Escolar Documentos
Profissional Documentos
Cultura Documentos
Laparotomia para Trauma
Enviado por
jesus-suarez-villamizar-2361Descrição original:
Título original
Direitos autorais
Formatos disponíveis
Compartilhar este documento
Compartilhar ou incorporar documento
Você considera este documento útil?
Este conteúdo é inapropriado?
Denunciar este documentoDireitos autorais:
Formatos disponíveis
Laparotomia para Trauma
Enviado por
jesus-suarez-villamizar-2361Direitos autorais:
Formatos disponíveis
Current Problems in
Volume 33 Number 8 August 1996
The Trauma Celiotomy: The Evolving
Concepts Of Damage Control
-------.-------
John A. Morris, Jr., MD
Associate Professor of Surgery
Director, Division of Trauma & Surgical Critical Care
Vanderbilt University School of Medicine
Nashville, Tennessee
Virginia A. Eddy, MD
Assistant Professor of Surgery
Division of Trauma & Surgical Critical Care
Vanderbilt University School of Medicine
Nashville, Tennessee
Edmund J. Rutherford, MD
Assistant Professor of Surgery
Division of Trauma & Surgical Critical Care
Vanderbilt University School of Medicine
Nashville. Tennessee
....,. ATimes Mirror
~ Company
Current Problems in
Surgery
Information for Readers
Annual
subscription prices USA Canada* International'
Individuals 5 90.00 $111.28 5\Ot-00
StudentslResidents 5 47.00 S 65.27 5 61.00
Institutions $122.00 $145.52 S136.00
Single Copy S 15.00 S 15.00 $ 15.00
Binders $ 23.00 S 24.61 S 23.00
Effective until September 30, 1996.
Airmail rates available on request.
'Canadian 7'7c Goods and Services Tax, calculated on US base rate, has been added and will be
paid by Mosby to Revenue Canada under GST No. R127341295.
t Exclusive of India and Japan. Contact the publisher for information on how to subscribe in
these countries.
ClIrren/ Problems ill SlIrgery1l (ISSN 0011-3840) is published monthly by Mosby-Year Book, Inc.,
11830 Westline Indusuial Dr., St. Louis. 1\10 63146-3318. Periodicals postage paid at St. Louis, Mo., and
additional mailing offices. US Send address changes 10 ClIrrell! Problems in SlIrgery',
Mosby-Year Book. Inc., 11830 Westline Indusuial Dr., St. Louis, 63146-3318.
Subscription OrderslInquiries and Back Issues: Contact Subscription Services, Mosby-Year
Book, Inc., 11830 Westline Industrial Dr., St. Louis, MO 63146-3318; telephone (800)453-4351 or
(314)453-4351; fax (314)432-1158; E-mail: jOllmal.sen'ice@mosby.com.
Bulk Quantity Purchases: Contact Donna S. Ricko, Mosby-Year Book,lnc., I Stonegate Road,
Chelmsford, MA 01824; telephone (508)4868971; fax (508)486-9423.
Copyright. Copyright tV 1996 by Mosby-Year Book. Inc. All rights reserved. No part of this
publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means-
electronic, mechanical, photocopying, recording, or otherwise-without prior written permission from
the publisher, except in cases described below.
This Journal has been registered \\ ith the Copyright Clearance Center. Inc. 222 Rosewood Drive.
Danvers. MA 01923. Consent is given for the copying of articles for personal or internal use of specific
clients. This consent is given on the condition that the copier pay directly to the CCC the base fee of
S6.00 per article plus $.\0 per page for copying be)ond that permitted by US Copyright Law: 0011-
3840/96/56.00 + .10. This consent does not extend to other kinds of copying. such as for general
distribution. resale, advertising, and promotional purposes or for creating new collective works. All
inquiries regarding copyrighted material from this publication other than those that can be handled
through the CCC should be directed, in writing, to Associate Publisher, Journal Permissions,
Mosby-Year Book, Inc. 11830 Westline Industrial Drive, SI. Louis. MO 63146-3318; telephone
(314)453-4129; fax (314)432-1380.
Indexing. ClIrrelll Problems ill SlIrgery' is listed in Illdex MediclIs, ClIrrelll COIl/ellls/Clillical
Medicille. EMBASE. the Medica database, and SCI.
Disclaimer. Statements and opinions expressed herein arc those of the author(s) and not necessarily
those of the editor(s) or publisher. and the editor(s) and publisher disclaim any responsibility or liability
for such material. Neither the editor(s) nor the publisher guarantees, warrants, or endorses any product
or service advertised in this publication. nor do they guarantee any claim made by the manufacturer of
such product or service.
