Você também pode gostar
- Snake Bite Management-2Documento102 páginasSnake Bite Management-2Manas DasAinda não há avaliações
- Snake BiteDocumento46 páginasSnake Bitejerly lAinda não há avaliações
- Snake Bite: DR - Vemuri ChaitanyaDocumento54 páginasSnake Bite: DR - Vemuri ChaitanyaMutiara YuliantikaAinda não há avaliações
- Snake Bite Injury: - PRESENTOR-Dr Varsha N Shetty - Moderator-Dr Nagaraj ShettyDocumento64 páginasSnake Bite Injury: - PRESENTOR-Dr Varsha N Shetty - Moderator-Dr Nagaraj ShettyDr. Apoorva KottaryAinda não há avaliações
- Snake Bite Medical ManagementDocumento35 páginasSnake Bite Medical Managementsyarifah nurlailaAinda não há avaliações
- Snake Bite: Abhija Babuji. Crri. Department of Pediatrics. SmimsDocumento76 páginasSnake Bite: Abhija Babuji. Crri. Department of Pediatrics. SmimsMeliani FranzAinda não há avaliações
- Snake Bite ManagementDocumento49 páginasSnake Bite ManagementIami MenotuAinda não há avaliações
- ThyroidDocumento20 páginasThyroidheartaoneAinda não há avaliações
- Hydrocarbon PoisoningDocumento10 páginasHydrocarbon PoisoningVarshith GandlaAinda não há avaliações
- SnakebiteDocumento54 páginasSnakebiteDimas Satrio BAinda não há avaliações
- Necrotizing EnterocolitisDocumento6 páginasNecrotizing EnterocolitisCharlie65129Ainda não há avaliações
- ExerciseDocumento2 páginasExercisenit_in10Ainda não há avaliações
- Keloid Treatment EvaluationDocumento136 páginasKeloid Treatment EvaluationMeilania HasnatashaAinda não há avaliações
- Osce Stations - Blogspot.com Paediatric Respiratory ExamDocumento2 páginasOsce Stations - Blogspot.com Paediatric Respiratory ExamrohitAinda não há avaliações
- Organophosphorus PoisoningDocumento14 páginasOrganophosphorus PoisoningSai KrishnaAinda não há avaliações
- Organophosphate PoisoningDocumento19 páginasOrganophosphate PoisoningPanda Kuma0% (1)
- Am-Pm BurnsDocumento1 páginaAm-Pm Burnsniraj_sdAinda não há avaliações
- S2 L7-8 Poisonous Plants of Sri Lanka Batch EditedDocumento48 páginasS2 L7-8 Poisonous Plants of Sri Lanka Batch EditedDr-Mirza Baig100% (1)
- Cwu - SurgeryDocumento10 páginasCwu - SurgeryThiviyaa SivaselvamAinda não há avaliações
- Paraquat PoisoningDocumento45 páginasParaquat PoisoningM. O. PHC HOLAVANAHALLYAinda não há avaliações
- PediatricsDocumento38 páginasPediatricskhanAinda não há avaliações
- National STI Guidelines 2014Documento80 páginasNational STI Guidelines 2014Raghu GhimireAinda não há avaliações
- Carbolic Acid & Oxalic AcidDocumento46 páginasCarbolic Acid & Oxalic AcidImteaz ahamadAinda não há avaliações
- Delirium in Critically IllDocumento37 páginasDelirium in Critically IllSanj.etcAinda não há avaliações
- AntihistaminesDocumento66 páginasAntihistaminesAfif Bastian100% (1)
- Management of Poisoning - Booklet PDFDocumento344 páginasManagement of Poisoning - Booklet PDFkrysteenAinda não há avaliações
- Pleural DiseasesDocumento4 páginasPleural DiseasesJennifer DayAinda não há avaliações
- 1.introduction To DermatologyDocumento57 páginas1.introduction To DermatologyMutasım Battah100% (2)
- Opioid Poisoning: by Dr. Daud Jabbar Taib Department of Forensic MedicineDocumento16 páginasOpioid Poisoning: by Dr. Daud Jabbar Taib Department of Forensic MedicineM KAinda não há avaliações
- PARAQUAT POISIONING 3rd Block Imed COMPLIEDDocumento15 páginasPARAQUAT POISIONING 3rd Block Imed COMPLIEDMohil PratapAinda não há avaliações
- MigraineDocumento9 páginasMigraineRose Athena SibalaAinda não há avaliações
- Introduction To Dermatology Assessment of A Dermatologic PatientDocumento86 páginasIntroduction To Dermatology Assessment of A Dermatologic PatientAtifAinda não há avaliações
- Snake BiteDocumento29 páginasSnake BiteIgbashioAinda não há avaliações
