Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Use of "Zingiber Officinale Roscoe L" Root in Various DiseasesDocumento8 páginasUse of "Zingiber Officinale Roscoe L" Root in Various DiseasesCentral Asian StudiesAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Chapter 7 - Hannah Wilder - ChorioamnionitisDocumento7 páginasChapter 7 - Hannah Wilder - ChorioamnionitisEunice CortésAinda não há avaliações
- Cosmetic Surgery PDFDocumento3 páginasCosmetic Surgery PDFDa Young Anna Choi100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- of M.pharmDocumento13 páginasof M.pharmVivek Patel ViksAinda não há avaliações
- Literature & MedicineDocumento14 páginasLiterature & MedicineJoyce LeungAinda não há avaliações
- Disabilities Act 1995Documento4 páginasDisabilities Act 1995directdeoAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Indications Dose Duration Administration Stability Warning & PrecautionsDocumento2 páginasIndications Dose Duration Administration Stability Warning & PrecautionsFatma HasanAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- HarveyDocumento6 páginasHarveyapi-276953527Ainda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Laboratory Investigation Report: HaematologyDocumento3 páginasLaboratory Investigation Report: HaematologyHarshitAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Rab Flow CHT 3 PeopleDocumento2 páginasRab Flow CHT 3 PeopleWDIV/ClickOnDetroitAinda não há avaliações
- Nur 300-Nursing Philosophy-CdDocumento7 páginasNur 300-Nursing Philosophy-Cdapi-501578262Ainda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Anemia Proposal RefinedDocumento13 páginasAnemia Proposal RefinedAxel BlazeAinda não há avaliações
- RECORDING Form 1: Masterlist of Grade 1 StudentsDocumento4 páginasRECORDING Form 1: Masterlist of Grade 1 StudentsGirlie Harical GangawanAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Conference & Workshop ScheduleDocumento5 páginasConference & Workshop ScheduleglmoningkaAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Daily Vagus Nerve Exercises A Self-Help G - Sherman SanderDocumento90 páginasDaily Vagus Nerve Exercises A Self-Help G - Sherman Sanderscriberone100% (6)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
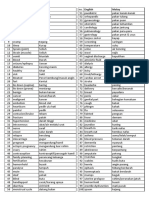
- Medic Term English MalayDocumento1 páginaMedic Term English MalaySyamimi SuhaimiAinda não há avaliações
- ProjectDocumento3 páginasProjectAnshul PaunikarAinda não há avaliações
- Hemisphere SpecializationDocumento7 páginasHemisphere SpecializationLisa MartinezAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Hipertensi KrisisDocumento30 páginasHipertensi KrisisLuthfan HakimAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- PeritonitisDocumento21 páginasPeritonitischrisyenAinda não há avaliações
- Gambaran Penggunaan Antibiotik Pada Pasien Pediatri Infeksi Saluran Pernapasan Akut (Ispa) Di Klinik Sint. Carolus BengkuluDocumento8 páginasGambaran Penggunaan Antibiotik Pada Pasien Pediatri Infeksi Saluran Pernapasan Akut (Ispa) Di Klinik Sint. Carolus BengkuluLuli Corvelo SarmentoAinda não há avaliações
- Thyroid Crisis... FinalDocumento53 páginasThyroid Crisis... FinalYhanaAdarneAinda não há avaliações
- Wilkins 6 - Neurological Assessment - AssignmentDocumento33 páginasWilkins 6 - Neurological Assessment - AssignmentArifurRahman100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Fractures in ChildrenDocumento26 páginasFractures in ChildrenRafli SoehadakAinda não há avaliações
- Category Class Merit Round2 MBBS-BDSDocumento102 páginasCategory Class Merit Round2 MBBS-BDSSUSHIL LAKRAAinda não há avaliações
- Ozone Therapy by Saul Pressman at Oxygen Therapies Support Forum, Topic 443552 PDFDocumento15 páginasOzone Therapy by Saul Pressman at Oxygen Therapies Support Forum, Topic 443552 PDFHello MisterAinda não há avaliações
- First Aid / CPR: HSE Training 2005Documento36 páginasFirst Aid / CPR: HSE Training 2005Martin griffinAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- InhalantDocumento8 páginasInhalantArvin Ian Penaflor100% (1)
- Roles & Responsibilities of CRADocumento26 páginasRoles & Responsibilities of CRANaresh Kumar RapoluAinda não há avaliações
- Vit KDocumento2 páginasVit KBilly Jeremia TandoAinda não há avaliações