Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Domain 3 Hayley Handout PDFDocumento9 páginasDomain 3 Hayley Handout PDFLenard DulansiAinda não há avaliações
- Anatomy of Female Reproductive SystemDocumento14 páginasAnatomy of Female Reproductive SystemkukadiyaAinda não há avaliações
- Success With Penile Prosthesis From Patient'S ViewpointDocumento3 páginasSuccess With Penile Prosthesis From Patient'S ViewpointJihad AnadAinda não há avaliações
- Cbse Class 8 Science Chapter 10 Reaching The Age of AdolescenceDocumento52 páginasCbse Class 8 Science Chapter 10 Reaching The Age of Adolescenceharshit kumarAinda não há avaliações
- Benefits and Risks of SterilizationDocumento29 páginasBenefits and Risks of Sterilizationvado_727Ainda não há avaliações
- Drosophila MelanogasterDocumento13 páginasDrosophila MelanogasterDavid MorganAinda não há avaliações
- Bab 5 f5Documento13 páginasBab 5 f5Ismaliza IshakAinda não há avaliações
- Quality of Postnatal Care ServicesDocumento10 páginasQuality of Postnatal Care Servicessaleha sultanaAinda não há avaliações
- Fertility InnDocumento15 páginasFertility Innkunnamon1234100% (2)
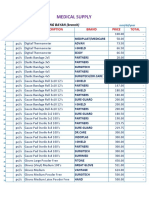
- Medical Supplies, & Baby Products PricelistDocumento5 páginasMedical Supplies, & Baby Products PricelistParmasya Ng Bayan Bacolor Main BranchAinda não há avaliações
- L The Importance of Emergency ContraceptionDocumento20 páginasL The Importance of Emergency ContraceptionAsma BegumAinda não há avaliações
- What Is The Male Reproductive SystemDocumento12 páginasWhat Is The Male Reproductive SystemDianne RuizAinda não há avaliações
- Breast Cancer KelseyDocumento12 páginasBreast Cancer Kelseyapi-3802092Ainda não há avaliações
- Pengaruh Pemberian Jus Jambu Biji Terhadap Kadar HB Pada Ibu Hamil Trimester Iii Di Polindes Krebet Kecamatan Bululawang Kabupaten MalangDocumento8 páginasPengaruh Pemberian Jus Jambu Biji Terhadap Kadar HB Pada Ibu Hamil Trimester Iii Di Polindes Krebet Kecamatan Bululawang Kabupaten MalangRosita Komala DewiAinda não há avaliações
- Genital FistulaeDocumento27 páginasGenital Fistulaeapi-3705046100% (1)
- Child and Adolescent Developmental StagesDocumento26 páginasChild and Adolescent Developmental StagesLaila PagdilaoAinda não há avaliações
- CDC - Fasciola - BiologyDocumento2 páginasCDC - Fasciola - BiologypecopecochanAinda não há avaliações
- Cephalopelvic DisproportionDocumento1 páginaCephalopelvic DisproportionWhinet Jojo TerunaAinda não há avaliações
- Faktor - Faktor Risiko Terjadinya Infertilitas Pada Wanita Pasangan Usia Subur Di Dusun V Desa Kolam Kecamatan Percut Sei Tuan Tahun 2020Documento6 páginasFaktor - Faktor Risiko Terjadinya Infertilitas Pada Wanita Pasangan Usia Subur Di Dusun V Desa Kolam Kecamatan Percut Sei Tuan Tahun 2020Anastasia AbrahamAinda não há avaliações
- Quantitative Morphological Changes in The Interplacentomal Wall of The Gravid Uterine Horn of Cattle During PregnancyDocumento8 páginasQuantitative Morphological Changes in The Interplacentomal Wall of The Gravid Uterine Horn of Cattle During PregnancyfeyisaAinda não há avaliações
- Organization of Maternity ServicesDocumento39 páginasOrganization of Maternity ServicesAnivasa KabirAinda não há avaliações
- SCIENCE FORM 3 Chapter 4 ExerciseDocumento7 páginasSCIENCE FORM 3 Chapter 4 ExerciseWan Shuhaimi Wan Ali100% (1)
- The Shakti Crystal Wand and Milking RitualDocumento8 páginasThe Shakti Crystal Wand and Milking RitualOana MicăAinda não há avaliações
- Jarvis 6th Ed - Chapter 26Documento4 páginasJarvis 6th Ed - Chapter 26edobleAinda não há avaliações
- Teen Pregnancy: Glorification Through Entertainment MediaDocumento5 páginasTeen Pregnancy: Glorification Through Entertainment MediaAshton TrumbleAinda não há avaliações
- 12 Biology - Reproductive HealthDocumento4 páginas12 Biology - Reproductive HealthTanya Mishra100% (1)
- A Guide To Semen Analysis: Information For PatientsDocumento8 páginasA Guide To Semen Analysis: Information For PatientsgalvigarciaAinda não há avaliações
- Intro To MycologyDocumento8 páginasIntro To Mycologycamille chuaAinda não há avaliações
- MDG Women ChildDocumento29 páginasMDG Women ChildevleopoldAinda não há avaliações
- Responsible ParenthoodDocumento21 páginasResponsible ParenthoodFrances Quibuyen DatuinAinda não há avaliações