Current Problems in
The Trauma Celiotomy: The Evolving
Concepts Of Damage Control
-------.-------
Foreword
In Brief
Introduction
Damage Control
Preoperative Evaluation
The Procedure
The Decision
Definitive Packing
Skin Closure
Restoration of Physiologic Reserve
Warming the Patient
Coagulopathy and Massive Transfusion
Cardiopulmonary Management
Acid-Base Balance
Special Considerations in Secondary Resuscitation
Reconstruction
Procedure
Options for Closure
Organ Repair
Introduction
Organs of the True Abdomen
Organs of the Retroperitoneum
Vascular
References
Curr Probl Surg, August 1996
612
613
617
619
620
621
630
632
632
634
634
635
637
640
642
645
645
647
649
649
,650
664
679
684
611
612
-------.-------
Foreword
Treatment of the patient with trauma and associated multiple
organ system injury is one of the most challenging problems
confronting the surgeon. In the first seven decades of this cen-
tury, improvements in the care of civilian patients with trauma
mostly resulted from lessons learned in world wars or regional
conflicts. In the last two decades the care of the severely in-
jured patient has continued to improve, but this improvement
has been primarily due to other factors: the regionalization of
trauma care and the development of designated trauma centers
combined with increased development of the disciplines ofemer-
gency medicine and surgical critical care. In this issue of Cur-
relit Problems ill Surgery, Dr. John Morris and his associates,
Dr. Virginia Eddy and Dr. Edmund Rutherford of the Vanderbilt
University School of Medicine, have written an outstanding
monograph on "The Trauma Celiotomy: The Evolving Con-
cept of Damage ControL" Their manuscript is divided into four
parts: preoperative evaluation and damage control of the in-
jured patient, secondary resuscitation and regeneration of the
patient's physiologic reserve, operative management with re-
construction of intraabdominal and extraabdomina,I injuries fol-
lowed by wound closure, and the definition of a grading system
to define injury. This monograph is an excellent
review of a topic of great importance to surgeons. It wiII serve
as an authoritative source of information for medical students,
house officers, and practicing surgeons.
Samuel A. Wells, Jr., MD
Editor-in-Chief
Curr Prabl Surg, August 1996
-------.-------
In Brief
Although the trauma celiotomy has its origins in the general surgery
celiotomy, these have evolved into two distinctly different operations. This
evolution has been nurtured by the advent of regional trauma systems and
the development of the discipline of surgical critical care. In this
monograph we offer our approach to patients undergoing trauma
celiotomy.
We view the trauma celiotomy as a continuum. This continuum begins
with the primary resuscitation initiated in the field by emergency medical
personnel and concludes with the return of the patient to the operating room
for definitive organ repair and fascial closure. In most patients this occurs
in a single procedure, but in other patients the continuum may occur over
several days.
When the trauma patient arrives at the hospital, primary resuscitation
proceeds according to advanced trauma life support guidelines and is
designed to identify and control immediately life-threatening injuries and
to define and enhance the patient's physiologic reserve. It is during the
primary resuscitation that the first critical decision must be made. That is,
does the patient require celiotomy? If the answer is yes, the trauma
celiotomy proceeds in an organized and disciplined fashion through three
phases: (1) damage control, (2) identification of injuries, and (3) organ
repair and reconstruction.
A small subset of patients, those who are ill extremis, are physiologically
incapable of tolerating extensive operative intervention. Impending
physiologic exhaustion, heralded by hypothermia, coagulopathy, and
acidosis, should mandate termination of the operation, rapid towel clip
closure, secondary resuscitation in the surgical intensive care unit, and
return to the operating 'room at a later time for definitive repair of injuries.
Recognition of the patient ill extremis is a crucial element of this approach.
Damage control, which was once applied only in desperation to patients
who were near physiologic exhaustion, is no longer a procedure of last
resort. Instead, physiologic exhaustion must be anticipated, and damage
control becomes the first step in every trauma celiotomy. Damage control
is designed to control hemorrhage, control contamination, and identify
injuries. These three elements are the first priorities and the only mandatory
components of the trauma celiotomy that must be performed on the day of
injury.
Curr Probl Surg. August 1996 613
The first step in damage control is the temporary control of hemorrhage
and contamination. This provides the surgeon time to achieve exposure,
define injuries, and develop a strategic plan for the remainder ~ f the
operation. Temporary control of hemorrhage is achieved by four quadrant
packing, which is designed to tamponade bleeding sites and absorb free
blood in the abdomen. This process takes only 3 to 4 minutes and can be
most beneficial in the setting of blunt trauma. Definitive control of
hemorrhage begins with the differentiation between parenchymal bleeding
and "surgical bleeding." Surgical bleeding from the major blood vessels
requires ligation or at least proximal and distal control.
