands your problem.
J would also like to make a point about cordless
telephones. I received a cordless phone for Christmas
two years ago. I placed the phone next to my bed and
when it rang one night I forgot to turn the off switch
(standby-talk) , on the phone and the bell rang into my
ear. Because of that I now have a more severe
tinnitus problem. Before, I had a loud hissing sound of
air--now I have sounds of birds chirping and ticking
sounds plus a loss of hearing that I didn't have before.
My husband and I are trying to make as many
people as we can aware of the possible dangers of the
cordless phones and wonder if this can be covered in
your newsletter? Thank you, Mrs. C. D. Moore
Dear Mrs. Moore,
You've just made your point to about 40,000
readers of this Newsletter. We unders t and that the
ne_wer cordless telephones have better protection ngainst
th1s problem. Your letter reminds us that protection
and prevention are the only 'real' cures for tinnitus .
Page 7.
HISTORICAL ORIGINS OF THE TREATMENT OF TINNITUS
by s.n.G. Stephens
(1llis article is reprinted with the permission of the British
Tinnitus Association)
The treatment of tinnitus can be traced back at least to
ancient Egypt and Mesopotamia and since the earliest times
there has been controversy as to whether it should be treated
as a specific entity or merely as a reOectlon of the
underlying ear disease.
The concept of treatment of tinnitus as a port of the
treatment of the underlying ear disease, dates back at least
to the time of Pliny the Elder, who compiled a compendium
of 'traditional' and 'orthodox' medical remedies for ear
disease which included tinnitus within the general context.
These treatments were often bizarre and scatological,
including such items as woman's milk, foam from a horse's
mouth, ass's dung, and boar's semen. However, such
approaches persisted until at least. the nineteenth and
provided much of the basis of car1catures of the medieval
physician and the later travelling quack.
Medieval theories
On a more quasi-scientific basis, a variety of herbal and
mineral oil bused products for administration to the patient's
ears for the treatment of otalgia, hearing loss and tinnitus
recur in innumerable medieval herbals and other manuscripts.
Du Verney (1683), who wrote the first major text book
otology, devoted 10 pages to tinnitus. He that .t
should be man11ged by treatment of the underlymg ear dJSease,
making no mention of symptomatic treatment. This view has
been renected in innumerable otological text books through to
the present day.
Since no technique at the present time can 'cure'
tinnitus on a permanent basis, it has been argued by Hallam,
Rachman and Hinchcliffe that therapy should be orientated
towards helping the patient to habituate to the condition. I
shall therefore, consider the symptomatic treatment of
tinnitus within the context of this habituation concept which
argues that the normal pattern is for habituation to develop,
this being reflected in the fact that population surveys have
shown that only a small number of tinnitus sufferers are
disturbed by the symptom.
Doth pharmacological and psychological approaches to
the management of tinnitus have been used .
historical times, with electrical suppression of tmrutus dating
from the 18th century and acoustical suppression and surgery
first being applied in a systematic manner only in the early
and late 19th century respectively.
Psychological treatment among the Annamites of
India depended upon a quasi-rational treatment of the t1nmtus
according to their theory of its causation. Thus they
considered that hearing took place by means of the activation
of a small animal within the ear. However, if it became
irritated or involved in a fight with a similar animal, this
gave rise to tinnitus. The animal could be by
fumigating the ear with smoke from the burmng skms of
non-poisonous snakes.
A more orthodox approach came with the use by the
Babylonians of incantations calling on the 'ghost' causing the
tinnitus to leave the patient. These ranged from a simple
'Whoever thou may be, may Ea restrain thee', to
'lt hath flown against me
It hath escaped the earth
It hath attacked me
0 seven heavens, seven earths,
seven winds, seven hurricanes,
seven fires, seven backs, seven sides
By heaven be ye exorcised
By earth be ye exorcised
Fly away like a bird of the heavens
Rise to the sky like smoke
Like a rainstorm disappear into the ground!
