Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Place For Others in IslamDocumento27 páginasThe Place For Others in Islamkiedd_04Ainda não há avaliações
- "Traditional" Exegeses of Q 4:34Documento15 páginas"Traditional" Exegeses of Q 4:34kiedd_04Ainda não há avaliações
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Documento2 páginasIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04Ainda não há avaliações
- Refleks ArcsDocumento34 páginasRefleks Arcskiedd_04100% (1)
- SYNAPSEDocumento35 páginasSYNAPSEkiedd_04100% (3)
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocumento13 páginasOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocumento25 páginasFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.6Documento1 páginaMicrobiology Colour Plate No.6kiedd_04Ainda não há avaliações
- Cell PhysiologyDocumento61 páginasCell Physiologykiedd_04100% (4)
- Microbiology Colour Plate No.7Documento1 páginaMicrobiology Colour Plate No.7kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.5Documento1 páginaMicrobiology Colour Plate No.5kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.8Documento1 páginaMicrobiology Colour Plate No.8kiedd_04Ainda não há avaliações
- Fadhilat Surah at TakwirDocumento1 páginaFadhilat Surah at Takwirkiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.9Documento1 páginaMicrobiology Colour Plate No.9kiedd_04Ainda não há avaliações
- API® CoryneDocumento4 páginasAPI® Corynekiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.2Documento1 páginaMicrobiology Colour Plate No.2kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.1Documento1 páginaMicrobiology Colour Plate No.1kiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.4Documento1 páginaMicrobiology Colour Plate No.4kiedd_04Ainda não há avaliações
- Mitigation of Climate ChangeDocumento41 páginasMitigation of Climate Changekiedd_04Ainda não há avaliações
- Microbiology Colour Plate No.3Documento1 páginaMicrobiology Colour Plate No.3kiedd_04Ainda não há avaliações
- Advance Diagnostic Medical Laboratory: The AP 20E® For Identification of BacteriaDocumento1 páginaAdvance Diagnostic Medical Laboratory: The AP 20E® For Identification of Bacteriakiedd_04100% (1)
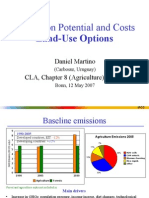
- Mitigation Potential and Costs Land-Use OptionsDocumento9 páginasMitigation Potential and Costs Land-Use Optionskiedd_04Ainda não há avaliações
- Diagram of Classification of EnterobacteriaDocumento1 páginaDiagram of Classification of Enterobacteriakiedd_04100% (1)
- Mitigation of Climate ChangeDocumento25 páginasMitigation of Climate Changekiedd_04Ainda não há avaliações
- Carnitine DeficiencyDocumento21 páginasCarnitine Deficiencykiedd_04100% (1)
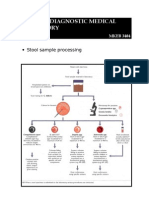
- Stool Sample ProcessingDocumento1 páginaStool Sample Processingkiedd_04Ainda não há avaliações
- Philosophical Consolation in Christianity and Islam Boethious and Al-KindiDocumento10 páginasPhilosophical Consolation in Christianity and Islam Boethious and Al-Kindikiedd_04Ainda não há avaliações
- Oxidase TestDocumento1 páginaOxidase Testkiedd_04100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- List of Steel Products Made in The UK PDFDocumento120 páginasList of Steel Products Made in The UK PDFAntonio MarrufoAinda não há avaliações
- A New Methodology For Determining The Moisture Diffusion Coefficient of Transformer Solid InsulationDocumento4 páginasA New Methodology For Determining The Moisture Diffusion Coefficient of Transformer Solid InsulationabetieAinda não há avaliações
