Escolar Documentos
Profissional Documentos
Cultura Documentos
Diabetes MGT From Victorian Govt Dept (Janet Laverick)
Enviado por
vinayinscribdTítulo original
Direitos autorais
Formatos disponíveis
Compartilhar este documento
Compartilhar ou incorporar documento
Você considera este documento útil?
Este conteúdo é inapropriado?
Denunciar este documentoDireitos autorais:
Formatos disponíveis
Diabetes MGT From Victorian Govt Dept (Janet Laverick)
Enviado por
vinayinscribdDireitos autorais:
Formatos disponíveis
Improving Victorias oral health
May 2007
Diabetes self-management
Guidelines for providing services to people
newly diagnosed with Type 2 diabetes
March 2007
ii Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
Published by the Victorian Government Department
of Human Services
Melbourne, Victoria
Copyright State of Victoria 2007
This publication is copyright, no part may be reproduced by
any process except in accordance with the provisions of the
Copyright Act 1968.
This document may also be downloaded from the
Department of Human Services website at:
http://www.health.vic.gov.au/communityhealth/
publications/diabetes.htm
Authorised by the State Government of Victoria,
50 Lonsdale Street Melbourne.
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes iii
Foreword
In Australia, the burden of chronic disease is increasing
rapidly. In Victoria, approximately 70 per cent of the total
burden of disease is attributed to six groups: cardiovascular
disease, cancers, injuries, mental health conditions,
asthma and diabetes. As of 2001, approximately one million
Australians were diagnosed with Type 2 diabetes. A few
decades ago Type 2 diabetes was known as adult-onset
diabetes, mainly affecting older people. The prevalence of
Type 2 diabetes in younger people, including children and
adolescents, is increasing at an alarming rate and is linked
to increasing rates of obesity.
Victorias primary health care system must be able to
respond in an appropriate and cost-effective way to
this challenge. Self-management is about people being
actively involved in their health care. The approach has
been recognised by the Commonwealth Government and
the Victorian Government as a key component of chronic
disease management including diabetes.
The diabetes self-management funding is a component of
Victorias commitment under the Australian Better Health
Initiative (ABHI): a joint Australian, State and Territory
Government initiative. The funding will support early
intervention for people with high risk and newly diagnosed
with Type 2 diabetes to assist them to become an active
partner in the management of their health.
The diabetes self-management guidelines are aimed at
Primary Care Partnerships and their member agencies (in
particular community health services, rural health services
and Divisions of General Practice) to support the provision
of planned, managed, integrated and proactive care for
people with chronic disease. I encourage you to use the
guidelines to improve the health outcomes for people with
chronic disease.
Janet Laverick
Director Primary Health Branch
iv Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
Contents
Foreword iiii
1. Introduction 1
1.1 About the guidelines 1
1.2 The impact of diabetes 2
1.3 A coordinated approach to chronic disease 4
1.4 Overview of diabetes self-management funding 5
2. Chronic disease management 7
model for primary care
3. Diabetes self-management 9
service delivery
3.1 Client assessment and care planning 9
3.2 Self-management 11
3.3 Client monitoring 14
4. Diabetes self-management 16
supporting systems
4.1 GP liaison 16
4.2 Client recruitment and referral pathways 17
4.3 Clients with multiple chronic conditions
or complex needs 17
4.4 Decision support tools 18
4.5 Flexibility in service provision 18
4.6 Addressing health inequalities 19
5. Funding and reporting 21
5.1 Funding and reporting for CHSs 21
5.2 Funding and reporting for PCPs 21
5.3 Funding for workforce development 21
Appendix 1
A summary model of community
care through community health
services for people with
Type 2 diabetes 22
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 1
1.1 About the guidelines
Care for people with chronic disease, such as Type 2
diabetes, usually involves multiple health care providers in
multiple settings. To provide this care within an integrated
system, health care providers must work collaboratively
to coordinate and plan care and services. This requires a
commitment from health care providers and agencies to
work together to achieve shared goals.
People with Type 2 diabetes need a responsive person-
centred and effective system of care. These diabetes
self-management guidelines aim to support member
agencies of Primary Care Partnerships (PCPs), in particular
Community Health Services (CHSs), Rural Health Services
(RHSs) where applicable, and Divisions of General Practice
(DGP), to implement new diabetes self-management
funding in the context of a chronic disease management
(CDM) approach across the service system. The guidelines
also provide support for CHSs, PCPs and DGP as part of the
broader integrated chronic disease management (ICDM)
work. They should be used in conjunction with the Chronic
Disease Management Program Guidelines.
Self-management is about people being actively involved
in their health care. The approach is underpinned by a
number of principles
1
and has been recognised by the
Commonwealth Government and the Victorian Government
as a key component of diabetes management and CDM
more broadly.
Diabetes self-management funding supports work already
being undertaken by CHSs and PCPs. For example:
All PCPs now receive recurrent funding for ICDM which
builds on the established PCP role in facilitating service
system integration and change management across
member agencies.
Core business for CHSs includes providing services to
people in the community who have chronic disease.
Many CHSs, particularly those in receipt of Early
Intervention in Chronic Disease funding, are working
on internal systems changes to ensure services are
delivered within a CDM model of care.
1 ational Health Priority Action Council (HPAC) 2006, ational Health Priority Action Council (HPAC) 2006, National
Chronic Disease Strategy, Australian Government Department of
Health and Ageing, Canberra
1. Introduction
While these guidelines are targeted at CHSs (or RHSs where
applicable) and PCPs that receive direct funding (recurrent
for CHSs/RHSs and one-off funding for PCPs), they are also
intended to support agencies in their work with people who
have chronic disease.
The diabetes self-management guidelines should be used in
conjunction with:
Chronic Disease Management Program Guidelines
2
Primary Care Partnership Planning and Reporting
20062009 guidelines
3
Audiences
Community Health Services
funded under diabetes self-management
Funding provided to CHSs (or RHSs where applicable)
for diabetes self-management has been made available
to CHSs that are not in receipt of Early Intervention in
Chronic Disease funding. However, as stated in the Early
Intervention in Chronic Disease guidelines, the diabetes
self-management funding also builds on the work already
being done by CHSs and PCPs to support people in the
community who have chronic disease. Specifically, it
provides CHSs with additional funding to increase service
delivery to people with Type 2 diabetes, but also expects
that CHSs will work on internal systems changes to deliver
services that are consistent with evidence-based chronic
care. Refer section 5.1.
PCPs
PCPs have been provided with one-off funding to facilitate
service system integration and change management across
member agencies. In particular, general practice (through
DGP) and CHSs will need to be involved. Refer section 5.2.
Other agencies
Although funding for this initiative has been targeted to
CHSs, all CHSs see significant numbers of people with
chronic disease who would benefit from self-management
interventions and approaches. These guidelines could be
applied to other agencies wanting to develop and/or embed
self-management into practice.
2 http://www.health.vic.gov.au/communityhealth/downloads/
cdm_program_guidelines.pdf
3 http://www.health.vic.gov.au/pcps/strategy/index.htm#reporting
2 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
Rationale for self-management
There is a strong evidence base internationally for self-
management and a growing evidence base within the
Australian context. The most recent and largest initiative to
test self-management models within the Australian health
care system was the Australian Government funded Sharing
Health Care Initiative. The initiative included a series of eight
demonstration projects conducted over three years using
a range of models including the Stanford Model, Flinders
Model and Telephone Coaching. All eight projects found
that people reported improved health outcomes, a better
quality of life and reduced use of health services
4
. These
trends were also found in Indigenous and culturally and
linguistically diverse (CALD) client groups, which were part
of most projects.
The National Chronic Disease Strategy
5
outlines a number
of key directions for self-management which have been
built into these guidelines. Embedding self-management
principles has been identified as a key to maximising the
quality of life of people with a chronic disease and reducing
the risk of complications.
1.2 The impact of diabetes
Diabetes has an enormous impact on people, their families,
the community and the health system. It has been proven
that people with Type 2 diabetes have significantly lower
productivity and participation rates. The costs for Type 2
diabetes have been rising rapidly over recent years. The
Australian Institute of Health and Welfare projects
6
that
government expenditure on Type 2 diabetes will increase
by over 600 per cent between 2001 and 2031.
The facts on diabetes means the government must act
to ensure a strong focus on:
prevention of diabetes
early detection and intervention
quality service provision, including self-management
to prevent complications.
4 ational Evaluation of the Sharing Health Care Initiative: http://
www.health.gov.au/internet/wcms/publishing.nsf/Content/
chronicdisease-nateval
5 ational Health Priority Action Council (HPAC) 2006, ational
Chronic Disease Strategy, Australian Government Department of
Health and Ageing, Canberra
6 Australian Institute of Health and Welfare 2006, Australian Institute of Health and Welfare 2006, Australias Health
2006, Canberra
Diabetes the facts
7
Diabetes is a disease in which the body does not produce or
properly use insulin. Insulin is a hormone that is needed to
convert sugar, starches and other food into energy needed
for daily life. The cause of diabetes is unknown. Both family
history and lifestyle factors, such as obesity, poor diet and
lack of exercise, are risk factors. The major types of diabetes
are gestational diabetes, prediabetes, Type 1 diabetes and
Type 2 diabetes.
Gestational diabetes
8
Occurs during pregnancy and usually goes away after the
baby is born.
Affects 38 per cent of pregnant females.
Increases the risk of developing Type 2 diabetes later in
life with a 3050 per cent chance of developing Type 2
diabetes within 15 years of pregnancy.
Prediabetes
5
Occurs when a person's blood glucose levels are higher
than normal but not high enough for a diagnosis of Type 2
diabetes.
Many people live with prediabetes unaware of the
condition and its impact on their health.
Type 1 Diabetes
5
Affects 10-15 per cent of Australians with diabetes.
Is an autoimmune condition.
Results from the body's failure to produce insulin.
Type 2 Diabetes
6
In 2001, approximately one million Australians were
diagnosed as having Type 2 diabetes.
Up to 50 per cent of all cases remain undiagnosed.
Is largely a preventable chronic disease.
By 2031, it is projected 3.3 million will have Type 2
diabetes.
Increases two to five times the risk of having a heart
attack or stroke.