May the magic of the word of the great
Lord Ea of Eridu be not annulled.'
This with the use of the magical number seven times seven,
with the astrological and divinatory theories developed
by the Assyrians. In both this and tltc by
the Annamites it is arguable that reassurmg the patient that
the causative factors underlying the disease process had been
dealt with would enable the patient to better accept the
symptom and facilitate the habituati.on .
Pharmacological treatments of the llme.s, wh1ch
accompanied these incantations and were .sometimes
independently administered, cons1sted of
relatively innocuous oils and restns mtr?duced mto the. outer
ear or of mild purgatives. At best thetr effects are hkely to
have been palliative.
Humoural imbalance
Graeco-Roman medicine interpreted tinnitus as an
imbalance between the humours and advocated a range of
relatively orthodox purging techniques coupled local
application of oils to the external meatus. Agam,
treatments probably helped the to the tinmtus
reassuring the patient that he had to worry wh1le
at the same time offering him the feehng that somethmg
useful was being done.
Hallam and his colleagues hove argued that
to the tinnitus is less likely to occur when the pa t1ent IS
over-aroused or has too little external stimulation to .dls.tract
him from his tinnitus. lt also occurs less when the hnnttus Is
inconsistent in nature. Approaches to the modification of
these situations were advocated by Galen, Alexander of
Tralles and Pseudo-Aristotle respectively. Thus Galen
that in certain patients with tinnitus, sedatives such as op1um
and 'mandrake should be administered. Alexander of Tl'o.lles
advocated that sufferers should go out into noisy open places
in which there was much noise and distracting activity and
Pseudo-Aristotle (c. thirteenth century) was the first
specifically to describe masking tinnitus by sounds.
111rough medieval times and mto the little
further advance took place in the management of tmmtus.
Even progressive medical seem:d more concerned
with extending the humoural theones to thetr .extremes than
with making systematic observations and apply1ng new
principles. Thus, for example, Paracelsus advocated repeated
scarification of the auricle, cupping behind the ear and
venesection under the tongue.
Surgery . .
The first approach to surgery was llkew1se based on the
theory dating back to Greek times which. ha.d suggested
the tinnitus wns caused by air trapped w1thm the ear wh1ch
then spun around within the ear like a miniature tornado.
Jean Riolan the younger argued that relief
by trepanning the mastoid process and allowmg th1s a1r to
escape. . .
The empirical treatment of tmnitus came With the
applies tion of electricity to the ear. by ( and
others. This became more systematised 1n the runeteenth
century by the work of Brenner who demonstrated the
importance of the use of anodal stimulation, although
experienced contemporaries such as McNaughton-Jones found
the overall results disappointing.
A fresh approach to the of tinnitus be
seen in the work of ltard, working wtthtn the more emp1r1cal
and observational tradition of the Parisian School of the late
eighteenth and early nineteenth centuries. While for certain
types of tinnitus he still advocated a humoural theory-based
approach such as cupping and bleeding, in most other cases
he took fresh look and had an enlightened attitude,
admitting frankly for the first time that most patients could
not be cured and that therapy should be orientated towards
the relief of the effects of the tinnitus on the patient.
(continued Page 8.)
Page 8.
(Continued from Pnge 7.
The effects which he highlighted were ongoing worry and
sleep disturbance, and to help these he devised various
masking procedurs to help the patient in his home trying to
get to sleep. These included the sound of a roaring fire in
the patient's bedroom, a fire with damp wood whistling in it,
a stream of water falling on to a copper bowl or a clockwork
motor. ln n most extreme case of tinnitus following
psychological trauma, he achieved success by sending the
patient to live for a time in a watermill.
HAVE YOU SENT IN YOUR MEMBERSHIP
A more cogent consideration of psychological aspects
and treatment of tiunitus came only with the work of Fowler
in the mid twentieth century, and even since his time most
efforts have been concentrated only on a particular technique,
such as biofeedback, rather than attempting to adopt a more
global psychological perspective.
