Você também pode gostar
- SOAP Note Cheat Sheet - Complete H&PDocumento2 páginasSOAP Note Cheat Sheet - Complete H&PAdeline N. Omene95% (19)
- Nursing Skills ManualDocumento52 páginasNursing Skills ManualCamille BattungAinda não há avaliações
- Pcca Confidential Hormone Evaluation: Medical HistoryDocumento5 páginasPcca Confidential Hormone Evaluation: Medical HistoryhaindnxjAinda não há avaliações
- Health and Medical Certificate 3Documento1 páginaHealth and Medical Certificate 3Danilo P. PancitoAinda não há avaliações
- Mirtazapine As An Appetite Stimulant and Anti-Emetic in Cats With Chronic Kidney Disease: A Masked Placebo-Controlled Crossover Clinical TrialDocumento5 páginasMirtazapine As An Appetite Stimulant and Anti-Emetic in Cats With Chronic Kidney Disease: A Masked Placebo-Controlled Crossover Clinical TrialWilliam ChandlerAinda não há avaliações
- Palliative Care NursingDocumento64 páginasPalliative Care NursingPrince Jhessie L. Abella100% (1)
- Old Disease NamesDocumento52 páginasOld Disease NamesMuhammad Ata Ul MustafaAinda não há avaliações
- Obstetric History Taking OSCE GuideDocumento17 páginasObstetric History Taking OSCE GuideSYDNIKA AIRA CARBONILLAAinda não há avaliações
- Fitness Assessment FormDocumento2 páginasFitness Assessment FormVishal PatleAinda não há avaliações
- Fitness Assessment FormDocumento2 páginasFitness Assessment FormVishal PatleAinda não há avaliações
- New Patient FormsDocumento6 páginasNew Patient FormsPerformax Physical TherapyAinda não há avaliações
- Health Assessment Form CSPCDocumento2 páginasHealth Assessment Form CSPCJoyce Ann B. Apin100% (2)
- Heart Disease: Heart Disease Risk Factors: The most important information you need to improve your healthNo EverandHeart Disease: Heart Disease Risk Factors: The most important information you need to improve your healthAinda não há avaliações
- PATIENT - HISTORY - FORM Final-20130611 PDFDocumento6 páginasPATIENT - HISTORY - FORM Final-20130611 PDFUloko ChristopherAinda não há avaliações
- The Terror of Pediatric MedicineDocumento360 páginasThe Terror of Pediatric MedicineNasir Khan100% (2)
- Review of SystemsDocumento3 páginasReview of SystemsCarrboro Family Medicine100% (1)
- Overcoming Helicobacter Pylori NaturallyDocumento130 páginasOvercoming Helicobacter Pylori NaturallywoofpaxAinda não há avaliações
- Musculoskeletal Assessment For Rugby PlayersDocumento43 páginasMusculoskeletal Assessment For Rugby PlayersThomas StAinda não há avaliações
- Decachords by A G ClarkeDocumento83 páginasDecachords by A G Clarkesunnyjamiel100% (1)
- Ankle and Foot Orthopedic TestsDocumento9 páginasAnkle and Foot Orthopedic TestsVishal PatleAinda não há avaliações
- Ankle and Foot Orthopedic TestsDocumento9 páginasAnkle and Foot Orthopedic TestsVishal PatleAinda não há avaliações
- Wheelchair Boxing & Fitness ExercisesDocumento230 páginasWheelchair Boxing & Fitness ExercisesVishal Patle100% (4)
- Assessment FormDocumento2 páginasAssessment FormVishal Patle67% (3)
- Blister Agents (HN T Q L HL)Documento65 páginasBlister Agents (HN T Q L HL)Reid Kirby100% (2)
- Cholesterol: Stress Management: The most important information you need to improve your healthNo EverandCholesterol: Stress Management: The most important information you need to improve your healthAinda não há avaliações