7 ational ReformAgenda, ational Reform Agenda, 2006: Victorias plan to address the growing
impact of obesity and type 2 diabetes, Consultation Draft, Council of
Australian Governments
8 Diabetes Australia, Diabetes Fact Sheets, viewed February 2007, Diabetes Australia, Diabetes Fact Sheets, viewed February 2007,
International Diabetes Institute Diabetes Research, Education and Care
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 3
Without adequate management a person with Type 2
diabetes is likely to develop complications such as renal
impairment and peripheral vascular disease.
Insulin is still produced by the pancreas, but is less
effective than normal. This is known as insulin resistance.
The prevalence of Type 2 diabetes in younger people,
including children and adolescents, is increasing at an
alarming rate. A few decades ago Type 2 diabetes was
known as adult-onset diabetes, mainly affecting older
people. The prevalence of Type 2 diabetes in children
and adolescents is linked to the increasing rates of obesity
in this group. Obesity rates for children aged 715 years,
based on studies conducted in 1985 and 1995, grew for
boys from 1.4 per cent to 4.5 per cent and grew for girls
from 1.2 to 5.3 per cent. It has been estimated that in
2004, 2025 per cent of children and adolescents were
overweight or obese.
9
Diabetes and chronic disease
in disadvantaged subgroups
The link between diabetes and an ageing population
and various subgroups within the population has been
recognised.
8
Subgroups include (but are not limited to):
Aboriginal and Torres Strait Islander communities
people from CALD backgrounds
rural and regional communities
people from lower socioeconomic groups.
These subgroups warrant attention to minimise the impact
of chronic disease on the individual, their family and the
broader community.
Aboriginal and Torres Strait Islander communities
Aboriginal and Torres Strait Islander communities have
particularly high rates of diabetes, with up to 30 per cent of
some communities being affected by diabetes. High levels
of ill health among Indigenous Australians
10,9
have been
linked to:
adverse socioeconomic conditions compared with general
Australian standards including lower incomes, poorer
educational outcomes and lower rates of home ownership
9 Australian Institute of Health and Welfare 2006, Australian Institute of Health and Welfare 2006, Australias Health
2006, Canberra
10 ational Public Health Partnership 2001, ational Public Health Partnership 2001, Eat Well Australia: An
Agenda for Action for Public Health Nutrition 20002010, Strategic
Inter-Governmental utrition Alliance, Canberra
http://www.nphp.gov.au/publications/signal/eatwell1.pdf
poor housing
exposure to violence
extent of control and perceptions of mastery in the
workplace and wider society
higher exposure to life stressors such as the death of
a family member or close friend, overcrowding at home,
alcohol and other drug problems, serious illness or
disability, and not being able to get a job
food insecurity.
Rural and regional communities
People living in rural and remote areas of Australia have
poorer health and higher levels of health risk factors
compared with those living in urban areas. This is despite
the perceived health advantages of living in rural areas
(clean air, less traffic, more relaxed lifestyle)
11
. Rurality itself
is not the main factor leading to poorer health among people
outside major cities. Factors associated with rurality are the
causes of comparative health disadvantage in those areas.
Such factors include:
socioeconomic disadvantage (including lower incomes
and education levels)
geographic isolation and difficulties with access to
health care
shortage of health care providers and services
greater exposure to injury
greater difficulties in transport and communications
sparsely distributed populations leading to diseconomies
of scale
insufficient supply of affordable and quality fresh food
unsupportive environment for physical activity.
Lower socioeconomic groups
Socioeconomic status (SES) is a strong predictor of
health. The lower a persons SES, the shorter his or her life
expectancy and the more prone he or she is to a wide range
of chronic diseases and conditions. Diabetes prevalence
is almost 2.5 times higher for the lowest SES groups. The
link between SES and health begins at birth and continues
through life. There is a strong, but indirect, association in
11 Australian Institute of Health and Welfare 2006, Chronic Diseases and
Associated Risk Factors in Australia, 2006, AIHW, Canberra, http://
www.aihw.gov.au/publications/phe/cdarfa06/cdarfa06.pdf
4 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
which SES affects health and health affects SES. Some
factors that can lead to SES effects on health
12,11
include:
differential access to high quality health care
individual factors such as smoking, exercise, nutrition,
stress and depression
social environments such as neighbourhood, work,
interpersonal support or conflict
violence and discrimination
long-term effects of prenatal and early childhood
environmental factors
structural factors that affect equitable access to food.
1.3 A coordinated approach
to chronic disease
A coordinated statewide response to diabetes is being
developed (currently out in draft for public comment)
13
and will be part of the ational Reform Agenda to address
the growing impact of chronic disease. Diabetes self-
management funding is one of many strategies that will
make up this statewide response. Strategies will be based
on evidence of what works and have a strong focus on
prevention, early detection and early intervention. Already
this focus has been given impetus by packages such as
the COAG Australian Better Health Initiative, of which this
funding is a part.
People with Type 2 diabetes require services from a broad
range of health care providers, are likely also to live with
other chronic conditions, and will use health services
throughout their life. Managing the burden of disease into
the future requires a robust health system that integrates
prevention and care over time and different stages of
disease, integrates the care of different conditions, and
integrates care across different services and service
providers.
12 ational Public Health Partnership 2001, Eat Well Australia: An
Agenda for Action for Public Health utrition 2000-2010, Strategic
Inter-Governmental utrition Alliance, Canberra http://www.nphp.
gov.au/publications/signal/eatwell1.pdf
11 Australian Institute of Health and Welfare 2006, Chronic Diseases and
Associated Risk Factors in Australia, 2006, AIHW, Canberra, http://
www.aihw.gov.au/publications/phe/cdarfa06/cdarfa06.pdf
13 National Reform Agenda: Victorias plan to address the growing
impact of obesity and type 2 diabetes, Consultation draft,
December 2006
The diabetes self-management funding is for the provision
of self-management interventions to high risk people newly
diagnosed with Type 2 diabetes. The services provided under
this funding should:
operate within a broader CHS CDM model
be linked to an ICDM approach across the local PCP.
Under the ICDM funding, PCPs have an important role in
bringing agencies together to develop systems that support
a coordinated approach to the planning and delivery of
services for people with chronic disease. PCPs are focusing
on service system integration over the next three years for
this client group by strengthening their service coordination
work. In particular, ICDM activities include:
strengthening referral systems to include regular feedback
and communication mechanisms that share service
outcomes between agencies, and between agencies and
general practice or between agencies and/or providers
developing clinical pathways for certain chronic diseases,
such as diabetes
supporting a self-management mapping process and
developing a plan to address gaps and facilitate workforce
development
developing inter-agency care planning models that
include and promote the participation of GPs, private
allied health practitioners and state-funded health
practitioners in multidisciplinary care through the Medical
Benefits Scheme (MBS) CDM items, such as Team Care
Arrangements.
These service system activities are essential in supporting
and helping to inform service delivery initiatives and
change management processes, such as diabetes self-
management.
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 5
Self-management mapping
The self-management mapping process is a PCP activity
that has strong links to diabetes self-management funding
and will inform future systems development for the initiative.
The information from the self-management mapping will be
invaluable to planning and developing the initiative.
Mapping data will assist PCPs and members to identify:
current gaps in the provision of self-management
interventions
workforce capacity and gaps
capacity vs. demand issues
referral pathways into self-management interventions.
This data will be key to PCP and members planning around
workforce development, coordinating the delivery of
self-management interventions across their catchment,
ensuring that interventions target high risk subgroups,
defining agency and general practice roles in providing self-
management interventions and support.
PCPs should prepare for this mapping process by identifying
agencies to be involved (state and Commonwealth funded,
public and private), conducting planning to ensure maximum
agency participation, and planning how the process can be
used for capacity building.
1.4 Overview of diabetes self-management
funding
The diabetes self-management funding is a component of
our commitment under the Australian Better Health Initiative
(ABHI): a joint Australian, State and Territory government
initiative. The initiative will provide early intervention to
people with high risk and newly diagnosed Type 2 diabetes
to support them to become good self managers of their
health. High risk includes subgroups of the community
that experience higher levels of chronic disease and find it
more difficult to access services. High risk groups include
Indigenous Australians, people from CALD backgrounds,
regional and rural communities, and those who experience
socio economic disadvantage.
It is important that people newly diagnosed with Type 2
diabetes have access to a range of services that are
well coordinated between health care providers. Early
intervention services should aim to provide:
information about diabetes and managing diabetes
assistance with monitoring and maintaining healthy
blood glucose levels
support for self-management (at an organisational and
clinical level)
information and assistance to manage lifestyle risks
links to community groups and programs that will support
lifestyle change
assistance to cope with the impacts of a long term
health condition
effective communication and referral between service
providers.
Early intervention services are best provided in the
primary care setting and delivered by a range of health
care providers, including GPs. The GP is the primary health
professional involved in detection and diagnosis and has
a central role in the ongoing medical management of the
disease. Allied health and nursing professionals have an
important role in providing education, self-management
support, foot care, lifestyle support (including dietary
management) and referral. The development of care plans
may be appropriate, through use of the MBS care planning
items, if the relevant criteria are met.
The diabetes self-management funding provides:
on-recurrent PCP funding in 200607 for work with
general practice (through DGP) to build on current activity
at the local level, focusing on people with chronic disease
and complex needs. While these funds need to be used to
ensure people newly diagnosed with Type 2 diabetes are
referred into self-management programs, they should also
support a broader approach to working with DGP, building
on existing effort as part of service coordination and ICDM.
on-recurrent funding in 200607 for staff training and
development, which will be managed by Department of
Human Services regions.
Recurrent CHS (or RHS where applicable) funding for
delivery of self-management interventions. Fourth quarter
targets only for 200607 and full year targets from 200708.
6 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
The funding has an emphasis on providing people with self-
management support that assists them and their families
(and/or carers) to gain the skills and resources to actively
manage their health. Effective client self-management is:
14
enhanced if started early
a key component of successful chronic disease
management
leads to improved health and wellbeing outcomes.
Self-management support goes beyond traditional
knowledge-based client education to include processes that
develop client problem-solving skills, improve self-efficacy,
and support application of knowledge in real-life situations
that matter to clients. Self-management is the ability of the
client to deal with all that a chronic disease entails, including
symptoms, treatment, physical and social consequences,
and lifestyle changes.
13
The funding for service delivery, in summary, should provide:
1. Client assessment.
2. Care planning (where this does not meet criteria for MBS
related care planning).