Once temporary control of hemorrhage is achieved and blood is removed
from the abdomen, a systematic exploration is performed. This disciplined,
structured process must identify both intraperitoneal and retroperitoneal
injuries. Injured bowel is identified, and contamination is controlled
temporarily with Babcock clamps. After the abdomen is fully explored,
definitive control of contamination is accomplished with either bowel
repair or resection, depending on the location, magnitude, and multiplicity
of the injury. Bowel resection is not performed, however, until all injuries
have been identified and assessed and a complete treatment strategy has
been developed.
Once injuries are defined and the physiologic reserve is quantified,
repairs are prioritized, and a strategic plan for the operation is devised and
executed. If at any point the patient's condition deteriorates to a critical
level of physiologic reserve, the operative procedure should be terminated
in an orderly fashion, and the patient is transported to the surgical intensive
care unit for secondary resuscitation.
Organ repair and reconstruction is undertaken only in patients who have
sufficient physiologic reserve to tolerate additional operative intervention.
Approximately 90% of patients undergoing trauma celiotomy can tolerate
damage control and organ repair at the same operative setting. The remaining
10% of patients are ill extremis, which we define to include temperature less
than 35C, a base deficit greater than -15 mmollL, coagulopathy, and bowel
edema. These patients have exhausted their physiologic reserve and cannot
tolerate further operative intervention. The early recognition of impending
physiologic exhaustion is a critical decision point. '
Once the patient is determined to be ill extremis, the operation is
terminated in an orderly fashion. Solid organs are packed definitively, and
surgical bleeding is controlled by vessel ligation. No effort is made to close
the fascia; instead, the skin is closed with towel clips. The patient is then
transported rapidly to the surgical intensive care unit for secondary
resuscitation.
614 Curr Probl Surg, August 1996
The secondary resuscitation includes correction of coagulopathy,
hypothermia, and acid-base balance. Simultaneously, efforts are instituted
to maximize oxygen delivery by appropriate blood transfusion, increasing
the cardiac output, and ventilator support. The patient is returned to the
operating room electively for organ repair and definitive abdominal closure
when the following goals of secondary resuscitation have been achieved:
temperature greater than 36
0
C, prothrombin time less than 15 seconds,
platelet count greater than 75,000 mm
3
, mixed venous oxygen saturation
greater than 65%, and cardiac index greater than 3.5 Umin. Operative
repair of extraabdominal injuries should be prioritized after abdominal
reconstruction. If the patient's physiologic condition permits, reconstruc-
tion of these injuries may be undertaken concurrently.
Although 80% of patients undergoing damage control celiotomy
successfully complete the secondary resuscitation, 20% require emergent
reoperation. It can sometimes be difficult to differentiate between "surgical
bleeding" and "medical bleeding" in the setting of coagulopathy and
hypothermia. For patients with penetrating trauma, the patient is
emergently returned to the operating room for reexploration if the post-
operative bleeding exceeds 15 units regardless of the patient's temperature.
For patients with either blunt or penetrating trauma, emergent reoperation
is indicated for bleeding greater than 2 units per hour in the presence of
normothermia or for the development of abdominal compartment
syndrome.
The redesigned trauma celiotomy and ultimately the entire surgical
treatment of patients is defined by three critical decision points: (I)
determining the need for celiotomy, (2) identifying the patient ill extremis
and terminating the procedure appropriately, and (3) given the patient ill
extremis, determining the most appropriate timing of reoperation. These
decisions should be based on experience and, above all, physiologic data. It
is no longer acceptable to perform a technically satisfying operation only to
have the patient die as a result of physiologic exhaustion. The trauma
surgeon must recognize the limits imposed by the patient's physiologic
condition and modify the duration and scope of the initial operation.
Curr Probl Surg, August 1996 615
John A. Morris, Jr., MD, is Director
of the Division of Trauma and Sur-
gical Critical Care and Associate
Professor of Surgery at Vanderbilt
University School of Medicine. He
completed his medical education
and surgical residency at the University of Kentucky and served a fellow-
ship in trauma and burns at San Francisco General Hospital. He is a Fellow
of the American College of Surgeons and a member of the Eastern Asso-
ciation for the Surgery of Trauma, the Western Trauma Association, the
Society of Critical Care Medicine, and the Southern Surgical Association.