- Patient Health History 2Documento4 páginasPatient Health History 2Linda LloydAinda não há avaliações
- Dad'SphysicalformDocumento2 páginasDad'SphysicalformValerie YapAinda não há avaliações
- Patient PT Medical History PTDocumento2 páginasPatient PT Medical History PTEvaAinda não há avaliações
- New Patient Sleep QuestionnaireDocumento5 páginasNew Patient Sleep QuestionnairealviantiauliaAinda não há avaliações
- Acupuncture Forms FH Celebration Patient History Form 2015Documento4 páginasAcupuncture Forms FH Celebration Patient History Form 2015adem TremblayAinda não há avaliações
- Medical HistoryDocumento1 páginaMedical HistoryrehbergAinda não há avaliações
- HistoryDocumento1 páginaHistoryjmfleckAinda não há avaliações
- Adult Appraisal SRDocumento21 páginasAdult Appraisal SRAjmal KhanAinda não há avaliações
- Personalized Exercise Program QuestionnaireDocumento4 páginasPersonalized Exercise Program QuestionnaireSusan MatayonAinda não há avaliações
- Medical Form 2020 - 0Documento3 páginasMedical Form 2020 - 0Light King ChaudharyAinda não há avaliações
- Softball QuestionnaireDocumento3 páginasSoftball Questionnaireapi-256827540Ainda não há avaliações
- Personal Details (1)Documento3 páginasPersonal Details (1)jyoti.monga87Ainda não há avaliações
- Patient Form 2010Documento3 páginasPatient Form 2010elliepickAinda não há avaliações
- Intake Form Page 2Documento1 páginaIntake Form Page 2Casey OrrAinda não há avaliações
- Apta Eval-Fax Version Asapt 2007Documento4 páginasApta Eval-Fax Version Asapt 2007Abdur RasyidAinda não há avaliações
- OSNC Patient History FormDocumento5 páginasOSNC Patient History Formc2196722Ainda não há avaliações
- Saint Louis University School of Medicine Department of Medicine General Data: Past Medical HistoryDocumento3 páginasSaint Louis University School of Medicine Department of Medicine General Data: Past Medical HistoryMarieCrisAinda não há avaliações
- Entrance Health Examination Form 1Documento1 páginaEntrance Health Examination Form 1JunatamAinda não há avaliações
- Health Questionnaire for Weight Loss SurgeryDocumento7 páginasHealth Questionnaire for Weight Loss Surgerynoctulius_moongod6002100% (1)
- Patient Health ProfileDocumento9 páginasPatient Health ProfilerogeliocszAinda não há avaliações
- Reach100 QuestionnaireDocumento8 páginasReach100 QuestionnairegenerjustnAinda não há avaliações
- Health History FormDocumento5 páginasHealth History Formtyler615Ainda não há avaliações
- Patient Assessment Form: Current ProblemDocumento8 páginasPatient Assessment Form: Current ProblemJonard Ariefsieter HelperAinda não há avaliações
- Gestational Health Survey General Information: Page 1 of 2Documento2 páginasGestational Health Survey General Information: Page 1 of 2Malcolm XAinda não há avaliações
- Social Developmental HistoryDocumento2 páginasSocial Developmental History5cr1bdedAinda não há avaliações
- CertificateofhealthDocumento1 páginaCertificateofhealthlolalelaAinda não há avaliações
- Ace HHQDocumento4 páginasAce HHQbojanAinda não há avaliações
- Nutritional Clinical History Pregnant WomanDocumento13 páginasNutritional Clinical History Pregnant WomanScribdTranslationsAinda não há avaliações
- Assessment FormDocumento1 páginaAssessment FormmelquiadeselameAinda não há avaliações
- Autistic ChildDocumento10 páginasAutistic ChildQurat-ul-ain RajaAinda não há avaliações