The author is Consultant Audiological Physician at '111e Royal
National Throat, Nose & Ear Hospital, London.
BOOKS BOOKS
DONATION?
Regular member $15 or more
Sustaining member $25 or more
Professional member $100 or more
Benefactor $500 or more
Name _____________________________________ _
Address ________________________________ __
Ci ty,State,Zip
Your ({ift is Tax Deductible
* * *
BOOKS BOOKS BOOKS
Tinnilus: of the 2ruLllilirrWl.t.iQnaL.lln.nLt.u.s..JieJn.irul.r is now available. This compilation of papers on the
subject of tinnitus covers subjects such as the mechanics of tinnitus, elect1ical stimulation, clinical assessment, and
various treatment methods. It Is the leading worl< In the field ot tinnitus relle(lroh. Tho book hoe boon printed In
England and is now here end being distributed from the ATA office. Prepaid orders only, please, in U.S. funds,
may be sent to: ATA, PO l3ox 5, Portland, OR 97207. Please make your checks for $25.00, which includes shipping,
to the American Tinnitus Association. Limited quantity available; reprinting is not anticipated.
Name
Address ______________________________________ _
City, State, Zip _______ _
* *
*
* *
*
*
llQ..'lli:;]
The American Tinnitus Association does not make its mailing list available to any other organization. Portia! lists are provided
to patients for the purpose of information nnd referral, or for their use in starting a self-help grotlp. The list is never to be
used for purposes outside the work of the ATA. Please do not abuse your membership privileges by letting the list fall into the
hnnds of anyone who is not part of ATA. We are repeating this message because it has come to out attention that some
membe rs have been solicited by promoters of treatments ond devices. Please be advised that there are safeguards being
programmed into our list so that further misuses will be nble to be traced and will be handled by legal counsel.
PubZished by tile
AMERICAN TINNITUS ASSOCIATION
A private non-profit corporation
tile Zaws of Oregon
SCIENTIFIC
ADVISORY BOARD
Jack D. Clem is, M.D.
Chicago, Illinois
David D. DeWeese, M.D.
Portland, Oregon
John R. Emmett, M.D.
Memphis, Tennessee
Chris B. Foster. M.D.
San Diego, California
Howard P. House, M.D.
Los Angeles, California
Robert M. Johnson, Ph.D.
Portland, Oregon
Merle Lawrence, Ph.D.
Ann Arbor, Michigan
Jerry Nort hem, Ph.D.
Denver. Colorado
George F. Reed, M.D.
Syracuse, New York
Robert E. Sandlin, Ph.D.
San Diego, California
Abraham Shulman. M.D.
New York, New York
Francis Sooy, M.D.
San Francisco, California
Harold G. Tabb, M.D.
New Orleans, Louisiana
BOARD OF DIRECTORS
Robert Hocks, Chairman
Portland, Oregon
Thomas Wissbaum, C.P.A.
Portland, Oregon
Gloria E. Reich, M.S.
Portl<ond. Oregon
Execu tivt! Director, Editor
HONORARY DIRECTORS
Del Clawson, House of Rep. Ret.
Downey, California
The Honorable Mark Hatfield
United States Senate
LEGAL COUNSEL
Henry C. Breilhaupt
Stoel, Rives, Boley, Fraser & Wyse
The American Tinnitus Association
Post Office Box 5
Portland, Oregon 97207
(503) 248-9985
ADDRESS CORRECTION REQUESTED
Non-Profit Organ.