Virginia A. Eddy, MD, is Assistant Professor of Surgery
at Vanderbilt University School of Medicine and the As-
sociate Director of Education in the Division of Trauma
and Critical Care. She completed her medical educa-
tion and surgical residency at the University of South
Carolina and served a fellowship in critical care and trauma at Vanderbilt
University. She is a member of the society of Critical Care Medicine, the
Eastern Association for the Surgery of Trauma, the Association for Surgi-
cal Education, and is actively involved in the American Association of Medi-
cal Colleges.
Edmund J. Rutherford, MD, graduated
from the University of Pittsburgh
School of Medicine, completed his resi-
dence at the University of North Caro-
lina at Chapel Hill arid New Hanover
Memorial Hospital in Wilmington, North Carolina, and served a fellowship
in critical care and trauma at the University of North Carolina. He is Assis-
tant Professor of Surgery at Vanderbilt University School of Medicine and a
Fellow of the American College of Surgeons. His professional member-
ships include the Eastern Association for the Surgery of Trauma, the Soci-
ety of Critical Care Medicine, and the Western Trauma Association.
616 Curr Probl Surg, August 1996
-------.-------
The Trauma Celiotomy: The Evolving:
Concepts Of Damage Control
T
he trauma patient ill extremis is one short step from death. As sur-
geons, we intuitively recognize these patients. They present with
profound shock, altered mental status, respiratory distress, and of-
ten extensive tissue destruction. These patients are unlikely to survive un-
less heroic efforts are made to control hemorrhage, restore blood volume,
and minimize infection.
These heroic techniques have evolved largely because of two recent trends
in health care: the implementation of regional trauma systems and the growth
of the discipline of surgical critical care. Trauma systems provide a struc-
ture for identifying severely injured patients in the field
2
and transporting
the patients to designated trauma centers.
3
Regionalization has brought the
evolution of trauma care from the battlefield and placed it squarely in the
civilian environment. One result of this regionalization of trauma care has
been to concentrate a relatively large number of patients with trauma in the
hands of a small number of physicians.
The discipline of surgical critical care merges the art of surgery with the
science of physiology. No longer is it acceptable to perform a technically
satisfying operation only to have the patient die as a resolt of physiologic
exhaustion. The trauma surgeon today is taught to recognize the limits
imposed by the patient's physiologic condition and to modify the duration
and scope of surgery accordingly. Nowhere is this more apparent than in
the celiotomy for trauma. In the trauma celiotomy, injuries are undefined,
the physiologic condition can be unstable, the exposure is poor, and tissue
damage has occurred hours before the patient is placed on the operating
table. This is very different from the elective celiotomy in which the ana-
tomic condition is defined, the physiologic condition is stable, exposure is
maximized, and tissue damage can be minimized by good surgical tech-
nique. Because of these basic differences, a unique operative approach to
the trauma celiotomy has evolved. This approach has its foundations in the
principles of the elective celiotomy but is modified to meet the exigencies
of the patient ill extremis.
4
'
Strategically, the trauma celiotomy has two parts: damage control and
reconstruction. The damage control portion of the trauma celiotomy in-
cludes control of hemorrhage,S-S identification of injuries, and control of
Curr Probl Surg, August 1996 617
contamination. Damage control must be performed in the immediate
postinjury period. This phase is designed to accomplish those things nec-
essary to ensure the immediate survival of the patient. Reconstruction is
defined as definitive repair of organ injury. A severity-based grading sys-
tem for injuries to each organ can be used to develop treatment options for
each grade of injury within an organ.
The trauma patients in extremis account for approximately 10% of trauma
celiotomies. These patients do not have the physiologic reserve to tolerate
both damage control and reconstruction at the same operation. Consequently,
a new strategy has evolved. That strategy is based on the concept of physi-
ologic reserve. Before injury, all patients begin with a certain quantity of
physiologic reserve. The magnitude of this reserve is defined by host fac-
t01'S9 that include age,1O sex,9 genetic predisposition, and preexisting medi-
cal conditions. 11.12 At the instant of injury, the patient's physiologic reserve
begins to diminish at a rate that depends on the magnitude of the injury and
a quantity that depends on the length of transport time. The greater the
injury and the longer the transport time are, the greater the depletion of
physiologic reserve.
When physiologic reserve is depleted, the patient enters a state of ine-
versible physiologic "exhaustion," a condition our surgical forefathers termed
"ineversible shock." Before complete physiologic exhaustion occurs, the
patient enters a period that we have defined as in extremis. Patients in extremis
are characterized clinically by hypothermia, coagulopathy, and acidosis.
The time period between in extremis and irreversible physiologic exhaus-
tion is very small and may in certain patients represent only a matter of
minutes.