- STUDENTS GUIDE RLE Written RequirementsDocumento22 páginasSTUDENTS GUIDE RLE Written Requirementsfhla.usman.swuAinda não há avaliações
- Mother's Information SheetDocumento1 páginaMother's Information SheetRochelle Gelvison100% (2)
- Tex Cuestionario SaludDocumento2 páginasTex Cuestionario SaludRaul ParsivalAinda não há avaliações
- Chronicle Diabetes Assessment FormDocumento8 páginasChronicle Diabetes Assessment FormpriyaAinda não há avaliações
- Health Questionnaire: Oral &maxillofacial SurgeryDocumento6 páginasHealth Questionnaire: Oral &maxillofacial SurgeryPaul MathaiAinda não há avaliações
- Case History 20Documento5 páginasCase History 20eric wruckAinda não há avaliações
- Medical Questionnaire For PatientsDocumento1 páginaMedical Questionnaire For Patientsjrepko1Ainda não há avaliações
- Carolina Plastic SurgeryDocumento5 páginasCarolina Plastic SurgeryBob LoblawAinda não há avaliações
- Wellnesspe HealthDocumento1 páginaWellnesspe Healthapi-264559907Ainda não há avaliações
- Date: - : (Last) (First) (Middle)Documento5 páginasDate: - : (Last) (First) (Middle)KatieAinda não há avaliações
- 2.physical E, HISTORY NCPDocumento13 páginas2.physical E, HISTORY NCPمريم حجيAinda não há avaliações
- Patient Entrance Form1 2019 12ptpdfDocumento6 páginasPatient Entrance Form1 2019 12ptpdfapi-478211107Ainda não há avaliações
- English Health Clearance FormDocumento2 páginasEnglish Health Clearance FormGerard HungAinda não há avaliações
- Cardiac Evaluation Form Final PosDocumento2 páginasCardiac Evaluation Form Final PosdrmuralicbeAinda não há avaliações
- Anamnesis Form: Name Dose Regularity How Long Have You Been Taking ItDocumento3 páginasAnamnesis Form: Name Dose Regularity How Long Have You Been Taking ItĐeŋýzař Đ ZòįđýckAinda não há avaliações
- Pediatric Medical History FormDocumento2 páginasPediatric Medical History FormRoshandiep Gill100% (1)
- Today's Date: - Name: - Date of Birth - Phone Number: - Age: - Email AddressDocumento2 páginasToday's Date: - Name: - Date of Birth - Phone Number: - Age: - Email Addressanedik40Ainda não há avaliações
- Sports PhysicalDocumento4 páginasSports Physicalapi-209628543Ainda não há avaliações
- My Heart Book: A Practical Book to Manage Heart FailureNo EverandMy Heart Book: A Practical Book to Manage Heart FailureAinda não há avaliações
- Comparative Study On Efficacy of Moderate Intensity Land Based Endurance Exercise & Moderate Intensity Water Based Endurance Exercise On Normal Young Individuals - Vishal Patle, Devayani ThakreDocumento20 páginasComparative Study On Efficacy of Moderate Intensity Land Based Endurance Exercise & Moderate Intensity Water Based Endurance Exercise On Normal Young Individuals - Vishal Patle, Devayani ThakreVishal PatleAinda não há avaliações
- Definition of PhysiotherapyDocumento1 páginaDefinition of PhysiotherapyVishal PatleAinda não há avaliações
- Definition of PhysiotherapyDocumento1 páginaDefinition of PhysiotherapyVishal PatleAinda não há avaliações
- POSTURE AssessmentDocumento4 páginasPOSTURE AssessmentVishal PatleAinda não há avaliações
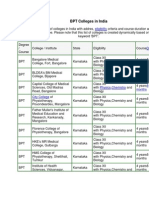
- Bachelor of Physiotherapy Colleges in IndiaDocumento7 páginasBachelor of Physiotherapy Colleges in IndiaVishal PatleAinda não há avaliações
- Physical Assessment Form AnalysisDocumento3 páginasPhysical Assessment Form AnalysisVishal PatleAinda não há avaliações