U.S. Postage
PAID
Permi t No. 1 792
Portland, Oregon
Você também pode gostar
- Budwig Diet Guide Budwig Center PDFDocumento50 páginasBudwig Diet Guide Budwig Center PDFGeorgi Ana100% (3)
- FSFI Questionnaire Behind Addyi, The Female Sex PillDocumento4 páginasFSFI Questionnaire Behind Addyi, The Female Sex PillToronto StarAinda não há avaliações
- Couples in Treatment Techniques and Approaches For Effective Practice CompressDocumento350 páginasCouples in Treatment Techniques and Approaches For Effective Practice CompressŞterbeţ Ruxandra100% (4)
- (1984) History of Biological Effects and Medical Applications of Microwave EnergyDocumento19 páginas(1984) History of Biological Effects and Medical Applications of Microwave EnergyabhiAinda não há avaliações
- Dmso TinnitusDocumento7 páginasDmso TinnitusJoão FrancoAinda não há avaliações
- Virginia Henderson 14 Basic Human NeedsDocumento34 páginasVirginia Henderson 14 Basic Human NeedsJi GozelAinda não há avaliações
- Acute GastroenteritisDocumento56 páginasAcute Gastroenteritisneil052298% (46)
- Rife Handbook - 5th - Ed - TOC - & - IndexDocumento55 páginasRife Handbook - 5th - Ed - TOC - & - IndexRoo00733% (3)
- Tinnitus Today March 1982 Vol 7, No 1Documento8 páginasTinnitus Today March 1982 Vol 7, No 1American Tinnitus AssociationAinda não há avaliações
- Journal Reading: "Direct Current Stimulation of The Ear in Tinnitus Treatment: A Double-Blind Placebo-Controlled Study"Documento16 páginasJournal Reading: "Direct Current Stimulation of The Ear in Tinnitus Treatment: A Double-Blind Placebo-Controlled Study"Rully SyahrizalAinda não há avaliações
- 405 2013 Article 2849Documento8 páginas405 2013 Article 2849nisawidiyawardaniAinda não há avaliações
- Audio AnalgesiaDocumento7 páginasAudio AnalgesiaRisana RahoofAinda não há avaliações
- The Effect of Transcutaneous Electrical Nerve Stimulation (TENS) On Chronic Subjective TinnitusDocumento5 páginasThe Effect of Transcutaneous Electrical Nerve Stimulation (TENS) On Chronic Subjective TinnitusSameer AlladinAinda não há avaliações
- Neuroelectric TherapyDocumento23 páginasNeuroelectric TherapyNiklas LuwamAinda não há avaliações
- Acupuncture and Herbs Quiet TinnitusDocumento16 páginasAcupuncture and Herbs Quiet TinnitusNilesh RadeAinda não há avaliações
- 1 s2.0 S138824571500231X MainDocumento8 páginas1 s2.0 S138824571500231X MainTianyi ZhengAinda não há avaliações
- Knardahl 1998Documento7 páginasKnardahl 1998Nurul AzizahAinda não há avaliações
- Zeng 2004 Trends in Cochlear ImplantsDocumento34 páginasZeng 2004 Trends in Cochlear ImplantsAlex A.Ainda não há avaliações
- 1 s2.0 S0004951414610059 Main PDFDocumento10 páginas1 s2.0 S0004951414610059 Main PDFIkramul Hussain KhanAinda não há avaliações
- Berger Dobie Acoustictraumafromcontinuousnoise JASA2019Documento7 páginasBerger Dobie Acoustictraumafromcontinuousnoise JASA2019Herman FakoudAinda não há avaliações
- Outcomes of TinnitusDocumento6 páginasOutcomes of TinnitusmakifkilicAinda não há avaliações
- Tinnitus Today December 1986 Vol, 11, No 4Documento8 páginasTinnitus Today December 1986 Vol, 11, No 4American Tinnitus AssociationAinda não há avaliações
- Chronic TinnitusDocumento6 páginasChronic TinnitusThomasMáximoMancinelliRinaldoAinda não há avaliações
- Audioanalgesia As An Adjunct To Mobilization of The Chronic Frozen ShoulderDocumento8 páginasAudioanalgesia As An Adjunct To Mobilization of The Chronic Frozen ShoulderIntan Eddy ParindinganAinda não há avaliações