J3
The responsibility for monitoring physiologic reserve in the operating
room falls to the anesthesiologist. While the surgeon is performing the
essential phases of damage control (i.e., control of hemonhage, explora-
tion, control of contamination), the anesthesiologist must evaluate the
patient's physiologic reserve. If this evaluation indicates that the patient is
approaching physiologic exhaustion, the surgeon must terminate the pro-
cedure. The patient's abdomen is packed to control bleeding, the skin is
closed to help conserve body heat, and definitive repair of visceral injuries
is deferred. This minimalist procedure, designed to maximize the patient's
chances for survival, is termed the damage control celiotomy. 14
After the damage control celiotomy is performed, the patient in extremis
is taken from the operating room to the surgical intensive care unit, where
hypothermia, coagulopathy, and acid base balance are restored and car-
function is optimized. Termed "secondary resuscitation,"15
this period lasts from 36 to 48 hours and is orchestrated by the surgeon.
61Jl
Curr Probl Surg, August 1996
Massive transfusion of crystalloid and blood products,16 the application of
sophisticated hemodynamic monitoring,17 and the initiation of heroic lev-
els of ventilatory support may be required.
18
,19
This monograph is organized into four parts. The first section addresses
the essential components of the trauma celiotomy performed on the
day of injury, including the preoperative evaluation, the damage con-
trol phase, and factors that lead to recognition of the trauma patient ill
extremis. The second section details the secondary resuscitation, in-
cluding optimization of oxygen delivery, elimination of lactic acido-
sis, and the regeneration of physiologic reserve for patients ill eXTremis.
The third section is devoted to the planned return to the operating room,
which involves definitive surgical reconstruction of all intraabdominal
injuries and wound closure. If the patient's condition permits, any
extraabdominal injuries including orthopedic and maxillofacial repairs
also can be addressed. The final section outlines a grading system to
define the severity of each organ injury, outlines treatment options, and
suggests a grade-oriented ~ r e a t m e n t strategy.
Damage Control
Damage control techniques trace their origins from Halsted's original de-
scription of "intrahepatic packing" for severe liver injuries in 1908. The
popularity of intrahepatic packing waxed and waned over the succeeding
two surgical generations. Beginning in the late 1970s, a series of reports on
"perihepatic" packing for severe liver injuries emerged.
10
-
25
This concept
expanded rapidly into packing for other injuries
26
including injuries to the
organs of the retroperitoneum
27
and pelvis.
28
In 1983 Stone and colleagues
29
recognized intraoperative coagulopathy
as a harbinger of physiologic exhaustion and advocated packing and early
termination of the operative procedure in this group of patients. In 1993 a
series of reports from large trauma centers addressed the utility of abdomi-
nal packing. The nomenclature was expanded to encompass such terms as
"damage control celiotomy,"14 "abbreviated celiotomy,"30 and "staged
celiotomy"31 for trauma. These reports and others
32
-
35
have shaped the op-
erative concepts, defined the decision-making processes, and clarified the
objectives of the operative procedure.
Along with the development of the concept of the damage control
celiotomy came rapid advances in the field of surgical critical care for the
postoperative support of trauma patients ill extremis,'S These advances in-
clude improved techniques of cardiopulmonary monitoring,17 blood bank-
ing,36,37 ventilator support,19 and temperature contro1.
38
A developing man-
agement strategy considered the trauma celiotomy to be a continuum that
Curr Prabl Surg, August 1996 619
includes the primary resuscitation, damage control celiotomy, secondary
resuscitation, and reconstruction.
Damage control is no longer a procedure of last resort applied only in
desperation to patients who are near physiologic exhaustion. Instead, physi-
ologic exhaustion must be anticipated. The operation is designed to priori-
tize the temporary control of hemorrhage, identify injuries, and control
contamination before any effort at operative reconstruction is initiated.
Reconstruction should not begin until damage control is complete. Once
the injuries are defined and the physiologic reserve is quantified, repairs
are prioritized and a strategic plan for the operation is devised mid ex-
ecuted. If at any point the patient approaches critical levels of physiologic
reserve, the operative procedure must be terminated in an orderly fashion,
and the patient transported to the surgical intensive care unit for secondary
resuscitation.
Preoperative Evaluation
Clinical data obtained in the prehospital environment
39
,40 and the emer-
gency department contribute to the recognition of the patient ill extremis
and to the decision-making process in the operating room.
41
For patients
with blunt trauma, critical preoperative data'include information obtained
from the chest radiograph, anteroposterior pelvis radiographs, and arterial
blood gas. For patients with penetrating trauma, additional information is
gained from the location of the entrance and exit wounds. Any penetrating
wound that crosses the midline has the potential for major vascular injury.