3. Self-management intervention.
4. Client monitoring.
These guidelines provide specific advice about service
delivery within each of these areas. This should build
on existing capacity to provide services to people with
diabetes. Funding should be used to address the gaps in
providing the services described in these guidelines.
Refer to section 5 for more funding information.
14 ational Health Priority Action Council (HPAC) 2006, ational Health Priority Action Council (HPAC) 2006, National
Chronic Disease Strategy, Australian Government Department of
Health and Ageing, Canberra
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 7
Core business for CHSs includes integrated population-
based health promotion initiatives and providing services
and programs to people with chronic disease, including
those with diabetes. Therefore, this funding and the
supporting diabetes self-management guidelines should add
value to existing services and programs involved in ICDM.
The diabetes self-management funding should operate
within a broader CHS CDM model that includes recognising
the importance of the interrelationships among individuals
and the social, cultural, environmental, behavioural and
biological factors that influence their health.
PCPs core activities include strengthening service
coordination systems across agencies for people with
chronic disease, with a focus on self-management, care
planning, and referral and communication mechanisms.
Key agencies involved in ICDM include CHSs and DGP.
Therefore, this funding should be integrated with and add
value to existing service system development across these
agencies and with general practice. Service coordination
work should align with the new Victorian Service
Coordination Practice Manual
15
which describes practice
standards for initial contact, initial needs identification,
assessment, care planning and referral.
To achieve this, the Primary Health Branch of the
Department of Human Services has adopted the Wagner
Chronic Care Model
16,17
for managing chronic disease in
the primary care setting. Wagner proposes that managing
chronic disease requires nothing less than a transformation
of health care, from a system that is essentially reactive
responding mainly when a person is sick to one that is
proactive and focused on keeping a person as healthy as
possible. The Chronic Care Model is a systems-based model
that summarises the essential elements for improving care in
health systems at the community, organisation, practice and
client levels. The model can be applied to a variety of chronic
diseases, health care settings and target populations.
15 http://www.health.vic.gov.au/pcps/publications/sc_pracmanual.htm
16 Improving chronic illness care: Improving chronic illness care:
http://www.improvingchroniccare.org/change/model/
components.html
17 Wagner E, Glasgow R, Davis C et al, 2001 uality Improvement in Wagner E, Glasgow R, Davis C et al, 2001 uality Improvement in
Chronic Illness Care: A collaborative Approach, Journal of Quality
Improvement, Volume 27 umber 2, February
Self-management is a key element in the model. The
elements are interdependent components, building upon
one another. Evidence-based principles under each
element, in combination, foster productive interactions
between informed clients and health care providers. As
its ultimate goal, the Chronic Care Model envisions an
informed, activated client interacting with a prepared,
proactive practice team, resulting in high quality, satisfying
encounters and improved outcomes. The Chronic Disease
Management Program Guidelines provide details of the
model in the context of CHS and PCP functions.
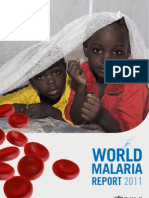
Table 1 provides examples of how diabetes self-
management can operate within a broader chronic care
model. This list is not exhaustive; it is provided to illustrate
the links and interdependence between the six elements
of the models. Local capacity, resources and requirements
will need to be considered in developing diabetes self-
management services.
2. Chronic disease management model for primary care
6 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
Table 1: Chronic Care Model examples
18
Health System
The Chronic Care Model
Community
Improved Outcomes
Self-
Management
Support
Delivery
Syst em
Design
Clinical
Informat ion
Syst ems
Decision
Support
Informed,
Act ivat ed
Pat ient
Effect ive
Self-Management
Prepared,
Proact ive
Pract ice Team
Productive
Interactions
Source: Wagner E, Glasgow et al 2001
The six eIements cf the mcdeI
Ccmmunity ExampIes
All staff have been trained and have access to Internet-based service directories which include community information.
Linkage to community programs (as appropriate) for people with diabetes and recorded on the care plan.
Self-management programs (including diabetes education program) include exercise sessions conducted at local leisure centres.
HeaIth system ExampIes
CHS strategic plan articulates a commitment and describes a plan to integrate funding (including diabetes self-management funding)
and provide a seamless and integrated chronic disease management (CDM) program.
Identification of clinical leaders to support staff.
Management and staff roles for planning, implementing and monitoring CDM are clearly defined.
Policies and procedure are in place that clearly support multidisciplinary teamwork and the diabetes team meets regularly.
SeIf-manaement suppcrt ExampIes
Self-management needs are routinely assessed for all clients with chronic disease including diabetes, using the Flinders Partners in
Health Scale (PIH)
18
or other identified tool.
All clients with sub optimal self-management skills are referred to self-management interventions (a range of interventions are available
depending on client need), clients with diabetes are offered a diabetes education group program or individual sessions (including face to
face and telephone contact).
DeIivery system desin ExampIes
A referral pathway to the CHS for diabetes care exists and is well known and used by GPs.
CHS nursing staff conduct assessment clinics every fortnight within two large local general practices; assessment clinics take referrals
for a range of programs.
GPs are available for case conferencing with CHS nurses (and other CHS staff via teleconference) for complex clients.
Follow up appointments between the GP and CHS for clients with chronic disease are coordinated.
Decisicn suppcrt ExampIes
Clients with chronic disease referred to the CHS are provided with a pocket size booklet to record their own health information
(developed through the CHS and DGP).
Diabetes guidelines and client handouts are evidence-based and sourced from Diabetes Australia.
Interagency care planning occurs for all clients with more than two chronic conditions (including diabetes) using the Service Coordination Plan,
coordinated by a key worker.
CIinicaI manaement systems ExampIes
Clinical indicator data collected by the GP is shared with the CHS following client consent.
Reports about CHS diabetes care are generated every 12 months and shared with GP practices, reports include no. of people: referred for service,
completing diabetes program, having a written care plan (with GP input), meeting lifestyle goals etc.
18 http://som.flinders.edu.au/FUSA/CCTU/Hand%20out%20Flinders%20Model%20June%202006.pdf
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 9
3. Diabetes self-management service delivery
Given the emphasis on an integrated approach to
delivering health services, CHSs in receipt of diabetes self-
management funding should use the funding to add value
to existing CDM programs by prioritising high risk clients
newly diagnosed with Type 2 diabetes. The initiative provides
CHSs with an opportunity to review their broader CDM
program and workforce capacity (in which the diabetes self-
management initiative should be embedded) to ensure it is:
based on evidence of what works
supported by systems (based on the Wagner Chronic Care
Model elements) that ensure best practice is routine
targeted at high risk clients who experience poorer health
and have difficulty accessing services.
The diabetes self-management funding builds on the
components of care that should be part of all CDM
programs, that is:
assessment
care planning
self-management interventions
linkage to community programs
client monitoring or follow-up.
Aspects of service delivery within these components will
vary depending on the chronic disease and on local service
models.
Therefore, the following describes the service delivery
requirements for high risk clients newly diagnosed with
Type 2 diabetes, without prescribing a model in which it is
to be implemented. The model should be determined at the
local level, to meet the needs of the local community and fit
within the local service system.
Agencies receiving diabetes self-management funding under
this initiative need to ensure the following service delivery
components are provided. A summary model of care is
provided at Appendix 1.
3.1 Client assessment and care planning
Assessment
All clients referred for a diabetes self-management service
must have access to a client assessment conducted by
an appropriately qualified health professional. A diabetes
assessment should include:
routine assessment procedures
taking anthropometric measurements
assessing knowledge and providing information
on diabetes
managing blood glucose levels
assessing lifestyle risk factors
assessing coping skills and social supports
screening for mental health issues.
Taking anthropometric measurements
Includes:
weight
body mass index (BMI)
waist circumference.
This provides the client and health professional with
baseline data from which changes over time can be
measured. Being overweight or obese is a leading risk factor
for Type 2 diabetes and most people diagnosed with the
disease are overweight. An American trial, The Diabetes
Prevention Program, studied people with prediabetes and
found that those who increased their physical activity most
days of the week and lost 5 to 7 per cent of their body
weight reduced their risk of developing diabetes by 58 per
cent. The Shape-Up test on the Diabetes Australia website
19
combines BMI and waist circumference to give clients an
idea of their risk for Type 2 diabetes. Although the tool is only
a guide aimed at healthy adults it can assist clients gain an
awareness of this risk factor.
The CHS and DGP should work together to establish a
process that ensures measurements are only taken by one
health professional and shared with the team (with client
consent). Often GPs collect this information, so CHSs
should not duplicate this assessment.
Assessing knowledge of diabetes
Includes:
assessing clients confidence and skills to manage
diabetes (self-efficacy).
Simply assessing knowledge is not enough because
knowledge does not necessarily equal behaviour change.
A client with a lot of knowledge may not put this knowledge
into practice. Assessment (that includes self-efficacy)
may be undertaken using a tool (such as the Flinders tools
Partners in Health Scale, Cue and Response) or through
a structured interview process. Self-efficacy has a greater
correlation with behaviour change. Clients should be asked
to rate how confidant they are to make changes based on
their knowledge.
19 http://www.diabetesnsw.com.au/diabetes_prevention_pages/
take_the_shape_up_test.asp
10 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
Managing blood glucose levels
Managing blood glucose levels is a very important
component of managing diabetes and should be done
together by the client, GP and other health professionals.
The GP may have started this process so the role of other
health professionals may be to assist the client to:
gain and use a home meter
understand hyperglycaemia and hypoglycaemia
understand use of insulin (if appropriate) and other
medication
access the ational Diabetes Services Scheme.
Assessing lifestyle risks
There is often a causal link between lifestyle risk factors
and Type 2 diabetes. Assessment of lifestyle risks can be
done through the use of a tool such as the GP lifestyle
script screening, based on the SAPW framework
(smoking, nutrition, alcohol consumption, physical activity,
weight management)
20
. Where lifestyle risks are identified
clients should be encouraged to set goals around
managing these risks.
Assessing coping skills
A persons support network and their ability to deal with
the emotional impacts of diabetes is important and will
impact on their ability to self-manage. We know that
effective self-management occurs in the context of strong
social connectedness. Good self-managers receive
support from their family, friends and/or community. It is
often psychosocial issues that limit self-management.
With training, health professionals without a professional
background in counselling can and should provide basic
psychosocial support. It is imperative that mechanisms are
in place to support health professionals in this role. This
is important as sadness, a sense of loss and other similar
emotions (that is not depression) are a normal experience
with chronic disease.