- Cardio-Respiratory Assessment ChartDocumento3 páginasCardio-Respiratory Assessment ChartVishal Patle100% (2)
- Initial Assessment ChecklistDocumento1 páginaInitial Assessment ChecklistVishal PatleAinda não há avaliações
- Download Physical Therapy & Orthopedic BooksDocumento7 páginasDownload Physical Therapy & Orthopedic BooksVishal PatleAinda não há avaliações
- Nursing Care for Digestive DisordersDocumento5 páginasNursing Care for Digestive DisordersNoriel GirayAinda não há avaliações
- Letter: "Kambô" Frog (Phyllomedusa Bicolor) : Use in Folk Medicine and Potential Health RisksDocumento2 páginasLetter: "Kambô" Frog (Phyllomedusa Bicolor) : Use in Folk Medicine and Potential Health RisksEdilene Coffaci de LimaAinda não há avaliações
- Premstop 5Documento6 páginasPremstop 5Laura SpinuAinda não há avaliações
- Microbiological Guidelines For Ready-To-Eat FoodsDocumento5 páginasMicrobiological Guidelines For Ready-To-Eat Foodscaya1172Ainda não há avaliações
- Universal IndicatorDocumento6 páginasUniversal IndicatorpraveenAinda não há avaliações
- Knowledge and Practices Regarding Management of Minor Ailments of Pregnancy Among Antenatal Mothers: A Descriptive Study From RajasthanDocumento8 páginasKnowledge and Practices Regarding Management of Minor Ailments of Pregnancy Among Antenatal Mothers: A Descriptive Study From RajasthanMudasir Ahmad BhatAinda não há avaliações
- n320 Peds NCP wk3Documento2 páginasn320 Peds NCP wk3api-301826049Ainda não há avaliações
- Norovirus ManagementDocumento23 páginasNorovirus ManagementsehrAinda não há avaliações
- Student - Module 1Documento31 páginasStudent - Module 1Emerlinda OlivaAinda não há avaliações
- wm2000 NaturalstandardDocumento3 páginaswm2000 NaturalstandardMarketplaceAinda não há avaliações
- What Is Theophylline ToxicityDocumento7 páginasWhat Is Theophylline ToxicitySaad BuhussainAinda não há avaliações
- Effects of Benson's Relaxation Technique On Nausea in Patients With Chronic Kidney Disease Undergoing HemodialysisDocumento10 páginasEffects of Benson's Relaxation Technique On Nausea in Patients With Chronic Kidney Disease Undergoing HemodialysisendroAinda não há avaliações
- Ayurveda Articles PDFDocumento704 páginasAyurveda Articles PDFAnonymous TWzli5100% (2)
- A Step-By-Step Guide To Performing A Complete Abdominal ExaminationDocumento8 páginasA Step-By-Step Guide To Performing A Complete Abdominal Examinationjojohnson250Ainda não há avaliações
- Drug Study School Nsg.Documento12 páginasDrug Study School Nsg.Keila RosalesAinda não há avaliações
- Drug study on chemotherapeutic alkylating agentsDocumento16 páginasDrug study on chemotherapeutic alkylating agentsPrincess CruzAinda não há avaliações
- Drug StudyDocumento2 páginasDrug Studykym_estrellaAinda não há avaliações
- Jurnal Anti EmetikDocumento13 páginasJurnal Anti EmetikandrianiAinda não há avaliações
- Maye Bato 47 Yo, F: Surgery Module 5 Facilitator: Dr. Jerry Alinsug Group 7Documento1 páginaMaye Bato 47 Yo, F: Surgery Module 5 Facilitator: Dr. Jerry Alinsug Group 7Luke Matthew MondaresAinda não há avaliações
- Mefenamic Acid Is A Non-SteroidalDocumento4 páginasMefenamic Acid Is A Non-SteroidalAnkan PalAinda não há avaliações
- Murtagh Triads FlashcardsDocumento116 páginasMurtagh Triads FlashcardsKeithKam100% (1)