For patients with blunt trauma, chest and anteroposterior pelvis radio-
graphs suggest the potential for major hemorrhage in the chest, pelvis, and
retroperitoneum. It is essential that the surgeon not focus on bleeding in
one body cavity to the exclusion of exsanguination in another body cav-
ity.S,42 The initial chest radiograph should be inspected for hemopneumo-
thorax and the presence of specific injuries including widened mediasti-
num,43-45 pulmonary contusion,46 and multiple rib fracturesY-49
Hemopneumothorax requires placement of a thoracostomy tube before the
operation. The presence of more than 2000 mL blood in the chest or con-
tinued bleeding of greater than 250 mLlhr from the chest tube are relative
indications for thoracotomy.5o
A widened mediastinum on the chest radiograph indicates the presence
of mediastinal blood. Ten percent of patients with blunt trauma and
mediastinal blood have an injury to the thoracic aorta,51 a surgical emer-
gency. In the stable patient the presence of a widened mediastinum
requires evaluation before a trauma celiotomy is performed. However,
in the unstable patient with intraabdominal injury, hemorrhage must be
620 Curr Prabl Surg, August 1996
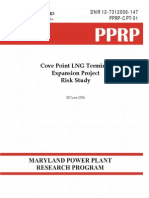
FIG. 1. Three fypes of pelvic fracture associated with the potential for major hemorrhage. From
left to right: straddle fracture, a fracture of all four pubic rami; the open book fracture, a diastasis
of the symphysis pubic of greater than 2.5 cm; the vertical sheer fracture, a fracture of both
anterior and posterior elements with vertical displacement of one hemipelvis by 1 cm or more.
controlled before the thoracic evaluation is performed.
52
After damage
control has been completed, the patient may be evaluated for injury to
the thoracic aorta with either transesophageal echocardiography53 or
aortography.
The pelvis radiograph provides valuable information in the patient with he-
modynamic instability. Isolated fractures of the pelvic rami rarely are hemo-
dynamically significant.5+56 However, three complex pelvic fractures (Fig. I)
are associated with the potential for massive retroperitoneal bleeding and he-
modynamic instability.57 These injuries include (1) the straddle fracture (de-
fined as a fracture of 4 pelvic rami), (2) the open-book fracture (a diastasis of
the pubic symphysis of greater than 2.5 cm), and (3) the vertical shear fracture
(fractures of both the anterior and posterior elements of the pelvis with dis-
placement of the entire hemipclvis by greater than I cm).
Arterial blood gases performed before operation define the patient's oxy-
genation, ventilation, and oxygen debt.
13
Patients with closed head injuries
who are not purposeful on physical examination or patients whose Sa0
2
is
less than 92% on 4 L of supplemental oxygen require immediate intubation
in the emergency department.
5o
The presence of a metabolic acidosis ac-
companied by a base deficit of greater than -8 mmolJL identifies a sub-
group of patients at high risk for physiologic exhaustion.
41
The purpose of the evaluation in the emergency department is to define
the need for operation and to collect essential pieces of physiologic data
that will guide subsequent decisions. Once an indication for an operation is
identified, the patient should be transported immediately to the operating
room. Time should not be wasted defining injuries in body systems that do
not require immediate repair.
The Procedure
The trauma celiotomy requires excellent communication among the sur-
geons, the anesthesiologist, and the nursing staff. Each teain member has a
Curr Probl Surg, August 1996 621
FIG. 2. The method of draping and the initial midline incision used for the patient with trauma.
The midline incision can be extended vertically into a median sternotomy and inferiorly to the
symphysis pubis. The patient is draped from the clavicles to the knees, allowing access to the
groin and the chest.
well-defined set of responsibilities and must remain focused on those re-
sponsibilities.
It is the responsibility of the nursing staff to prepare the patient for op-
eration. On arrival in the operating room, the patient with blunt trauma is
transferred to the operating table on a spine board. This procedure facili-
tates rapid movement and prevents further injury to the neck, back, or pel-
vis. The patient remains on the spine board throughout the trauma celiotomy,
and the board is removed only after the patient is transferred to the inten-
sive care unit.
622 Curr Probl Surg, August 1996
It is the responsibility of the anesthesiologist to place appropriate moni-
toring devices, ensure adequate oxygen delivery, and provide general ane,s-
thesia. Once the patient has been placed on the operating table, supple!TIen-
tal oxygen, electrocardiographic monitoring, and pulse oximetry are
initiated. A radial artery catheter and additional intravenous catheters are
placed, as indicated. As the surgical team scrubs, the patient is anesthetized
and intubated, and the airway is secured.