Although depression is not a recognised side effect of
diabetes, people with diabetes have a higher incidence of
depression. Certainly literature, such as the National Survey
on Mental Health and Wellbeing and the Victorian Burden of
20 http://www.health.gov.au/internet/wcms/publishing.nsf/
Content/health-pubhlth-strateg-lifescripts-index.htm
Disease
21
, states that people with chronic medical diseases
commonly experience depression and anxiety. Because of
this association, an awareness of and screening for mental
health issues is important. Studies show that undiagnosed
depression will make it harder for people to self-manage, for
example, take medications, eat properly and keep health
care appointments
22
. CHS staff should be aware that clients
with depression may be able to access private counsellors
under new MBS items for mental health, through GP referral.
Care planning
All clients referred for a diabetes self-management service
will require a care plan. Assessment outcomes identified
areas where further support is required. This will assist the
client and health professionals determine the plan of care.
Practice standards for care planning are described in the
new Victorian Service Coordination Practice Manual
23
.
The manual identifies three levels of care planning: service
specific care planning, intra-agency care planning and inter-
agency care planning. Care planning under this funding may
occur at all three levels. Service specific plans may include
a GP management plan, a self-management plan, and a
foot care plan. However, it will also be important to develop
models for intra-agency and inter-agency care planning
because medical management, allied health management
and self-management should be coordinated.
Clients with complex needs may also be eligible for a Team
Care Arrangement under the MBS-CDM items. For these
clients, it will be important that CHS staff provide input
into the care planning and coordination of services, with
the GP and, potentially, specialists and private allied health
professionals.
The care planning process should be a dynamic,
consultative process that includes the client (and family/
carers as appropriate) and health care providers, and meets
the clients health needs in a holistic way. Treatment options
should be provided so clients can make informed decisions
about their care. Goals and actions should be measurable
and articulate who is responsible, so that review and
reflection is possible.
21 http://www.health.vic.gov.au/healthstatus/bodvic/bod_current.
htm
22 University of Arkansas for Medical Sciences (UAMS), Depression
makes chronic diseases harder to handle, http://www.uams.edu/
today/2003/021003/chronic.htm
23 http://www.health.vic.gov.au/pcps/publications/sc_pracmanual.htm
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 11
Care plans should include the following elements:
issues/problems
goals, actions, target dates, responsible agents
regular review dates
participants
checklist evidence of need
method of planning.
Goal setting
Goal setting is an essential component of care planning
for people with chronic disease. It should follow a health
professional and client interaction that identifies problems
from the clients perspective, and barriers to making
change. Goal setting should involve the client setting short
term and long term goals. The goals should be realistic,
proposing behaviours that clients are confident they can
achieve. Confidence can be measured by asking the client
to estimate their confidence on a 0 to 10 scale that they
can achieve their goals. Experience shows that if the answer
is 7 or higher, the goals are likely to be achieved. If the
answer is below 7, the goals should be made more realistic
in order to avoid failure.
It is important that goals are client-centred, that is, they are
developed by the client and are relevant to the client. The
purpose of clients setting their own goals is to increase their
confidence in managing diabetes. Confidence fuels internal
motivation. Health professionals need to support clients to
do this initially. The Commonwealth Sharing Health Care
Initiatives 20012004, found that health professionals had
difficulty shifting their practice from a traditional medical
model of care to a client self-management focus which
included care planning where clients set personal goals
rather than health professionals setting clinical goals.
24
Goal setting support tools Flinders self-management
care plan and ACIC self-management support tool
25
are examples to guide discussion between the health
professional and client. The tools assist the health
professional and client to determine goals, identify steps to
24 ational Evaluation of the Sharing Health Care Initiative
Demonstration Projects 2005 http://www.health.gov.au/internet/
wcms/publishing.nsf/Content/chronicdisease-nateval
25 http://www.improvingchroniccare.org/tools/PDFs/self_mngmt_
support.pdf
achieve their goals, identify barriers to reaching their goals,
and plan for overcoming these barriers, including obtaining
needed resources.Goals for self-management should
include:
managing blood glucose levels
managing lifestyle risks
engaging in normal activities of daily life that are
important to the client.
Goals should be documented on the care plan.
3.2 Self-management
Self-management is described as
26
:
The client (and their family/carers as appropriate) working
in partnership with their health care provider to:
know their condition and various treatment options
negotiate a plan of care
engage in activities that protect and promote health
monitor and manage the symptoms and signs of the
condition(s)
manage the impact of the condition on physical
functioning, emotions and interpersonal relationships.
Self-management is the ability of the client to deal with all
that a chronic disease entails, including symptoms, treatment,
physical and social consequences, and lifestyle changes.
Self-management support
Self-management support is the care and encouragement
provided to people (and their family/carers as appropriate)
with chronic disease to help them understand their
central role in managing their conditions, making informed
decisions about care, and engaging in healthy behaviours.
Self-management support goes beyond traditional
knowledge-based client education to include processes that
develop client problem-solving skills, improve self-efficacy,
and support application of knowledge in real-life situations
that matter to clients.
26 http://som.flinders.edu.au/FUSA/CCTU/Hand%20out%20Flinders
%20Model%20June%202006.pdf
12 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
Good self-management support involves collaboration
between client and health care provider, where the
provider is coach as well as clinician and the client
and family are managers of daily care. It also includes
helping clients (and their family/carers as appropriate)
identify and achieve appropriate behavioural and lifestyle
changes. This often means identifying the attitudes and
beliefs that clients hold about their health, and addressing
the barriers to behaviour change.
As identified, self-management support should include family
and/or carers. Supporting behaviour change for individuals
may include supporting changes being made within a family.
For example, an individual who wants to make changes to
their diet may need support from family members who do the
food shopping and/or meal preparation.
Self-management interventions
Self-management interventions support and cover all
aspects of self-management as described above. While the
diabetes self-management funding should provide a range of
interventions that are flexible in content and delivery to suit
individual client needs and preferences, it is important that
interventions aim at achieving the following client outcomes:
engagement or re-engagement in life-fulfilling activities
engagement in health promoting behaviours and
reduction of lifestyle risks
learned skills and techniques to manage symptoms and
overcome health problems
a positive attitude to life and being able to live with the
disease without it controlling life
self-monitoring of clinical indicators, insight into living with
a health problem and setting realistic limitations
ability to confidently interact with health professionals and
use the health system appropriately
social engagement and the ability to seek support from
interpersonal relationships and community organisations
improved general emotional wellbeing
support client sustaining the lifestyle changes over the
longer term.
Table 2 illustrates the broad range of self-management
interventions that have been developed from one-on-
one interventions to group-based programs. This enables
interventions to be provided to suit the local capacity and
the needs of the client.
Table 2: Examples of self-management interventions
27
Individual
Population
Type of intervention Examples
Face-to-face
consultation
Flinders University model
of clinician-administered
support
Telephone coaching Coaching patients On
Achieving Cardiovascular
Health (COACH) program
Internet individual
course
ew South Wales Arthritis
Foundation course
Internet group course UK ational Health
Services
Expert Patients Program
online
Group: ongoing cycle Rehabilitation programs
Group: formal/
structured
Stanford University
program
Written information on-government
organisation publications
Television/multimedia,
social marketing
Back pain beliefs
campaign;
uit anti-smoking
campaign
Source: Joanne Jordan and Richard Osborne January 2007
Generic evidence-based self-management interventions
Includes:
Stanford Model
Flinders Model
motivational interviewing for behaviour change.
The most common behavioural models that underpin self-
management interventions
28
are the:
social learning theory that includes problem solving and
goal setting to improve self-efficacy
cognitive behavioural approach which aims to motivate
clients to adjust thought distortions that impact behaviour.
27 Jordan J and Osborne R 2007, Chronic Disease self-management
education programs: challenges ahead, Medical Journal of Australia,
Volume 186 umber 1, p. 1
28 Joanne Jordan, Joan ankervis, Caroline Brand and Richard Osborne
Chronic Disease self-management education programs: where should
Victoria go?, Final Technical Report 200506
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 13
Generic self-management models are appropriate for people
with diabetes; however, they need to be provided by an
appropriately qualified allied health professional (such as
a dietitian or physiotherapist) and combined with diabetes
education. The advantage of self-management interventions
that combine education with behavioural models is that they
build client knowledge as well as self-efficacy.
Stanford Model
Developed by Stanford University,
29
the model is a
structured group program that runs over six sessions for
people with arthritis or osteoporosis, or any chronic health
problem. Sessions are facilitated by two trained leaders
and cover:
techniques to deal with problems such as frustration,
fatigue, pain and isolation
appropriate exercise for maintaining and improving
strength, flexibility, and endurance
appropriate use of medications
communicating effectively with family, friends, and health
professionals
nutrition
how to evaluate new and alternative treatments.
Flinders Model
Developed by the Flinders Human Behaviour and Health
Research Unit,
30
the model is a generic set of tools and
processes. It enables clinicians and clients to undertake
a structured process that allows for assessment of self-
management behaviours, collaborative identification of
problems and goal setting, leading to the development of
individualised care plans. The tools include the Partners in
Health Scale, Cue and Response Interview, Problem and
Goals Assessment and Self-Management Care Plan.
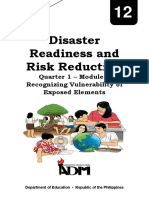
Motivational interviewing
Based on the Prochaska and Declemente Model, a cognitive
behavioural approach, motivational interviewing is a
counselling approach that prepares clients for behaviour
change. Using the technique, health professionals
encourage clients to identify lifestyle behaviours that they
would like to change and to articulate the benefits and
difficulties of making that change. The interviewer uses
directive questions and reflective listening to help clients
come to their own decisions by exploring their uncertainties.
29 http://patienteducation.stanford.edu/programs/
30 http://som.flinders.edu.au/FUSA/CCTU/Hand%20out%20Flinders
%20Model%20June%202006.pdf
This style of interview, asking the patient provocative
questions and discussing the responses, can often help
uncover important behaviour change issues.
Relapse Precontemplation
Determination/
preparation
Contemplation Maintenance
Action
Stages of Change Model
The Stages of Change Model identifies the stages
through which clients pass. The model is based on
the premise that behaviour change is a process, not
an event, and that individuals have varying degrees
of motivation or readiness to change. Motivational
interviewing has been proven effective in assisting
clients move through stages of change and preventing
relapse. Research has found that providing motivation is
much more successful
31
than simply providing clients
with knowledge.