- PHYSIO ReviewerDocumento3 páginasPHYSIO ReviewerPHILYP EPHRAIM PARANGALANAinda não há avaliações
- Unit Cells PDFDocumento3 páginasUnit Cells PDFel_tano33Ainda não há avaliações
- CHEM 141 Lab 3 (Stoichiometry) ProcedureDocumento5 páginasCHEM 141 Lab 3 (Stoichiometry) ProcedureKiersten RobertsAinda não há avaliações
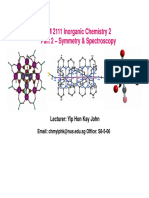
- CM 2111 Part 2 Lecture Notes 1Documento57 páginasCM 2111 Part 2 Lecture Notes 1Tan Yong KhaiAinda não há avaliações
- Product CatalogueDocumento16 páginasProduct CatalogueAsgerAinda não há avaliações
- Solar RefrigerationDocumento13 páginasSolar RefrigerationNivash RamAinda não há avaliações
- Book2 Wound Dressing GuideDocumento51 páginasBook2 Wound Dressing GuideBrian Niu100% (1)
- School of Maritime Studies Vels University Thalambur: Soda Acid Extinguisher AimDocumento2 páginasSchool of Maritime Studies Vels University Thalambur: Soda Acid Extinguisher AimAayush AgrawalAinda não há avaliações
- Us 4570540Documento3 páginasUs 4570540erwerAinda não há avaliações
- Centricast CL 1520 Data SheetDocumento6 páginasCentricast CL 1520 Data SheetOlmer Romero MendezAinda não há avaliações
- Exam 3 Review Sheet Chem 1601 F17Documento1 páginaExam 3 Review Sheet Chem 1601 F17RossAinda não há avaliações
- 5 Reflection High Energy Electron Diffraction (RHEED)Documento19 páginas5 Reflection High Energy Electron Diffraction (RHEED)Lương Hữu BắcAinda não há avaliações
- Chapter-6 Tissues-Full NotesDocumento12 páginasChapter-6 Tissues-Full NotesAdithya VinodAinda não há avaliações
- Watercut Monitors-Delta CDocumento8 páginasWatercut Monitors-Delta CShakeel AhmedAinda não há avaliações
- Barceloneta Landfill EPA Record of DecisionDocumento90 páginasBarceloneta Landfill EPA Record of DecisionRamon CardonaAinda não há avaliações
- Manual de Partes Cat 3507Documento4 páginasManual de Partes Cat 3507Julito Santa CruzAinda não há avaliações
- Workplace HazardsDocumento26 páginasWorkplace HazardsPageduesca RouelAinda não há avaliações
- Safety Data Sheet - Perfect Coat Flea & Tick Dog Shampoo PDFDocumento7 páginasSafety Data Sheet - Perfect Coat Flea & Tick Dog Shampoo PDFhoneybelAinda não há avaliações
- ID Senyawa Antibakteri Yang Diproduksi OlehDocumento8 páginasID Senyawa Antibakteri Yang Diproduksi OlehNurawaliah RezkyAinda não há avaliações
- Structural Composite Material. FinalDocumento43 páginasStructural Composite Material. Finalআলবার্ট হালদার100% (3)
- Determination of Total Carbohydrates by Anthrone MethodDocumento2 páginasDetermination of Total Carbohydrates by Anthrone MethodGuru Raj PNAinda não há avaliações
- Purestab Md1024: Technical Data SheetDocumento2 páginasPurestab Md1024: Technical Data SheetHadyan AdliAinda não há avaliações
- BS 1881-5 Testing ConcDocumento15 páginasBS 1881-5 Testing Conchz135874Ainda não há avaliações
- Unit 3 EM MCQDocumento21 páginasUnit 3 EM MCQPratik WakchoureAinda não há avaliações
- Omnova Coatings PresentationDocumento12 páginasOmnova Coatings PresentationNatalia Rodriguez100% (1)
- Iso 4260 1987 FR en PDFDocumento8 páginasIso 4260 1987 FR en PDFWilliam Orellana CarballoAinda não há avaliações
- TI-Polymer-Shrinkage in PlasticsDocumento6 páginasTI-Polymer-Shrinkage in PlasticsRadu Sorin MarinescuAinda não há avaliações
- MCAT Topic Focus Biology Electrophoresis and Blotting FSQ DrillDocumento1 páginaMCAT Topic Focus Biology Electrophoresis and Blotting FSQ DrillAnjalie GulatiAinda não há avaliações