Adequate oxygen delivery requires the administration of crystalloid and
blood products and the maintenance of an adequate arterial oxygen satura-
tion. An 8F introducer catheter (Arrow, Inc., Reading, Pa.), placed into
either the subclavian or internal jugular position, is designated as the resus-
citation line. This catheter is attached to the high-volume infuser (Level I
Technologies, Inc., Rockland, Mass.) so all fluids, both crystalloid and
blood products, can be warmed to 40 C and delivered through this single
line. The hematocrit, platelet count, and arterial blood gases are measured
at this time. These critical tests, which have a short turnaround time, pro-
vide valuable intraoperative information about trends in the patient's physi-
ologic reserveY
The patient is prepared from the clavicle to the knees (Fig. 2). This al-
lows access to the chest, if thoracotomy58 is needed, and to the groin, if
femoral access is required.
59
A midline incision extending from the xi-
phoid process to the symphysis pubis is preferred. This incision has the
advantage of providing adequate exposure to all four quadrants of the ab-
domen.
The patient with a large retroperitoneal hematoma
60
and a complex pel-
vic fracture presents the surgeon with a difficult dilemma. If the space of
Retzius (the anterior reflection of the retroperitoneum) is opened, tamponade
of pelvic venous bleeding is lost, and the patient may exsanguinate. There-
fore in patients with anyone of the complex pelvic fractures (Fig. 1) iden-
tified on the emergency department anteroposterior pelvis radiograph, the
linea alba is opened only to the umbilicus. A handheld retractor is used to
elevate the anterior abdominal wall, permitting the surgeon to determine
whether blood is present in the space of Retzius. If no blood is present in
the space of Retzius, the abdominal incision is extended to the symphysis
pubis. If significant blood is present in the space of Retzius, every effort is
made to perform the operation through the supraumbilical incision, be-
cause opening the retroperitoneum leads to loss of tamponade and, poten-
tially, exsanguination. In the patient with a large retroperitoneal hematoma
defined by a preoperative computed tomography (CT) scan, a bilateral,
subcostal incision provides excellent access to the liver and spleen, but this
incision makes exposure of the lower quadrants more difficult.
Curr Prabl Surg, August 1996 623
FIG. 3. The division of the falciform ligament and the placement of suction catheters to evacuate
blood from the upper quadrants of the abdomen, facilitating exploration.
Once the linea alba is incised, the peritoneum is identified. A bluish
discoloration under the peritoneum indicates significant intraabdominal
hemorrhage. If this discoloration is present, the surgeon must notify the
anesthesiologist to expect a transient episode of hypotension at the time
the peritoneum is opened. Rapid crystalloid administration is necessary to
counteract the effects of this loss of tamponade.
The most critical time during the trauma celiotomy' occurs when the
abdomen is opened. As intraperitoneal tamponade is released, the surgeon
must make a gross estimate of the intraabdominal blood loss. Concurrently,
the anesthesiologist must determine the patient's current blood volume and
must communicate to the surgeon the patient's physiologic reserve. If nec-
essary, the surgeon can reduce intraabdominal blood loss by temporarily
occluding the aorta at the diaphragmatic hiatus or by applying manual pres-
sure to the bleeding sites.
The first step in the trauma celiotomy is the division of the falciform
ligament. Although the falciform ligament may be difficult to visqalize
when the abdomen is full of blood, its exposure is facilitated by placing a
suction catheter on both sides of the ligament (Fig. 3). The ligamentum
Teres is identified, and clamps are applied. The falciform ligament is then
divided to its junction, with the coronary ligaments overlying the hepatic
veins and vena cava. Division of the falciform ligament allows complete
exploration and packing of the liver without further damage to the liver
parenchyma.
61
624 Curr Probl Surg. August 1996
FIG. 4. Manual compression of a liver laceration provides for temporary hemostasis.
Control of hemorrhage. Because exsanguination is the major cause of
death during the trauma celiotomy, control of hemorrhage is critical to the
operation.
42
.
62
Many patients are bleeding from multiple sites. Therefore
initial efforts should be directed at the temporary control of all bleeding
sites. Temporary control is obtained by four-quadrant packing or direct
pressure to a bleeding point. An adjunct to temporary control is aortic con-
trol either at the diaphragmatic hiatus or via resuscitative. thoracotomy.42.62
The purpose of temporary control is to provide the surgeon with adequate
time to achieve exposure, define injuries, and develop a strategic plan for
the operation. At the same time, the anesthesiologist is restoring the circu-
lating blood volume and building physiologic reserve.