- The History of Microcurrent Stimulation PDFDocumento2 páginasThe History of Microcurrent Stimulation PDFjegm09100% (2)
- A Preliminary Study On The Efficacy and Safety of Low Level Light Therapy in The Management of Cochlear TinnitusDocumento6 páginasA Preliminary Study On The Efficacy and Safety of Low Level Light Therapy in The Management of Cochlear TinnitusTinnitus Man IndonesiaAinda não há avaliações
- The Leg Three Miles Acupuncture PointDocumento5 páginasThe Leg Three Miles Acupuncture Pointdoktormin106Ainda não há avaliações
- Electric Pulp Testing A Review J Lin & N P Chandler 2008Documento11 páginasElectric Pulp Testing A Review J Lin & N P Chandler 2008ABDUSSALAMAinda não há avaliações
- Transcutaneous Electrical Nerve Stimulation: Basic Science Mechanisms and Clinical EffectivenessDocumento13 páginasTranscutaneous Electrical Nerve Stimulation: Basic Science Mechanisms and Clinical Effectivenessninja-bookAinda não há avaliações
- Jastreboff2000-Tinnitus Retraining Therapy TRT As A Method For Treatment and Hyperacusis PatientsDocumento18 páginasJastreboff2000-Tinnitus Retraining Therapy TRT As A Method For Treatment and Hyperacusis PatientsEvans rizqanAinda não há avaliações
- Acoustic NeuromaDocumento4 páginasAcoustic NeuromaEmily AnnAinda não há avaliações
- Head 12650Documento8 páginasHead 12650josetelhadoAinda não há avaliações
- Electric Pulp Testing: A ReviewDocumento10 páginasElectric Pulp Testing: A ReviewWilliam BarrettAinda não há avaliações
- Electroconvulsive Therapy, Practice and Evidence: EditorialDocumento3 páginasElectroconvulsive Therapy, Practice and Evidence: EditorialIrmagian PaleonAinda não há avaliações
- Niemtzow Battlefield AcupunctureDocumento10 páginasNiemtzow Battlefield AcupunctureAruna BandaraAinda não há avaliações
- Electro DiagnosticsDocumento39 páginasElectro DiagnosticsGerson Ghese AltamiranoAinda não há avaliações
- A Uri Culo TherapyDocumento6 páginasA Uri Culo Therapyquirmche70Ainda não há avaliações
- NET Journal English Translation HEALING THROUGH ELECTRICITY?Documento5 páginasNET Journal English Translation HEALING THROUGH ELECTRICITY?heinz_toblerAinda não há avaliações
- E News Vol 3 Issue 2Documento16 páginasE News Vol 3 Issue 2Muhammad FahmyAinda não há avaliações
- E Stim PDFDocumento6 páginasE Stim PDFAlvaro Toledo100% (1)
- Electrical Stimulation at AuricularDocumento9 páginasElectrical Stimulation at AuricularshaukijameelAinda não há avaliações
- Abstract PRF and ApplicationDocumento1 páginaAbstract PRF and Applicationkuncupcupu1368Ainda não há avaliações
- Use of Magnetic Neurostimulator Appliance in Temporomandibular DisorderDocumento5 páginasUse of Magnetic Neurostimulator Appliance in Temporomandibular Disorderenfermeironilson6321Ainda não há avaliações
- E News Vol 3 Issue 1Documento16 páginasE News Vol 3 Issue 1Muhammad FahmyAinda não há avaliações
- Tinnitus Today September 1986 Vol 11, No 3Documento8 páginasTinnitus Today September 1986 Vol 11, No 3American Tinnitus AssociationAinda não há avaliações
- E News Vol 2 Issue 4Documento22 páginasE News Vol 2 Issue 4Muhammad FahmyAinda não há avaliações
- Transcutaneous Electrical Nerve Stimulation Basic ScienceDocumento13 páginasTranscutaneous Electrical Nerve Stimulation Basic ScienceMuhammad FahmyAinda não há avaliações
- TRT Tinnitus TreatmentDocumento16 páginasTRT Tinnitus TreatmentKarina CastroAinda não há avaliações
- Electro Stim FreqsDocumento10 páginasElectro Stim FreqsPuzzleMasterAinda não há avaliações