- General Management of PoisoningDocumento22 páginasGeneral Management of Poisoningranjithajay100% (1)
- Adrenergic Agonists 2020 PDFDocumento65 páginasAdrenergic Agonists 2020 PDFAlaa NaserAinda não há avaliações
- 5 - Differential Diagnosis of DermatologyDocumento6 páginas5 - Differential Diagnosis of DermatologyAyaa YousefAinda não há avaliações
- Spotting PSMDocumento60 páginasSpotting PSMAmanAinda não há avaliações
- ErythropoisisDocumento47 páginasErythropoisisDisha SuvarnaAinda não há avaliações
- Name: Bhanderi Akashkumar H. Clinical Clerk BCCM. ROTATION: OCT. 11-20, 2020Documento7 páginasName: Bhanderi Akashkumar H. Clinical Clerk BCCM. ROTATION: OCT. 11-20, 2020Venkatesh GarikapatiAinda não há avaliações
- Cutaneous TuberculosisDocumento78 páginasCutaneous TuberculosisDr Daulat Ram DhakedAinda não há avaliações
- Case Presentation CRUH FinalDocumento27 páginasCase Presentation CRUH FinalMatthew LeiAinda não há avaliações
- Organo Phosphate Poisoning by DR Gireesh Kumar K PDocumento16 páginasOrgano Phosphate Poisoning by DR Gireesh Kumar K PAETCM Emergency medicineAinda não há avaliações
- Degenerative Neurological DisordersDocumento61 páginasDegenerative Neurological DisordersMarites Santos AquinoAinda não há avaliações
- Dokumen - Pub Bedside Techniques Methods of Clinical Examination Fifth 2019nbsped 9789696375258Documento234 páginasDokumen - Pub Bedside Techniques Methods of Clinical Examination Fifth 2019nbsped 9789696375258doyoumatterindeedAinda não há avaliações
- Taenia SpeciesDocumento25 páginasTaenia SpeciesMark Arlo Hernandez SegundoAinda não há avaliações
- ALCIAN Blue Staining IMPDocumento4 páginasALCIAN Blue Staining IMPPallaval VeerabramhachariAinda não há avaliações
- Treatment of Psoriasis PDFDocumento187 páginasTreatment of Psoriasis PDFAngga SuryaAinda não há avaliações
- Anaphylaxis Shock: Bagian Anestesi FK UNISSULA SemarangDocumento15 páginasAnaphylaxis Shock: Bagian Anestesi FK UNISSULA SemarangTeguh PambudiAinda não há avaliações
- Sarcoidosis: Dr. Col. Vishal MarwahaDocumento26 páginasSarcoidosis: Dr. Col. Vishal MarwahaSreekrishnan TrikkurAinda não há avaliações
- 6 KG (Doubles) 65 6 KG (Doubles) 65: 6 Months 6 MonthsDocumento32 páginas6 KG (Doubles) 65 6 KG (Doubles) 65: 6 Months 6 MonthsskAinda não há avaliações
- PSORIASISDocumento27 páginasPSORIASISnurulzakinahnunu100% (1)
- Opioid Analgesics: Dr. Nisha.A.RDocumento93 páginasOpioid Analgesics: Dr. Nisha.A.RHassim M H SAinda não há avaliações
- Organophosphate PoisoningDocumento19 páginasOrganophosphate PoisoningapokawAinda não há avaliações
- DermatitisDocumento307 páginasDermatitisAbraham ChiuAinda não há avaliações
- Final Professional MBBS Annual Examination 2009Documento2 páginasFinal Professional MBBS Annual Examination 2009lovesyndromeAinda não há avaliações
- MUT17 Booklet 2Documento18 páginasMUT17 Booklet 2baang43farhanAinda não há avaliações
- Derm Pathology PDFDocumento21 páginasDerm Pathology PDFMara MitrutAinda não há avaliações
- Medicine Revision E6.5 (Medicalstudyzone - Com)Documento209 páginasMedicine Revision E6.5 (Medicalstudyzone - Com)Diya B johnAinda não há avaliações
- Cestode SDocumento38 páginasCestode SJang JangAinda não há avaliações
- Snakebites in Indonesia: Ribka TheodoraDocumento24 páginasSnakebites in Indonesia: Ribka TheodoraRibka TheodoraAinda não há avaliações
- CG en PDFDocumento335 páginasCG en PDFJessicaPaolaGutiérrezAranaAinda não há avaliações
- Unconscious PatientDocumento19 páginasUnconscious PatientChhabilal BastolaAinda não há avaliações
- 7 TH Semester Dermatology LecturesDocumento44 páginas7 TH Semester Dermatology LecturesChhabilal BastolaAinda não há avaliações
- Oxygen TherapyDocumento44 páginasOxygen TherapyChhabilal BastolaAinda não há avaliações