Disease specific evidence based self-management
interventions
These interventions have been proven to be effective
through rigorous evaluation (for example, control group,
before and after time series) and have demonstrated
improved client outcomes.
In 2002, the Department of Human Services funded the
Hume Moreland PCP, through the Diabetes Prevention
and Management Initiative, to develop a lifestyle group
program for people with diabetes. The program, called One
Step Ahead, combines self-management support, exercise
and diabetes education. The program was implemented
in four health services and evaluated by The University of
Melbourne. Evaluation results showed that participants were
31 Bodenheimer T and Lorig K, Patient Self-management of Chronic
Disease in Primary Care, http://jama.ama-assn.org/cgi/content/
full/288/19/2469
14 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
highly satisfied with the program and client health outcomes
included improved self-reported physical activity levels and
statistical improvements in blood glucose control at six and
12 months post-program completion. A program manual
was developed out of the initiative along with a workforce
development strategy. The program manual describes:
the structure and content of the six session program
all necessary resources
information about conducting the program.
It is anticipated that both the program manual and
workforce development strategy will be available on the
Department of Human Services website in early 2007.
Under the diabetes self-management funding, it is expected
that self-management interventions will be provided to
clients over the period of approximately 12 months. This
may include a period of service intensity, for example, a
group program. However, intensity should step up or down
to regular but infrequent contact as clients support needs
change, for example, telephone contact every three months.
3.3 Client monitoring
A team approach to diabetes management starts with
the client and their GP, and adds allied health, specialist
and education services as required, particularly following
diagnosis. The diabetes self-management funding is aimed
at CHSs providing a range of services to people following
diagnosis and ensuring they have adequate supports in
place for long-term management. Therefore, it is important
that people with Type 2 diabetes have a regular GP. If not,
they should be supported to find a GP they trust. It is also
important that communication occurs between the CHS
and GPs of clients receiving services.
GP communication
Communication between the GP and other health care
providers is important to maintain the team approach to
care. Agreements and protocols around communication
between the GP and CHS should be established (if not
already in place) to ensure this occurs and should be
consistent with the practices, processes, protocols and
systems described in the Victorian Service Coordination
Practice Manual. Referral
32
and communication pathways
are also discussed in section 4. It is recommended that
the diabetes self-management guidelines be used in
conjunction with the manual.
32 http://www.health.vic.gov.au/pcps/coordination/ppps.htm
Communication agreements should be part of broader
ICDM inter-agency care planning models. Models may
vary in sophistication but should always be underpinned
by processes for sharing information and coordinating
care. For example, a basic level care planning model may
simply include sharing service specific care plans between
agencies. At a more sophisticated level, the model may
include discussion between health care providers from
different agencies around client goals which leads to
the development of one new coordinated care plan that
synthesises all information from service specific plans.
Following the package of services and self-management
support provided to clients, the CHS should take a step
down approach and communicate with the GP regarding
ongoing management. A step down approach may include
one or more of the following options:
The client exiting from service with an opportunity for
re-contact should other issues arise or through invitation
to additional or refresher diabetes self-management
programs.
Annual podiatry appointments.
Ongoing but infrequent telephone coaching.
Ongoing management
As well as self-management interventions, clients may
require allied health (for example, podiatry, dietetics),
nursing and/or counselling services. Clients should be
assisted to access these services via appropriate referral.
These services may or may not be funded directly by the
diabetes self-management funding, and may or may not be
provided by the CHS, depending on how funding is used
and what services outside the CHS are more appropriate
(such as MBS funded allied health and dental).
Clients should also be educated about, and linked to, other
health and community services that can provide routine
ongoing care and support. Ideally, as part of an annual cycle
of care (sourced from the Australian Government Health and
Ageing website Medicare online), the GP will facilitate the
following:
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 15
Other important health care checks include:
33
a dental check up
a foot assessment by a podiatrist
an eye examination for retinopathy by an eye specialist/
ophthalmologist or experienced optometrist.
Clients should have a good relationship with their GP and
be linked into services prior to exiting the CHS. Services
may include MBS funded allied health, dental and/or
counselling.
Lifestyle modification
A healthy lifestyle for people with diabetes means enjoying
healthy eating, maintaining a healthy weight, being
physically active, learning to manage stress and thinking
positively. Where lifestyle risks exist, support for lifestyle
modification is important. Best practice guidelines for
people with diabetes (as per the International Diabetes
Institute
34
) include:
cessation of smoking
alcohol intake of 2 standard drinks/day for men and
1 standard drink/day for women
a healthy diet that includes reducing saturated fat and
ensuring carbohydrates are low in glycaemia index and
high in fibre
33 http://www9.health.gov.au/mbs/fullDisplay.cfm?type=note&q=A.2
9&qt=oteID
34 http://www.diabetes.com.au/living.php?regionID=52&page=overview
at least 30 minutes of moderate physical activity on most,
preferably all, days.
There are many programs and supports provided by
community organisations and peak bodies, or available on
the Internet, that can assist people make lifestyle changes.
Providing clients with support for lifestyle modification will
require up skilling staff to:
provide support where appropriate
make referrals or assist client to make links with these
programs and supports.
Community linkages
Community programs, networks and clubs can often provide
people with diabetes the support necessary to assist
them maintain a healthy lifestyle. Community programs
include strength training programs at neighbourhood
houses, Weight Watchers groups, yoga classes, church
networks. The list is endless and the health system must
learn to make the most of such resources. Many PCPs
have been involved in supporting electronic records that
include such information. Health care providers should
discuss possibilities with their clients. Helping clients
gain support from their community to make and maintain
lifestyle changes is very important. Care plans may include
facilitating referrals or supporting clients to make links with
community programs.
Table 3: Diabetes Annual Cycle of Care
33
Assess diabetes control by measuring HbA1c At least once every year
Ensure that a comprehensive eye examination is carried out At least once every two years
Measure weight and height and calculate BMI At least twice every cycle of care
Measure blood pressure At least twice every cycle of care
Examine feet At least twice every cycle of care
Measure fat profile (lipids), including HDL (good cholesterol), LDL
(bad cholesterol), total cholesterol and triglycerides
At least once every year
Test for microalbuminuria (protein levels in urine for indications
of early kidney damage)
At least once every year
Provide self-care education Patient education regarding diabetes management
Review diet Reinforce information about appropriate dietary choices
Review levels of physical activity Reinforce information about appropriate levels of physical activity
Check smoking status Encourage cessation of smoking (if relevant)
Review medication Medication review
16 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
The evidence for a systems approach to embedding ICDM is
overwhelming. The Sharing Health Care Initiative found that
projects best able to meet the challenges of implementing
self-management into the community
35
:
were organisationally mature, with good infrastructure and
support, including organisational and clinical leadership
supporting self-management
had strong relationships with key stakeholders (for
example, community groups and DGP)
established or capitalised on pre-existing relationships
with a range of health service providers including GPs
were flexible in their approach and design and able to
respond to client feedback
employed a variety of approaches to recruitment and
implementation, depending on the target group
built capacity from an organisational perspective,
most notably in the areas of network partnerships and
knowledge transfer.
4.1 GP liaison
Allocation of non-recurrent funds
DGP are key PCP member agencies and have considerable
expertise in communicating with, and advocating on behalf
of, GPs. Therefore, it is expected that the PCP will work with
the local DGP to develop a work plan that builds on existing
GP liaison activity to ensure that referral pathways between
GPs, the CHS and other relevant services are in place to
support the diabetes self-management initiative. The non-
recurrent funding should support PCP activity on ICDM. The
delivery of the work plan should be negotiated between the
PCP and DGP and could include funds allocation to the DGP
to support delivery of some or all of the outcomes against
the work plan.
The work plan should include effective strategies for:
informing GPs and their staff about the diabetes services
and programs delivered by the CHS
encouraging GPs to systematically refer patients with
newly diagnosed diabetes
sharing patient information between the general practice
and CHS, and effectively communicating with GPs
35 ational Evaluation of the Sharing Health Care Initiative:
http://www.health.gov.au/internet/wcms/publishing.nsf/
Content/chronicdisease-nateval
developing care plans aligned with MBS guidelines, with
appropriate participation of the CHS and other relevant
agencies, with GPs and, potentially, private allied health
services, in care plans aligned with MBS guidelines.
GP liaison activity
GP liaison activity for this initiative should be consolidated
with broader CDM GP liaison activity, to ensure consistent
systems are established between GPs and the CHS.
This will require strong DGP leadership in the design
and implementation of systems to support coordinated
chronic care that includes GPs as referrers, providers of
medical perspectives in care plans and key members of
multidisciplinary care teams. CHSs are encouraged to work
with their local DGP to develop an agreed plan for building
on existing capacity for liaison with general practice and
further embedding ICDM systems.
GP liaison activity could include:
canvassing GP views and awareness of CHS
providing input into the development of CHS resources for
GPs and their clients
supporting practice staff to make appropriate referrals
(practice staff visits to the CHS or CHS visits to practices)
encouraging GPs to support their clients attending self-
management programs
establishing appropriate systems that meet the needs of
clients and GPs.
Flexibility and innovation should be used in the development
of systems to ensure general practice involvement with the
CHS in delivering diabetes care. Most importantly, systems
need to work for the people they service. For example,
where accessibility is an issue, the CHS may negotiate
with a large general practice to conduct group programs
for their clients within the practice on a day that clients are
also booked for appointments with their GP. To facilitate
coordinated care planning, the CHS may establish an
agreement with a practice to conduct assessment clinics
(carried out by a CHS nurse) within the practice and provide
input into care planning and case conferences.
4. Diabetes self-management supporting systems
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 17
Establishing systems to identify appropriate clients to be
referred from the GP to the CHS will include discussion
about clients who are eligible for Team Care Arrangements
and MBS funded allied health. The DGP (and potentially
GP representatives) should be involved in making
recommendations about a local model that provides for both
these scenarios.
4.2 Client recruitment and referral
pathways
Experience has shown that client recruitment into self-
management programs is most effective when health
professionals facilitate the referral. Often the health
professional with the greatest influence is the GP. Therefore,
it is important that client recruitment and referral pathways
developed as part of chronic disease care, particularly
diabetes care, include self-management interventions as
routine and are offered to all clients and family/carers by
their health care providers.
