Você também pode gostar
- Riyafa Hussainsm NewDocumento10 páginasRiyafa Hussainsm NewRiyafa AhmedAinda não há avaliações
- Riyafa Hussainsm NewDocumento10 páginasRiyafa Hussainsm NewRiyafa AhmedAinda não há avaliações
- Benefits of SocialDocumento5 páginasBenefits of SocialRiyafa AhmedAinda não há avaliações
- Job Description PG 2Documento1 páginaJob Description PG 2Riyafa AhmedAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- The LungsDocumento6 páginasThe LungsnandaAinda não há avaliações
- Scrotal HerniaDocumento9 páginasScrotal HerniaReymart BolagaoAinda não há avaliações
- Masterlist SummaryDocumento6 páginasMasterlist Summarykentclark03Ainda não há avaliações
- A Mindfulness Intervention For Children With Autism Spectrum DisorderDocumento155 páginasA Mindfulness Intervention For Children With Autism Spectrum Disorderclaughlinsr4721Ainda não há avaliações
- Medical Certificate Guidelines June 2012Documento3 páginasMedical Certificate Guidelines June 2012wudthipanAinda não há avaliações
- Clinical Examination and Management of Impairments in VariousDocumento34 páginasClinical Examination and Management of Impairments in Variousmukesh pokharelAinda não há avaliações
- Staph and Strep Lab Report BMS 501Documento2 páginasStaph and Strep Lab Report BMS 501aruiz93Ainda não há avaliações
- Modified Fluid Wax Impression For A Severely Resorbed Edentulous Mandibular RidgeDocumento4 páginasModified Fluid Wax Impression For A Severely Resorbed Edentulous Mandibular RidgeChepe LemusAinda não há avaliações
- Integrating Modern Dermatology and AyurvedaDocumento25 páginasIntegrating Modern Dermatology and AyurvedachandusgAinda não há avaliações
- Class 11 English Snapshots Chapter 7Documento2 páginasClass 11 English Snapshots Chapter 7Alpha StarAinda não há avaliações
- Click Here Click Here To View Optimized Website For Mobile DevicesDocumento4 páginasClick Here Click Here To View Optimized Website For Mobile DevicesFirman SalamAinda não há avaliações
- Emergency Preparedness Concepts Test BankDocumento13 páginasEmergency Preparedness Concepts Test BankTyson Easo JonesAinda não há avaliações
- Klucel - Varnostni List PDFDocumento4 páginasKlucel - Varnostni List PDFIljuha9Ainda não há avaliações
- Elphos Erald: Second Shot: Hillary Clinton Running Again For PresidentDocumento10 páginasElphos Erald: Second Shot: Hillary Clinton Running Again For PresidentThe Delphos HeraldAinda não há avaliações
- This Just In!: Queen Pin Carla!Documento10 páginasThis Just In!: Queen Pin Carla!BS Central, Inc. "The Buzz"Ainda não há avaliações
- PG Physician Guide 03 Eng1Documento88 páginasPG Physician Guide 03 Eng1hüseyin vururAinda não há avaliações
- Complex Regional Pain Syndrome in Adults - Second Edition - 0 PDFDocumento97 páginasComplex Regional Pain Syndrome in Adults - Second Edition - 0 PDFLotteDomineAinda não há avaliações
- Pest Control Risk Assessment Indoor and OutdoorDocumento72 páginasPest Control Risk Assessment Indoor and OutdoorarmkarthickAinda não há avaliações
- Relaxation TechniquesDocumento13 páginasRelaxation TechniquesBhakti Joshi KhandekarAinda não há avaliações
- Medical Surgical Treatments For EDDocumento31 páginasMedical Surgical Treatments For EDskumar_p7Ainda não há avaliações
- Anvisa National Health Surveillance AgencyDocumento52 páginasAnvisa National Health Surveillance AgencyVimarsha HSAinda não há avaliações
- Pivas 2018Documento46 páginasPivas 2018Denny PaatAinda não há avaliações
- Sage Char-Lee ResumeDocumento2 páginasSage Char-Lee Resumeapi-510197139Ainda não há avaliações
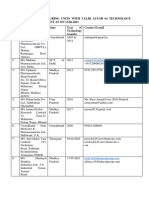
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Documento5 páginasList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesAinda não há avaliações
- RAV Admission Notice for Ayurveda CoursesDocumento4 páginasRAV Admission Notice for Ayurveda CoursesBhargav KalalAinda não há avaliações
- Your Consequences WorksheetDocumento10 páginasYour Consequences WorksheetThe Center for Motivation and ChangeAinda não há avaliações
- Case Study of Mrs. WalkerDocumento4 páginasCase Study of Mrs. WalkerPreet ChahalAinda não há avaliações
- Pasteurized EggsDocumento8 páginasPasteurized Eggsapi-202950260Ainda não há avaliações
- Rayner 2018Documento11 páginasRayner 2018antonio de diaAinda não há avaliações
- 2014 Body Code Client Information PDFDocumento7 páginas2014 Body Code Client Information PDFkrug100% (1)