- RTMS For Chronic Tinnitus - Langguth, Lehner, Schecklmann - Summer '12Documento3 páginasRTMS For Chronic Tinnitus - Langguth, Lehner, Schecklmann - Summer '12American Tinnitus AssociationAinda não há avaliações
- Relief of Objective Tinnitus: Case StudyDocumento4 páginasRelief of Objective Tinnitus: Case StudyAmerican Tinnitus AssociationAinda não há avaliações
- Assessment of Patients For Treatment With Tinnitus Retraining Therapy (PDFDrive)Documento22 páginasAssessment of Patients For Treatment With Tinnitus Retraining Therapy (PDFDrive)Evans rizqanAinda não há avaliações
- The Basis For Micro Current Electrical Therapy in Conventional Medical PracticeDocumento10 páginasThe Basis For Micro Current Electrical Therapy in Conventional Medical PracticeFarouk AzzabiAinda não há avaliações
- ISMST GuidelinesDocumento112 páginasISMST GuidelinesDhrubo TaraAinda não há avaliações
- Bio Les Balancing ArticleDocumento4 páginasBio Les Balancing Articlegabriel1963Ainda não há avaliações
- Living The Field Energy Therapies by LynnMc TaggartDocumento95 páginasLiving The Field Energy Therapies by LynnMc Taggartxifaramaria96% (23)
- Electroconvulsive TherapyDocumento8 páginasElectroconvulsive TherapySimranjeet KaurAinda não há avaliações
- Effects of Electrical Stimulation in Early Bells Palsy On Facial Disability Index ScoresDocumento6 páginasEffects of Electrical Stimulation in Early Bells Palsy On Facial Disability Index Scorespriyanka banerjeeAinda não há avaliações
- The Vagus-Immune Connection: Harness Your Vagus Nerve to Manage Stress, Prevent Immune Dysregulation, and Avoid Chronic DiseaseNo EverandThe Vagus-Immune Connection: Harness Your Vagus Nerve to Manage Stress, Prevent Immune Dysregulation, and Avoid Chronic DiseaseAinda não há avaliações
- Hyperbaric Oxygen Therapy For The Treatment of Acute Cochlear Disorders and TinnitusDocumento2 páginasHyperbaric Oxygen Therapy For The Treatment of Acute Cochlear Disorders and TinnitusNur Syah Fitriyana RamadhaniAinda não há avaliações
- Schwannoma Vestibular TinnitusDocumento6 páginasSchwannoma Vestibular TinnitusThomasMáximoMancinelliRinaldoAinda não há avaliações
- Electroconvulsive Therap1Documento20 páginasElectroconvulsive Therap1Anonymous 83o62cAinda não há avaliações
- Extracorporeal Shockwave TherapyDocumento1 páginaExtracorporeal Shockwave Therapywr48f26rjmAinda não há avaliações
- TinitusDocumento4 páginasTinitusFridaZorayaAinda não há avaliações
- J Yebeh 2019 106551Documento6 páginasJ Yebeh 2019 106551Luisa Fernanda Lopez MoraAinda não há avaliações
- ATA Electronic Newsletter February 2012Documento8 páginasATA Electronic Newsletter February 2012American Tinnitus AssociationAinda não há avaliações
- ATA's 2012 Advocacy Accomplishments Inform 2013 Efforts With Congress - Outlaw - Winter '12Documento2 páginasATA's 2012 Advocacy Accomplishments Inform 2013 Efforts With Congress - Outlaw - Winter '12American Tinnitus AssociationAinda não há avaliações
- ATA Electronic Newsletter October 2011Documento7 páginasATA Electronic Newsletter October 2011American Tinnitus AssociationAinda não há avaliações
- ATA Electronic Newsletter October 2012Documento7 páginasATA Electronic Newsletter October 2012American Tinnitus AssociationAinda não há avaliações
- Scientists' Side of A Cure (Interview With Drs. de Ridder and Langguth) - Summer '12Documento2 páginasScientists' Side of A Cure (Interview With Drs. de Ridder and Langguth) - Summer '12American Tinnitus AssociationAinda não há avaliações