In a recent study in Victoria, it was found that, in general,
poor recruitment of clients into self-management
interventions is due to poor engagement with health
professionals for the following reasons:
36
They have not been well informed.
They are uncertain about the benefits for their clients.
They lack a structured or uniform process to refer their
clients.
They need hard evidence relating to the outcomes for
their clients or at least outcomes at a local level.
The report recommends that a whole of system approach
be taken to planning and implementing self-management
interventions. This includes establishing standard referral
pathways, communication pathways within and between
health sectors for client self-management referral, feedback
and continuity of care processes, and promotion/marketing
strategies that include educating health professionals in the
benefits and importance of self-management interventions.
Referral pathways should be underpinned by the Service
Coordination strategy and include quality information
sharing, feedback and agreed response times. Recruitment
criteria should be clearly defined and become part of initial
needs identification, which involves screening of client
needs, determining access and priority, and assessing risk.
36 Jordan, ankervis, Brand & Osborne (2006), Jordan, ankervis, Brand & Osborne (2006), Chronic Disease Self-
management Education Programs Where Should Victoria Go? Final
Technical Report
It is expected that GPs will be a primary source of referral
for CHS diabetes self-management programs. Therefore, the
DGP will be key to developing clear pathways and supporting
general practice referrals. DGP should encourage the use of
the Statewide Referral Tool for GP referrals.
CHSs should consider strategies to ensure that high risk
clients are recruited into the program, particularly those
who have difficulty accessing services due to geographic
location, ethnicity, language barriers, limited literacy levels
or who lack the confidence to be good self-managers of their
own health care. Transport for clients in rural and regional
areas is often reported to be a major barrier in accessing
health services and programs. CHSs could play a role in
assisting clients overcome these barriers with strategies
such as facilitating car pooling, organising volunteer
transport, conducting programs offsite in more accessible
venues (such as church halls, club halls).
4.3 Clients with multiple chronic
conditions or complex needs
It is not uncommon for people with diabetes to be diagnosed
with other chronic conditions and/or have complex needs.
Clients with multiple chronic conditions and/or complex
needs may benefit from a key worker whose role would
include:
coordinating service specific assessments and other
assessments as required
ensuring that a coordinated (inter-agency) care plan is
developed, monitored and reviewed
being involved in a Team Care Arrangement (as
appropriate)
communicating and liaising (including service outcome
communication) with other health care providers
(including GP and private allied health providers)
coordinating a multidisciplinary case conference (as
appropriate)
being a contact for the client should their condition
deteriorate and/or circumstances change that may
impact on the management of their diabetes
providing support for carers (as appropriate)
making referrals to community-based activities (as
appropriate)
taking a flexible approach to ongoing follow up
following up clients who drop out of the program.
16 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
At a minimum, the key worker should have contact with the
client at three months, six months and 12 months as part of
the client monitoring phase.
CHSs should work closely with the DGP to ensure that
clients who may be eligible for allied health services through
the MBS-CDM items have access to these services and that
service duplication does not occur. The MBS-CDM items
include:
preparation and review of a GP Management Plan
coordination and review of Team Care Arrangements
contribution to a multidisciplinary care plan being
prepared by another health or care provider.
37
4.4 Decision support tools
Decision support includes:
supporting practitioners to deliver best practice care
using resources, tools and best practice guidelines
supporting clients to make decisions about their own
health and health care behaviour.
Decision support tools are becoming more common in
health care and can take a variety of formats, such as
printed guidelines, Internet supports, computer software
programs (IPPS is an example of a decision support tool
for program planning), and decision algorithms (for example,
a risk rating tool for diabetes). Health care providers should
use evidence-based tools to support them to deliver best
practice diabetes care. These are best sourced from peak
bodies, such as Diabetes Australia Victoria and International
Diabetes Institute. It is important that clients receive
consistent messages from all their health care providers and
this can only be achieved through:
embedding evidence-based guidelines into daily clinical
practice
sharing evidence-based guidelines and information with
clients to encourage their participation
using proven provider education methods.
An example of a decision support tool is the commonly
used stoplight analogy to teach clients about monitoring
and managing their chronic condition. Many providers
suggest that a copy of this document is kept by the client
in a prominent place (for example, at home or work).
37 Commonwealth Department of Health and Ageing, Commonwealth Department of Health and Ageing,
www.health.gov.au/internet/wcms/publishing.nsf/Content/
pcd-programs-epc-chronicdisease
Red
Stop to assess
ellow ellow
Caution in planning
Green Green
Go to action
The stoplight tool divides various signs and
symptoms (for example, daily blood glucose levels)
into green, yellow and red management zones.
Green indicates stability and good control over the
condition, yellow indicates caution and suggests
steps for regaining control, and red indicates a
medical crisis that requires a providers attention.
Effective use of tools in the management of diabetes can
empower health care providers to make good clinical
judgments, involve clients in self-management, and provide
timely and efficient care, all of which contribute to improved
outcomes.
It may be appropriate for the CHS to work with the PCP to
develop a decision support tool to be used by numerous
member agencies. For example, this is relevant where a local
diabetes risk or triage tool is required to ensure that clients get
the right care, at the right time by the right service provider
(which may be the CHS, GP, RDS, HARP). Some PCPs have
already done this work and are willing to share their learnings,
in particular the tools that they have developed.
Refer Chronic Disease Management Program Guidelines.
4.5 Flexibility in service provision
To ensure diabetes services and program respond to the
needs of local communities and individuals, flexibility must
be built into the design of these services and programs.
For example, it is likely that people newly diagnosed with
Type 2 diabetes will include middle age adults still working.
Therefore, after hours services and programs (including
week nights and/or weekends) should be offered.
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 19
Flexible approaches to self-management
interventions
Self-management interventions must take into account that:
ot all people respond well to group programs, due to
issues of culture, language, education and preference.
Therefore, individual appointments should be offered
where group programs are not appropriate.
Group programs are appropriate for some Indigenous
and CALD communities, however programs need to
be reviewed and modified to ensure they are culturally
appropriate. Where clients are literate in their own
language, translated written materials may be appropriate,
otherwise different approaches are required.
Cultural differences in definitions of health and
expectations around health care behaviours impact on
self-management, so interventions must be sensitive to
these differences and explore meanings around living a
healthy life.
Running group programs in rural settings may require
running groups with smaller numbers and running groups
for people with a variety of diagnoses.
Individual appointments can take a range of forms
based on need, for example, one-on-one appointments,
telephone coaching, Internet support.
It should also be recognised that the term self-management
is a fairly new concept and is not well understood outside of
the health workforce. Therefore, careful planning should be
taken to market these interventions. Involving community
and consumer representatives in planning recruitment and
marketing strategies and developing resource materials will
be important.
4.6 Addressing health inequalities
Evidence tells us that low health status and unequal burden
of chronic disease is consistently experienced by high risk
subgroups within the community, including:
Indigenous Australians
people who experience socioeconomic disadvantage (and
who often have low literacy and education levels)
rural and remote populations
CALD communities.
Providing self-management interventions to Indigenous
Australians and people from CALD backgrounds does
not simply involve providing interpreters and translated
materials. It requires working with these communities
to explore and identify culturally appropriate concepts,
terminology and meaning. It also means undertaking
multi-faceted health promotion strategies, tailored to the
needs and characteristics of local populations, to raise
the profile of self-management across these communities.
CHSs are encouraged to work with ethno-specific
agencies, Migrant Information Centres and Aboriginal
Controlled Community Organisations that have expertise
in working with these subgroups.
Factors shown to contribute to the success of self-
management interventions include:
understanding health beliefs and expectations and
adapting interventions to meet these beliefs
increasing levels of health literacy and self-efficacy
tailoring information and materials
improving the communication skills of health care
providers
working with clients, their carers, families and
communities
addressing issues related to affordability in program
design, so that interventions present no barrier to take-up
addressing social, economic and environmental issues,
such as access to fresh food and improving access to
primary health care services
employing people from the target populations, including
Aboriginal health workers and bilingual health workers
ensuring that language barriers are addressed through the
use of interpreters, translation of materials or production
of pictorial materials
routinely following up clients (or recalling them for review)
who are at a higher risk of developing complications
supporting local communities to identify actions
that could increase the availability, accessibility and
appropriateness of self-management interventions
supporting local communities to identify social, economic
and environmental barriers to adopting healthy lifestyles
and addressing these through local health promotion
initiatives.
Australian work
Some work has already been conducted within Australia
to adapt the Stanford self-management group program to
better suit Chinese (Mandarin and Cantonese speaking),
Greek and Italian subgroups. The ational Health and
Medical Research Council funded a research project
(control trial) called Peer-Led Self-Management of Chronic
Illness for Chinese, Vietnamese, Greek and Italian People.
20 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
Information about this work and the research project is
available on the web.
38
The Commonwealth-funded Sharing Health Care Initiative
projects also focused on disadvantaged population
subgroups. Five projects were Indigenous-specific, two
focused on socioeconomic disadvantage, and two included
a focus on CALD subgroups. Information on the outcomes
of these projects and resources developed is available
on the web
39
. It is recommended that CHSs use these
learnings and resources.
Indigenous Australians
Findings from the Sharing Health Care Initiative working
with Indigenous Australians found that changes in behaviour
and self-management only occurred when individuals and
communities were informed about and accepted the need
to change, and when communities were engaged in decision
making around the problems that prevented behaviour
change. The key success factors for improved health
outcomes resulting from the initiative were:
a strong community engagement and development
approach
the use of health promotion strategies to bring about
changes to social and environmental barriers
communication between different organisations
systems flexibility and adaptability.
38 http://www.chronicillness.org.au/sig/documents/CIASIGSeminar-
Belfrage.pdf
http://www.latrobe.edu.au/aipc/director/plsmci/about_
healthprof.htm
39 http://www.health.gov.au/internet/wcms/Publishing.nsf/
Content/Sharing+Health+Care+Initiative-1
Examples of strategies included:
Videos were cooperatively produced to raise community
awareness of chronic disease and preventative activities.
Community support workers and community members
worked together to establish responsible serving of
alcohol in a popular club, and improve the quality and
quantity of fruit and vegetables at a local store.
Staff continuity within the initiative to build trust and
respect with community leaders.
International work
Outside of Australia, work has also occurred to modify self-
management programs to meet the needs of CALD groups.
