Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocumento13 páginasOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- Cell PhysiologyDocumento61 páginasCell Physiologykiedd_04100% (4)
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Documento2 páginasIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04Ainda não há avaliações
- In The Book We Have Left Out Nothing: The Ethical Problem of The Existence of Verse 4:34 in The QuranDocumento11 páginasIn The Book We Have Left Out Nothing: The Ethical Problem of The Existence of Verse 4:34 in The Qurankiedd_04Ainda não há avaliações
- The Problems of Conscience and Hermeneutics: A Few Contemporary ApproachesDocumento15 páginasThe Problems of Conscience and Hermeneutics: A Few Contemporary Approacheskiedd_04Ainda não há avaliações
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocumento25 páginasFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04Ainda não há avaliações
- Matrix Table of Night Of Power (Arabic: لیلة القدر) 1430 Hijri, 2009Documento1 páginaMatrix Table of Night Of Power (Arabic: لیلة القدر) 1430 Hijri, 2009kiedd_04Ainda não há avaliações
- "Traditional" Exegeses of Q 4:34Documento15 páginas"Traditional" Exegeses of Q 4:34kiedd_04Ainda não há avaliações
- The Place For Others in IslamDocumento27 páginasThe Place For Others in Islamkiedd_04Ainda não há avaliações
- Nerve ExerciseDocumento2 páginasNerve Exercisekiedd_04Ainda não há avaliações
- Synaptic Transmission ExercisesDocumento1 páginaSynaptic Transmission Exerciseskiedd_04Ainda não há avaliações
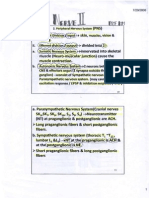
- Nerve Part IDocumento16 páginasNerve Part Ikiedd_04Ainda não há avaliações
- Nerve Part IIDocumento5 páginasNerve Part IIkiedd_04Ainda não há avaliações
- Blood (Part I)Documento54 páginasBlood (Part I)kiedd_04Ainda não há avaliações
- Blood (Part II)Documento68 páginasBlood (Part II)kiedd_04100% (1)
- Fadhilat Surah at TakwirDocumento1 páginaFadhilat Surah at Takwirkiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.9Documento1 páginaMicrobiology Colour Plate No.9kiedd_04Ainda não há avaliações
- Introduction To PhysiologyDocumento38 páginasIntroduction To Physiologykiedd_04Ainda não há avaliações
- SYNAPSEDocumento35 páginasSYNAPSEkiedd_04100% (3)
- Refleks ArcsDocumento34 páginasRefleks Arcskiedd_04100% (1)
- Microbiology Colour Plate No.5Documento1 páginaMicrobiology Colour Plate No.5kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.8Documento1 páginaMicrobiology Colour Plate No.8kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.7Documento1 páginaMicrobiology Colour Plate No.7kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.4Documento1 páginaMicrobiology Colour Plate No.4kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.1Documento1 páginaMicrobiology Colour Plate No.1kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.6Documento1 páginaMicrobiology Colour Plate No.6kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.2Documento1 páginaMicrobiology Colour Plate No.2kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.3Documento1 páginaMicrobiology Colour Plate No.3kiedd_04Ainda não há avaliações
- Vaccines (MFEB 3402)Documento17 páginasVaccines (MFEB 3402)kiedd_04Ainda não há avaliações
- Bacteria Classification & Structure (MFEB 3402)Documento12 páginasBacteria Classification & Structure (MFEB 3402)kiedd_04100% (1)
- Best 12 Weeks of Powerlifting All F'kin Year (Cast Iron Strength)Documento15 páginasBest 12 Weeks of Powerlifting All F'kin Year (Cast Iron Strength)Gustavo BelleiAinda não há avaliações
- Pulmonary Artery Wedge PressureDocumento2 páginasPulmonary Artery Wedge PressuresabaxlentAinda não há avaliações
- Behavior Analysis in Education Final.22Documento12 páginasBehavior Analysis in Education Final.22Bea Dimaun100% (1)
- FrancisD BUSN623 Week 7 Discussion What Is Your Ethical Framework 2 21 2021Documento7 páginasFrancisD BUSN623 Week 7 Discussion What Is Your Ethical Framework 2 21 2021Devona FrancisAinda não há avaliações