- MMF I&R Excerpt 2013 Jan 02Documento2 páginasMMF I&R Excerpt 2013 Jan 02American Tinnitus AssociationAinda não há avaliações
- ATA Electronic Newsletter June 2012Documento10 páginasATA Electronic Newsletter June 2012American Tinnitus AssociationAinda não há avaliações
- RTMS For Chronic Tinnitus - Langguth, Lehner, Schecklmann - Summer '12Documento3 páginasRTMS For Chronic Tinnitus - Langguth, Lehner, Schecklmann - Summer '12American Tinnitus AssociationAinda não há avaliações
- Tinitus PDFDocumento3 páginasTinitus PDFAtlerAinda não há avaliações
- FY 2011-2012 Annual Report - Winter '12Documento7 páginasFY 2011-2012 Annual Report - Winter '12American Tinnitus AssociationAinda não há avaliações
- Sound Therapy Can Be Very Effective For Treating Tinnitus - Jun, Rojas-Roncancio, Tyler - Winter' 12Documento3 páginasSound Therapy Can Be Very Effective For Treating Tinnitus - Jun, Rojas-Roncancio, Tyler - Winter' 12American Tinnitus AssociationAinda não há avaliações
- Tinnitus Information Sheet 2012Documento2 páginasTinnitus Information Sheet 2012American Tinnitus Association100% (1)
- Tinnitus Today September 2001 Vol 26, No 3Documento27 páginasTinnitus Today September 2001 Vol 26, No 3American Tinnitus AssociationAinda não há avaliações
- Facts About TinnitusDocumento2 páginasFacts About TinnitusAmerican Tinnitus AssociationAinda não há avaliações
- Tinnitus Today June 2000 Vol 25, No 2Documento26 páginasTinnitus Today June 2000 Vol 25, No 2American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today December 2000 Vol 25, No 4Documento27 páginasTinnitus Today December 2000 Vol 25, No 4American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today September 2000 Vol 25, No 3Documento27 páginasTinnitus Today September 2000 Vol 25, No 3American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today March 2001 Vol 26, No 1Documento28 páginasTinnitus Today March 2001 Vol 26, No 1American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today June 2001 Vol 26, No 2Documento27 páginasTinnitus Today June 2001 Vol 26, No 2American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today March 2000 Vol 25, No 1Documento28 páginasTinnitus Today March 2000 Vol 25, No 1American Tinnitus Association100% (1)
- Tinnitus Today December 1999 Vol 24, No 4Documento29 páginasTinnitus Today December 1999 Vol 24, No 4American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today September 1999 Vol 24, No 3Documento27 páginasTinnitus Today September 1999 Vol 24, No 3American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today March 1999 Vol 24, No 1Documento29 páginasTinnitus Today March 1999 Vol 24, No 1American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today September 1998 Vol 23, No 3Documento27 páginasTinnitus Today September 1998 Vol 23, No 3American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today December 1998 Vol 23, No 4Documento29 páginasTinnitus Today December 1998 Vol 23, No 4American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today June 1999 Vol 24, No 2Documento27 páginasTinnitus Today June 1999 Vol 24, No 2American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today June 1998 Vol 23, No 2Documento28 páginasTinnitus Today June 1998 Vol 23, No 2American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today March 1998 Vol 23, No 1Documento29 páginasTinnitus Today March 1998 Vol 23, No 1American Tinnitus Association100% (1)