For example, in the UK, where the Stanford Model has been
integrated into the ational Health System, the program
has been modified to suit the cultural needs of Bangladeshi
communities. Modifications include development of a
video that covers the key messages using key Bangladeshi
community members, separate programs for men and
women, and supporting volunteers from within the
community to deliver the program and recruit clients.
40
40 Jordan J and Osbourne R, 2007, Chronic Disease self-management Jordan J and Osbourne R, 2007, Chronic Disease self-management
education programs: challenges ahead, Medical Journal of Australia,
Volume 186 umber 1, p. 1.
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 21
5. Funding and reporting
5.1 Funding and reporting for community
health services
As CHSs already provide services to people with Type 2
diabetes, the self-management funding should be integrated
with existing funding. However, due to this funding being a
part of a new State Government commitment to manage
the impact of Type 2 diabetes on the Victorian population,
reporting for this funding will include:
service hours (as per standard community health
reporting mechanisms)
number of clients provided with a service (part of routine
data collection, but new in terms of CHS targets).
Funding is based on an allocation of $650 per person.
Therefore number of client targets are calculated on this
per person cost. CHSs that use SWITCH as their data
collection software should not have to change the way
they report, except to use a new diabetes self-management
code. The SWITCH mulitipurpose report has the capacity to
report client numbers against this new code.
5.2 Funding and reporting for PCPs
One-off funding of $15,000 has been provided to PCPs to
develop a range of strategies and processes to integrate
service provision delivered by GPs with service provision
delivered by CHSs and other relevant PCP member agencies
(in particular, referral and communication pathways), and
to develop relationships between CHS staff and general
practice staff. Given the core business of local DGP in
improving integration between GPs and other health care
providers, consideration should be given to allocation
of resources to the local DGP to support strategies for
engaging and working with local GPs.
Reporting on this funding will be:
a copy of the work plan developed with relevant PCP
member agencies including, in particular, the DGP.
a report at 12 months on the demonstrated outcomes
of this funding against the work plan.
5.3 Funding for workforce development
Funding for workforce development will be held by
Department of Human Services regional offices and
organised at a regional level. The level of funding provided is
based on need, as indicated by Ambulatory Care Sensitive
Condition data for diabetes in each region. It should be
targeted at improving the skills of the workforce to deliver
chronic care, in particular providing services to high risk
people with newly diagnosed Type 2 diabetes. The workforce
may include staff within ACCHOs, CHSs, DGP, PCPs,
practice nurses within general practices, RHSs.
Workforce development initiatives could provide staff with:
up-to-date diabetes education
a range of self-management interventions
motivational interviewing skills
lifestyle modification support skills
culturally appropriate services.
Workforce development may also need to be targeted
towards managers and leaders required to lead change,
develop and implement new systems, and review practices
and processes to ensure a greater focus on chronic care.
A training and development needs assessment at a regional
level may enable workforce development to be prioritised
and targeted towards identified gaps. The self-management
mapping process conducted on a PCP level will assist with
this process.
The following list provides some information about available
trainers and training packages. It is not exhaustive and the
department does not endorse any one trainer over another.
The list seeks to provide information only to regional offices
and funded agencies as they organise their own workforce
development strategy. In addition, agencies and/or PCPs
have worked with consultants who have expertise in CDM
and systems change.
Centre for Ethnicity in Health
Phone: 9342 9700
Email: training@ceh.org.au
Website: http://www.ceh.org.au/education/index.html
Culturally appropriate practice
Meeting the needs of CALD communities
Diabetes Australia, Victoria
Phone: 9667 1728
Email: mail@dav.org.au
Diabetes specific education
Regional forums available
International Diabetes Institute
Phone: 9258 5053
Website: http://www.diabetes.com.au/training/
Diabetes specific education
Flinders model training
Regional forums available
22 Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes
Initial diabetes services
People diagnosed with Type 2 diabetes should have access
to services within the first 12 months of being diagnosed.
Community Health Services would provide the following
initial services:
information about diabetes and managing diabetes
assistance with monitoring and maintaining healthy blood
glucose levels
support for self-management
referral information
liaison with the GP
assistance in coping with the impacts of a long-term
health condition.
The following initial services would be offered:
Client assessment: 1 one-hour consultation conducted
by an appropriately qualified allied health professional that
includes:
assessing knowledge and providing information on
diabetes
managing blood glucose levels
assessing lifestyle risk factors diet, physical activity
goal setting (short term and long term goals)
providing motivation for behaviour change.
Self-management intervention: 6 week two-hour
self-management group program conducted by an
appropriately qualified allied health professional (dietician,
physiotherapist etc.) that includes:
information on diabetes
self-management principles
using health and community services appropriately
carer/family involvement.
(Groups require a minimum of eight client participants.
Clients not suitable for groups will have access to 3 45
minute individual appointments.)
Client services and monitoring: 3 half-hour
consultations (over a 12-month period) conducted by
appropriately qualified allied health professionals to:
follow up individual issues
provide specific allied health services (for example,
podiatry, dietetics)
provide lifestyle support and diabetes advice
provide feedback to the GP.
Appendix 1
A summary model of community care through
community health services for people with Type 2 diabetes
Diabetes self-management: Guidelines for providing services to people newly diagnosed with Type 2 diabetes Guidelines for providing services to people newly diagnosed with Type 2 diabetes 23
Department of
Human Services
Você também pode gostar
- Chronic Disease Self-Management Education Programs: Challenges AheadDocumento4 páginasChronic Disease Self-Management Education Programs: Challenges AheadNurul Alif D SAinda não há avaliações
- Lifestyle-Related Diseases: DescriptionDocumento2 páginasLifestyle-Related Diseases: DescriptionKrizle AdazaAinda não há avaliações
- Self-Care Plan Empowers West Kent ResidentsDocumento32 páginasSelf-Care Plan Empowers West Kent Residentsflorentina dianAinda não há avaliações
- Improving Primary Health Care in NZDocumento40 páginasImproving Primary Health Care in NZfhreankAinda não há avaliações
- Challenges & Achievements of NRHMDocumento3 páginasChallenges & Achievements of NRHMRenu R NairAinda não há avaliações
- 5156904_688447230_1695638Documento12 páginas5156904_688447230_1695638Kalix NguyễnAinda não há avaliações
- Doh Community Health ProgramsDocumento48 páginasDoh Community Health ProgramsHope CarenaAinda não há avaliações
- The Philippine Health Care Delivery SystemDocumento4 páginasThe Philippine Health Care Delivery SystemKris Elaine GayadAinda não há avaliações
- Operational Guidelines For HWCDocumento83 páginasOperational Guidelines For HWCharleenAinda não há avaliações
- 5 Fifth National Action Plan Mar-08-01 (27-2-2014) PDFDocumento6 páginas5 Fifth National Action Plan Mar-08-01 (27-2-2014) PDFRamSha NoorAinda não há avaliações
- Community Nursing and Care Continuity LEARNING OUTCOMES After CompletingDocumento23 páginasCommunity Nursing and Care Continuity LEARNING OUTCOMES After Completingtwy113100% (1)
- PRESENTATION: Asia Pacific's Health Trends-Obesity, NCDs and ADB's Operational Plan For Health 2015-2020Documento40 páginasPRESENTATION: Asia Pacific's Health Trends-Obesity, NCDs and ADB's Operational Plan For Health 2015-2020ADB Health Sector GroupAinda não há avaliações
- CHN ReviewerDocumento18 páginasCHN ReviewerJean SamonteAinda não há avaliações
- Health Care DeliveryDocumento27 páginasHealth Care DeliveryAriane joy Cantilero100% (2)
- The Aquino Health AgendaDocumento38 páginasThe Aquino Health AgendaEdalyn CapiliAinda não há avaliações
- Office of The SecretaryDocumento15 páginasOffice of The SecretaryPatricia CastellanoAinda não há avaliações
- National Health Policies 2 ND YearDocumento40 páginasNational Health Policies 2 ND YearLIDIYA MOL P VAinda não há avaliações
- Borja APE Part IDocumento15 páginasBorja APE Part IArt BorjaAinda não há avaliações
- ADA 2023 GuidelineDocumento341 páginasADA 2023 GuidelineNazmul Hasan MahmudAinda não há avaliações
- G-4 HSM AssDocumento6 páginasG-4 HSM AssdavemanAinda não há avaliações
- The Health Care Delivery SystemDocumento34 páginasThe Health Care Delivery SystemFritzie Buquiron67% (3)
- IDF Guideline For Type 2 DiabetesDocumento123 páginasIDF Guideline For Type 2 DiabetesCho Maharani Rijhigo BaeAinda não há avaliações
- HEALTH CARE DELIVERY SYSTEM - CHNDocumento28 páginasHEALTH CARE DELIVERY SYSTEM - CHNShiangAinda não há avaliações
- Recommendations:: 1) Promoting Healthy LifestyleDocumento4 páginasRecommendations:: 1) Promoting Healthy LifestyleLea TanAinda não há avaliações
- Guidelines For Insulin Donations in Low-And Middle-Income Countries September 2017Documento8 páginasGuidelines For Insulin Donations in Low-And Middle-Income Countries September 2017armanAinda não há avaliações