- 7 TH Semester Anesthesia LecturesDocumento35 páginas7 TH Semester Anesthesia LecturesChhabilal BastolaAinda não há avaliações
- Altered Sensorium and Care of Unconscious PatientsDocumento17 páginasAltered Sensorium and Care of Unconscious PatientsChhabilal BastolaAinda não há avaliações
- Opioids in AnaesthesiaDocumento28 páginasOpioids in AnaesthesiaChhabilal BastolaAinda não há avaliações
- Investigations For Thrombotic Tendencies - Australian Prescriber PDFDocumento6 páginasInvestigations For Thrombotic Tendencies - Australian Prescriber PDFChhabilal BastolaAinda não há avaliações
- Meningitis and Brain AbscessDocumento32 páginasMeningitis and Brain AbscessChhabilal BastolaAinda não há avaliações
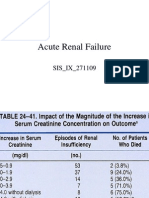
- Acute Renal FailureDocumento125 páginasAcute Renal FailureChhabilal BastolaAinda não há avaliações
- Dental Anatomy For MBBSDocumento33 páginasDental Anatomy For MBBSChhabilal BastolaAinda não há avaliações
- Emergency Drug Doses - PBS Doctor's Bag Items - Australian PrescriberDocumento4 páginasEmergency Drug Doses - PBS Doctor's Bag Items - Australian PrescriberChhabilal BastolaAinda não há avaliações
- ERC Guidelines 2005 Advanced Adult Life SupportDocumento48 páginasERC Guidelines 2005 Advanced Adult Life SupportJoãoBrasil100% (2)
- ChronicKidneyDisease IX Semseter MBBSDocumento38 páginasChronicKidneyDisease IX Semseter MBBSChhabilal BastolaAinda não há avaliações
- Kumj-Guideline For AuthorsDocumento6 páginasKumj-Guideline For AuthorsChhabilal BastolaAinda não há avaliações
- How - To - Read - Guitar TabDocumento29 páginasHow - To - Read - Guitar TabChhabilal Bastola100% (3)
- Resusgl 2010Documento157 páginasResusgl 2010Salman IslamAinda não há avaliações
- Laboratory Diagnosis of Coagulation DisordersDocumento59 páginasLaboratory Diagnosis of Coagulation DisordersChhabilal BastolaAinda não há avaliações
- Usmle LabsDocumento3 páginasUsmle LabsAdnan KhurshidAinda não há avaliações
- Wellness and Fitness Exercise ManualDocumento63 páginasWellness and Fitness Exercise ManualcienciaxAinda não há avaliações
- UsmleDocumento58 páginasUsmleFaisal Chukwudera Adam100% (1)
- 42 Deep Thought On Life, The Universe, and EverythingDocumento195 páginas42 Deep Thought On Life, The Universe, and EverythingHenry Ford100% (3)
- Step 3: Content Description and General InformationDocumento73 páginasStep 3: Content Description and General Informations1234321Ainda não há avaliações
- Im Yours Chords: by Jason MrazDocumento2 páginasIm Yours Chords: by Jason MrazChhabilal BastolaAinda não há avaliações
- Lyrics and Chords From UltimateDocumento2 páginasLyrics and Chords From UltimateChhabilal BastolaAinda não há avaliações
- 2010 Step 2 CKDocumento76 páginas2010 Step 2 CKandres ord100% (2)
- LyricsDocumento2 páginasLyricsChhabilal BastolaAinda não há avaliações
- Top 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalDocumento5 páginasTop 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalChhabilal BastolaAinda não há avaliações
- Top 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalDocumento5 páginasTop 100 QS World University Rankings For Medicine 2011 - Higher Education Network - Guardian ProfessionalChhabilal BastolaAinda não há avaliações
- Chicken PoxDocumento5 páginasChicken PoxYudith Iriani PalinggiAinda não há avaliações
- 86 Research Papers Supporting The Vaccine Autism LinkDocumento69 páginas86 Research Papers Supporting The Vaccine Autism LinkDanielPerez100% (1)
- Liver DiseasesDocumento29 páginasLiver DiseasesRicaneth TaanAinda não há avaliações
- Current Topics in Microbiology and ImunologyDocumento203 páginasCurrent Topics in Microbiology and ImunologyAndreea StanescuAinda não há avaliações