- Analysis of The Antitumor Activity of Bioactive Compounds of Cannabis Flowers Extracted by Green SolventsDocumento6 páginasAnalysis of The Antitumor Activity of Bioactive Compounds of Cannabis Flowers Extracted by Green SolventsJesusAinda não há avaliações
- C304 Task 1 Word A PDFDocumento33 páginasC304 Task 1 Word A PDFCamille Joy BaliliAinda não há avaliações
- MD3 Peer TutoringDocumento3 páginasMD3 Peer Tutoringdragtoss2Ainda não há avaliações
- Transparency of The National Government in COVIDDocumento6 páginasTransparency of The National Government in COVIDMariane NobleAinda não há avaliações
- Review On Chemical-Biological Applications of Thiazole Derivatives - 14!03!2020!04!58 - 10 - AmDocumento14 páginasReview On Chemical-Biological Applications of Thiazole Derivatives - 14!03!2020!04!58 - 10 - AmScientific Forefront JournalsAinda não há avaliações
- Bitter Melon Bioactive Composition and Health Benefits A Review - Tan Et Al. 2015Documento23 páginasBitter Melon Bioactive Composition and Health Benefits A Review - Tan Et Al. 2015Fatima HerreraAinda não há avaliações
- Shitnosis PDF EbookDocumento242 páginasShitnosis PDF EbookAlex William SmithAinda não há avaliações
- Wheat To FlourDocumento6 páginasWheat To Flourkumari shaliniAinda não há avaliações
- Final Project Therapeutic CloningDocumento8 páginasFinal Project Therapeutic Cloningsanjana andeAinda não há avaliações
- Swot Analysis: BERNARDO, Eleina Bea L. 11 Grade - Plato of Athens (ABM)Documento4 páginasSwot Analysis: BERNARDO, Eleina Bea L. 11 Grade - Plato of Athens (ABM)Eleina Bea BernardoAinda não há avaliações
- Bibliograhy-Tanishka MistryDocumento23 páginasBibliograhy-Tanishka Mistryapi-512047026Ainda não há avaliações
- Pestle Analysis On Reliance Industries: MBA Student - DBS Module International ManagementDocumento15 páginasPestle Analysis On Reliance Industries: MBA Student - DBS Module International ManagementshubhamAinda não há avaliações
- Biochemical Mechanism of Vitamin A in VisionDocumento3 páginasBiochemical Mechanism of Vitamin A in VisionAurelia HernandezAinda não há avaliações
- Mandibular Growth Anomalies - ObegweserDocumento450 páginasMandibular Growth Anomalies - ObegweserandresAinda não há avaliações
- Research Protocols and Clinical TrialsDocumento9 páginasResearch Protocols and Clinical TrialsMohammed GazoAinda não há avaliações
- Breast Cancer Cell LineDocumento34 páginasBreast Cancer Cell LineCatherine RajanAinda não há avaliações
- Resume For PortfolioDocumento2 páginasResume For Portfolioapi-546575413Ainda não há avaliações
- 744 FullDocumento16 páginas744 FullDaniela PopaAinda não há avaliações
- Master Thesis Product ManagementDocumento7 páginasMaster Thesis Product Managementjjvveqvcf100% (2)
- Name: Grace AGE: 28 Gender: Female Assessment Nursing Diagnosis Objectives Nursing Intervention Rationale Evaluation Subjective: GeneralDocumento2 páginasName: Grace AGE: 28 Gender: Female Assessment Nursing Diagnosis Objectives Nursing Intervention Rationale Evaluation Subjective: GeneralRainier IbarretaAinda não há avaliações
- MSC Counselling and PsychotherapyDocumento71 páginasMSC Counselling and PsychotherapyGenesis TallyacademyAinda não há avaliações
- Clinical Practice Pharmacy Policy and Procedure ManualDocumento11 páginasClinical Practice Pharmacy Policy and Procedure ManualStephanie Camille SamonteAinda não há avaliações
- Sample United States Navy Maintenance Requirement Card PDFDocumento3 páginasSample United States Navy Maintenance Requirement Card PDFInaamAinda não há avaliações
- Emotional Intelligence PresentationDocumento31 páginasEmotional Intelligence Presentationsweety100% (1)
- National Health Mission (NHM) : Kavita Singh, Director - FinanceDocumento64 páginasNational Health Mission (NHM) : Kavita Singh, Director - FinanceOWAIS ZAHOOR BHATAinda não há avaliações
- The Pursuit of Human Wellbeing 2017 PDFDocumento829 páginasThe Pursuit of Human Wellbeing 2017 PDFCSWCD Aklatan UP Diliman100% (1)