- Tinnitus Today September 1997 Vol 22, No 3Documento31 páginasTinnitus Today September 1997 Vol 22, No 3American Tinnitus AssociationAinda não há avaliações
- Tinnitus Today March 1997 Vol 22, No 1Documento29 páginasTinnitus Today March 1997 Vol 22, No 1American Tinnitus AssociationAinda não há avaliações
- Little HansDocumento3 páginasLittle HansJC4REAL86Ainda não há avaliações
- EGDTDocumento33 páginasEGDTaLineLanAinda não há avaliações
- The Intentional Arc and Rationality in DepressionDocumento17 páginasThe Intentional Arc and Rationality in DepressionSyed Waliullah HussainiAinda não há avaliações
- Overall Strategy For Treatment of Critical Limb IschemiaDocumento83 páginasOverall Strategy For Treatment of Critical Limb IschemiaamurachAinda não há avaliações
- Tennis Elbow Lateral Epicondylitis - Orthoinfo - AaosDocumento5 páginasTennis Elbow Lateral Epicondylitis - Orthoinfo - Aaosapi-228773845Ainda não há avaliações
- How To Learn Homeopathy 1Documento3 páginasHow To Learn Homeopathy 1kayes82100% (1)
- Psychological Effects of Method ActingDocumento5 páginasPsychological Effects of Method ActingDisha T100% (1)
- A Guide To Crisis Intervention 5th Edition Kanel Test BankDocumento12 páginasA Guide To Crisis Intervention 5th Edition Kanel Test Bankmelaniehallwgrqkdtxic100% (48)
- Drug De-AddictionDocumento19 páginasDrug De-AddictionClaudia De Rosa0% (1)
- ACT: A Brief Intervention To Reduce ProcrastionDocumento14 páginasACT: A Brief Intervention To Reduce ProcrastionCamAinda não há avaliações
- International Journal of Surgery Open: Yophtahe Woldegerima Berhe, Amare Hailekiros Gebregzi, Nigussie Simeneh EndalewDocumento6 páginasInternational Journal of Surgery Open: Yophtahe Woldegerima Berhe, Amare Hailekiros Gebregzi, Nigussie Simeneh EndalewfaeAinda não há avaliações
- Oral HabitsDocumento78 páginasOral HabitsMrunali MaskeAinda não há avaliações
- Electrical Stimulation, Ultrasound, and Laser Light HandbookDocumento36 páginasElectrical Stimulation, Ultrasound, and Laser Light Handbookparji santosa100% (1)
- DMSCO Log Book Vol.6 7/1928-7/1929Documento111 páginasDMSCO Log Book Vol.6 7/1928-7/1929Des Moines University Archives and Rare Book RoomAinda não há avaliações
- BIOASSAYDocumento16 páginasBIOASSAYFree Escort ServiceAinda não há avaliações
- 2014 06 Manejo de Las Varices GastricasDocumento11 páginas2014 06 Manejo de Las Varices GastricasrafodocAinda não há avaliações
- IAL Textbook of Leprosy - Hemanta Kumar Kar and Bhushan KumarDocumento3 páginasIAL Textbook of Leprosy - Hemanta Kumar Kar and Bhushan KumarindraAinda não há avaliações
- 2017 10Documento200 páginas2017 10Eduardo RomeroAinda não há avaliações
- Walsall Medical PosterDocumento1 páginaWalsall Medical Posterlaur_rbAinda não há avaliações
- Acne Vulgaris: Basic Dermatology CurriculumDocumento58 páginasAcne Vulgaris: Basic Dermatology CurriculumJhoel Jhonatan Torres MuñozAinda não há avaliações
- Epstein1978 PDFDocumento13 páginasEpstein1978 PDFana rahmadaniAinda não há avaliações
- Abstracts: Brit. J. Vener. Dis. (1956), 32, 131Documento5 páginasAbstracts: Brit. J. Vener. Dis. (1956), 32, 131Shaashi DamodaranAinda não há avaliações
- Factors Affecting Bone Development, Growth, and RepairDocumento6 páginasFactors Affecting Bone Development, Growth, and RepairJoseph Arnold AlmonteAinda não há avaliações
- Anesthesia & Analgesia For Labor & DeliveryDocumento30 páginasAnesthesia & Analgesia For Labor & DeliveryPalwasha MalikAinda não há avaliações