- Perlindungan Hak Anak Dalam Pelaksanaan Program Imunisasi Di Kabupaten Karanganyar (Kajian Kasus Penolakan Imunisasi Anak Di Kabupaten Karanganyar)Documento12 páginasPerlindungan Hak Anak Dalam Pelaksanaan Program Imunisasi Di Kabupaten Karanganyar (Kajian Kasus Penolakan Imunisasi Anak Di Kabupaten Karanganyar)SalsaAinda não há avaliações
- Chapter 2 MicroorganismsDocumento9 páginasChapter 2 MicroorganismsNIKHILPATNIAinda não há avaliações
- Infection and Modes of TransmissionDocumento14 páginasInfection and Modes of TransmissionLucky Radita Alma100% (1)
- Dengvaxia, Sanofi Pasteur's Dengue VaccineDocumento3 páginasDengvaxia, Sanofi Pasteur's Dengue VaccineshakiraAinda não há avaliações
- Virusolve TriggerDocumento3 páginasVirusolve TriggerFem CruzAinda não há avaliações
- Synflorix: What Is in This Leaflet?Documento3 páginasSynflorix: What Is in This Leaflet?A Nizar MasbukhinAinda não há avaliações
- Answers To Mike Adams's 21 Curious Questions About VaccinesDocumento32 páginasAnswers To Mike Adams's 21 Curious Questions About VaccinesLiz DitzAinda não há avaliações
- Mandarin TrifoldDocumento2 páginasMandarin TrifoldAlexander Edo TondasAinda não há avaliações
- MumpsDocumento19 páginasMumpsAmri RizalAinda não há avaliações
- Discursive EssayDocumento2 páginasDiscursive EssaySara100% (1)
- Lesson Plan On Theory.Documento12 páginasLesson Plan On Theory.Bhumi ChouhanAinda não há avaliações
- 0076 Tanushree Barua Assignment 1Documento3 páginas0076 Tanushree Barua Assignment 1AKSHAT SINGHAinda não há avaliações
- National Immunization Schedule: For InfantsDocumento2 páginasNational Immunization Schedule: For InfantsRahul DixitAinda não há avaliações
- Who-Laboratory Protocol For SalmonellaDocumento43 páginasWho-Laboratory Protocol For SalmonellaEvelyn ChumoAinda não há avaliações
- Patterns of Development III - Problem-Solution and PersuasionDocumento7 páginasPatterns of Development III - Problem-Solution and PersuasionRine CabusaoAinda não há avaliações
- This Is Not A Boarding Pass: Milan MalpensaDocumento13 páginasThis Is Not A Boarding Pass: Milan MalpensaEnida MataAinda não há avaliações
- Rabies QuestionDocumento4 páginasRabies QuestionRichardDumlaoAinda não há avaliações
- Emerging and Re-Emerging Bacterial Diseases in IndiaDocumento7 páginasEmerging and Re-Emerging Bacterial Diseases in IndiaPoorna ChandarAinda não há avaliações
- Lepto Spiros IsDocumento6 páginasLepto Spiros IsalvinbbAinda não há avaliações
- Introduction To Viruses - Wikipedia PDFDocumento80 páginasIntroduction To Viruses - Wikipedia PDFSaad-ullah SultanAinda não há avaliações
- 40 Años de Microbiología ClínicaDocumento6 páginas40 Años de Microbiología ClínicaDennis Lorena Cárdenas LealAinda não há avaliações
- GPA Maritime Declaration of Health Form v2 13.10.14Documento2 páginasGPA Maritime Declaration of Health Form v2 13.10.14Viorel AndreiAinda não há avaliações
- Immunology 1700s: Immunology and Serology Terminologies and Historical BackgroundDocumento3 páginasImmunology 1700s: Immunology and Serology Terminologies and Historical BackgroundLyka ReyesAinda não há avaliações
- Adult Combined Schedule VaccineDocumento33 páginasAdult Combined Schedule VaccinehatsuneAinda não há avaliações
- Modi Poster Row: Arrest Me Too, Rahul Dares Govt: Cyclone Rips Into Many StatesDocumento12 páginasModi Poster Row: Arrest Me Too, Rahul Dares Govt: Cyclone Rips Into Many StatesShah12Ainda não há avaliações
- DOH 210111 DM 2021 0047 Interim Guidelines On Masterlisting For The COVID 19 Electronic Immunization Registry CEIR Phase 1Documento9 páginasDOH 210111 DM 2021 0047 Interim Guidelines On Masterlisting For The COVID 19 Electronic Immunization Registry CEIR Phase 1kima conAinda não há avaliações