- Government Hospital Project ReportDocumento23 páginasGovernment Hospital Project ReportAditi JainAinda não há avaliações
- Health Service Extension Programme Implementation GuidelineDocumento41 páginasHealth Service Extension Programme Implementation GuidelineWorkineh ChekolAinda não há avaliações
- HSTP With STG - G7Documento26 páginasHSTP With STG - G7Estiv W. StigAinda não há avaliações
- Health Policy AssignmentDocumento6 páginasHealth Policy AssignmentmmdadnanAinda não há avaliações
- Standards of Medical Care in Diabetes - 2021: Abridged For Primary Care ProvidersDocumento30 páginasStandards of Medical Care in Diabetes - 2021: Abridged For Primary Care Providersmỹ duyên đoànAinda não há avaliações
- Unit: 2Documento11 páginasUnit: 2Shristi BakhunchheAinda não há avaliações
- World Kidney Day 2024Documento2 páginasWorld Kidney Day 2024Al BasawiAinda não há avaliações
- Evidence Based Nutrition Guidelines For The Prevention and Management of DiabetesDocumento60 páginasEvidence Based Nutrition Guidelines For The Prevention and Management of DiabetesDiabetes Care100% (1)
- A Report On The Principles of Health EducationDocumento11 páginasA Report On The Principles of Health EducationRoucher PascuaAinda não há avaliações
- Lab CPHDocumento73 páginasLab CPHYam100% (1)
- Management of DM Type 2 CPGDocumento141 páginasManagement of DM Type 2 CPGShu ShanAinda não há avaliações
- Tools To Improve Access To Insulin: Acciss Multi-Stakeholder MeetingDocumento5 páginasTools To Improve Access To Insulin: Acciss Multi-Stakeholder MeetingarmanAinda não há avaliações
- Achieving Better Health Through Primary CareDocumento14 páginasAchieving Better Health Through Primary CareLu-an ReyesAinda não há avaliações
- Overview of Public Health Nursing in The PhilippinesDocumento35 páginasOverview of Public Health Nursing in The PhilippinesDarlen Rabano100% (1)
- Unit 5Documento39 páginasUnit 5Muhammad Abu Bakar Siddique 962-FET/BSME/F20Ainda não há avaliações
- Community Health Nursing roles, principles, and goalsDocumento21 páginasCommunity Health Nursing roles, principles, and goalsCleo Gabiana Jubay100% (1)
- Diaclincd 21 As 01Documento30 páginasDiaclincd 21 As 01renzo cardenasAinda não há avaliações
- Prevention and Reversal of Type 2 Diabetes: Highlights From A Symposium at The 2018 Diabetes UK Annual Professional ConferenceDocumento20 páginasPrevention and Reversal of Type 2 Diabetes: Highlights From A Symposium at The 2018 Diabetes UK Annual Professional ConferenceJorge Luis Jara ValderramaAinda não há avaliações
- Health SystemsDocumento29 páginasHealth SystemsMayom MabuongAinda não há avaliações
- BC Guiding Framework For Public Health 2017 UpdateDocumento58 páginasBC Guiding Framework For Public Health 2017 UpdateMayAinda não há avaliações
- Unit 8 P1 P2Documento10 páginasUnit 8 P1 P2Daniel John HaighAinda não há avaliações
- Ghidul Asociatiei Americane de Diabet Din 2022Documento315 páginasGhidul Asociatiei Americane de Diabet Din 2022Adina BrahaAinda não há avaliações
- National & Sttae Health Care Policy, National Population Policy, AyushDocumento52 páginasNational & Sttae Health Care Policy, National Population Policy, Ayushkrishnasree100% (2)
- Why Health Systems Must Change: Addressing The Needs of Ageing Populations in Low - and Middle-Income CountriesDocumento12 páginasWhy Health Systems Must Change: Addressing The Needs of Ageing Populations in Low - and Middle-Income CountriesHelpAge InternationalAinda não há avaliações
- NCD National PolicyDocumento14 páginasNCD National PolicyHerlene Lyneth ZalamedaAinda não há avaliações
- Tele DiabDocumento10 páginasTele DiabNelson LoboAinda não há avaliações
- How Proven Primary Prevention Can Stop DiabetesDocumento4 páginasHow Proven Primary Prevention Can Stop DiabetesSteveEpsteinAinda não há avaliações
- Unit 5 WADocumento5 páginasUnit 5 WAbnvjAinda não há avaliações
- Contemporary Community HealthDocumento36 páginasContemporary Community HealthChe ThaqifAinda não há avaliações
- Nationa L Health Policy 2017: Ms - Neethu Vincent Asst Professor KVM College of NursingDocumento34 páginasNationa L Health Policy 2017: Ms - Neethu Vincent Asst Professor KVM College of NursingNeethu Vincent100% (2)
- Module 2 CHNDocumento20 páginasModule 2 CHNyuuki konnoAinda não há avaliações
- Reflection Paper About Philippine Healthcare Delivery SystemDocumento2 páginasReflection Paper About Philippine Healthcare Delivery SystemTWINKLE MAE EGAY100% (1)
- India's Government Initiatives for Diabetes ManagementDocumento3 páginasIndia's Government Initiatives for Diabetes ManagementAchyutAinda não há avaliações
- Current Systems of Health CareDocumento4 páginasCurrent Systems of Health Carekangna_sharma20Ainda não há avaliações
- List of WHO Publications: Water Supply, Sanitation: How To Integrate Water, Sanitation and Hygiene Into HIV ProgrammesDocumento20 páginasList of WHO Publications: Water Supply, Sanitation: How To Integrate Water, Sanitation and Hygiene Into HIV ProgrammesvinayinscribdAinda não há avaliações
- Dengue ResourcesDocumento1 páginaDengue Resourcesdamag3Ainda não há avaliações
- WHO Article On Financing Malaria ControlDocumento107 páginasWHO Article On Financing Malaria Controlvinayinscribd100% (1)
- Article by National Academy On Aging SocietyDocumento6 páginasArticle by National Academy On Aging SocietyvinayinscribdAinda não há avaliações
- CDC Guidelines On DiabetesDocumento16 páginasCDC Guidelines On DiabetesvinayinscribdAinda não há avaliações
- Diabetes WHO-IDF ArticleDocumento20 páginasDiabetes WHO-IDF Articlevinayinscribd100% (1)
- Glucose Testing DevicesDocumento3 páginasGlucose Testing DevicesvinayinscribdAinda não há avaliações
- 23Documento148 páginas23vinayinscribdAinda não há avaliações
- Out Patient DepartmentDocumento52 páginasOut Patient DepartmentAnonymous ibmeej971% (7)
- Smart City 1 PDFDocumento187 páginasSmart City 1 PDFAvipriyo KarAinda não há avaliações
- Learners' Activity Sheets: Health 8Documento10 páginasLearners' Activity Sheets: Health 8Leode Joy TulangAinda não há avaliações
- Report On The Prevention and Intervention of Domestic Violence in Hong KongDocumento211 páginasReport On The Prevention and Intervention of Domestic Violence in Hong KongPablo ChanAinda não há avaliações
- Health Equity Handbook 8 CumulativeExampleDocumento18 páginasHealth Equity Handbook 8 CumulativeExamplePriyanshu MAinda não há avaliações
- CONCEPT EpidemilologyDocumento13 páginasCONCEPT EpidemilologyKrishnaveni MurugeshAinda não há avaliações
- General Dentistry: Provider Information Was Last Updated On 1/5/2012Documento8 páginasGeneral Dentistry: Provider Information Was Last Updated On 1/5/2012dusjohnAinda não há avaliações
- Patient Education and Clinical Health PromotionDocumento10 páginasPatient Education and Clinical Health PromotionReyta NoorAinda não há avaliações
- Phototherapy Care PlanDocumento17 páginasPhototherapy Care PlanISLAMIC KNOWLEDGE BASED ON TRULY HADIS100% (3)
- Smokers Level of Awareness On The Sin Tax Law and Their Cigarette ConsumptionDocumento60 páginasSmokers Level of Awareness On The Sin Tax Law and Their Cigarette ConsumptionKenjay CelesteAinda não há avaliações
- Test Bank For Gerontological Nursing 3rd Edition Patricia A Tabloski Isbn 10 0132956314 Isbn 13 9780132956314Documento13 páginasTest Bank For Gerontological Nursing 3rd Edition Patricia A Tabloski Isbn 10 0132956314 Isbn 13 9780132956314blowncolyhaxl100% (39)
- HIV Case (Week 2) - Antao, Alvarez, Hasan, Sanaani, UsmanDocumento15 páginasHIV Case (Week 2) - Antao, Alvarez, Hasan, Sanaani, UsmanNUR-HATHI SANAANIAinda não há avaliações
- Genetic Predisposition in Type 2 Diabetes A PromisingDocumento23 páginasGenetic Predisposition in Type 2 Diabetes A PromisingRa,i Al HaddadAinda não há avaliações
- Indonesia Country ProfileDocumento4 páginasIndonesia Country ProfilegitasariaryaniAinda não há avaliações
- Bronchiectasis 2Documento19 páginasBronchiectasis 2Liza FathiarianiAinda não há avaliações
- WEEK 1 - Concept of CommunityDocumento5 páginasWEEK 1 - Concept of Communitypoleene de leonAinda não há avaliações
- Epidemiological Aspects of Maternal and Child HealthDocumento30 páginasEpidemiological Aspects of Maternal and Child HealthNitin Sharma100% (1)
- World Health Organization Preventing Chronic Diseases A Vital InvestmentDocumento199 páginasWorld Health Organization Preventing Chronic Diseases A Vital InvestmentTux Gil100% (1)
- ONCA Conference 2017Documento316 páginasONCA Conference 2017Dave EatonAinda não há avaliações
- MLSPRIN Prelim NotesDocumento6 páginasMLSPRIN Prelim NotesJULIA MARIE BALILIAinda não há avaliações
- Public Health Theme: Introduction To Public Health: DR Elizabeth OrtonDocumento38 páginasPublic Health Theme: Introduction To Public Health: DR Elizabeth OrtonSidiq AboobakerAinda não há avaliações
- Foundations For Health Promotion Levels of Prevention: AbstractDocumento4 páginasFoundations For Health Promotion Levels of Prevention: AbstractIme ApAinda não há avaliações
- Atencion Integral de Enfermedades Respiratorias (AITER PAL OMSDocumento137 páginasAtencion Integral de Enfermedades Respiratorias (AITER PAL OMSBer Amorín UscataAinda não há avaliações
- Assessment of Knowledge, Attitudes and Practices of Mothers in Jos North Regarding ImmunizationDocumento9 páginasAssessment of Knowledge, Attitudes and Practices of Mothers in Jos North Regarding ImmunizationUlil Amri Pramadani100% (1)
- Rwanda PBF Manual Provides Guidance for Health FacilitiesDocumento44 páginasRwanda PBF Manual Provides Guidance for Health FacilitiesDamasceneAinda não há avaliações
- Family Assessment Manual PatternDocumento17 páginasFamily Assessment Manual PatternhoneykrizelAinda não há avaliações
- SLMQ1G11to12DRRM4 v2Documento22 páginasSLMQ1G11to12DRRM4 v2Joie OsherAinda não há avaliações
- 3.levels of Health CareDocumento43 páginas3.levels of Health CareNamrah AfzalAinda não há avaliações
- 6 08 Feng GarridoDocumento33 páginas6 08 Feng Garridoaprijon anasAinda não há avaliações
- Community Health Care Management For ChedDocumento5 páginasCommunity Health Care Management For Chedkrissy100% (1)