Four-quadrant packing is designed to tamponade bleeding sites and ab-
sorb free blood within the abdomen. The surgeon at the right of the table
provides robust countertraction on the right abdominal wall. The surgeon
at the left then sweeps a hand over the superior surface of the right lobe of
the liver, rapidly identifying areas of injury. After the initial assessment of
liver injury is performed, celiotomy packs are placed over the dome' and
entire right lobe of the liver. If the liver is injured, the technique of pack
placement is crucial, because the liver parenchyma, stripped of its capsule,
is friable.
61
Rough placement of packs can exacerbate liver damage and
bleeding. To avoid damage the surgeon places a hand on either side of the
liver defect, positioning the liver edges in apposition (Fig. 4). Packs are
then placed over the hand while the assistant keeps sturdy traction on the
Curr Probl Surg, August 1996 625
right upper quadrant. After six to eight packs have been placed, the surgeon's
hand is removed, and the abdominal wall is released. This places pressure
on the packs and tamponades the injured liver. Packs are then positio'ned
under the liver to create additional pressure against the diaphragm arid liver.
Caution must be used, however, to avoid compression on the inferior vena
cava.
The right paracolic gutter must now be exposed. The surgeon gathers the
small bowel out of the pelvis and sweeps the bowel toward the midline.
Packs are then placed in the right paracolic gutter and pelvis. Adjunctive
measures such as warm celiotomy pads or bowel bags require additional
time for placement and offer no advantages at this stage of the operation.
After the right paracolic gutter is packed, traction is applied to the left
anterior abdominal wall. The surgeon then sweeps a hand over the left lobe
of the liver and palpates the spleen to identify injuries.
Regardless of the presence of an injury, the left upper quadrant is packed
tightly, with packs placed at the base of the diaphragm which provide di-
rect pressure on the spleen and the left lobe of the liver. Again, the bowel is
moved toward the midline, and the left paracolic gutter is packed. Before
packs are placed in the pelvis, the sump suction catheter is positioned in
the pouch of Douglas to absorb blood and allow inspection of organs. The
pelvis is then packed. The upper quadrants are packed in all cases of blunt
trauma with hemoperitoneum regardless of whether injuries are found at
the initial evaluation. Once packs are placed in all four quadrants, virtually
all hemorrhage within the true abdomen is temporarily controlled.
The process of four-quadrant packing takes 3 to 4 minutes. During this
time information has been obtained about the presence of a pelvic hematoma
and injuries to the liver and spleen. At the same time an initial look at the
retroperitoneum was 9btained while the paracolic gutters were exposed.
The process of four-quadrant packing is most beneficial in patients with
blunt trauma. In the setting of penetrating trauma and exsanguination, con-
trol of the aorta is a useful adjunct for temporary control of hemorrhage.
Aortic control can be achieved through either the abdomen
63
or the chest.6-l
We recommend abdominal control. Control of the abdominal aorta is initi-
ated by palpating the aorta adjacent to the spine at the level of the diaphrag-
matic hiatus. Blunt finger dissection through the gastrohepatic ligament
then allows the placement of the aortic occluder at the hiatus. This tech-
nique is relatively simple to perform. However, it is ineffective for injuries
at the level of the celiac axis, because there is not sufficient room for de-
finitive vascular control of these injuries.
The alternative to abdominal vascular control is the resuscitative
thoracotomy advocated by a number of authors.5s.6H7 In this approach the
626 Curr Probl Surg, August 1996
Inferior Mesentertic < 5
Aorta
Left Colic =0
Distal Mesenteric> 50 -----'
Left Hepatic < 10 Hepatic =0
- Left Gastric =0
Right Hepatic < 10 '
Proper Hepatic < 10 111\' S I '-0
penlc-
Gastroduodenal =0 "'It R,",' > 90
Right Renal> 90 L
Superior Mesenteric> 95
FIG. 5. Diagram summarizes the risk of ischemia associated with the ligation of named arteries
within the abdomen.
unstable patient undergoes a thoracotomy for aortic control before under-
going abdominal celiotomy. In theory, this approach provides proximal
aortic control before abdominal tamponade is released. This approach has
the disadvantages, however, of substantial heat loss associated with open-
ing a second body cavity, increasing the operative time, and contributing to
additional surgical bleeding.
Our treatment algorithm calls for abdominal aortic control except in the
patient with a large, supracolonic, retroperitoneal hematoma. A supracolonic
hematoma suggests a supraceliac aortic injury. In this situation we proceed
with resuscitative thoracotomy&! before exposing the supraceliac aorta.
Once temporary control of hemorrhage has .been achieved, the surgeon
communicates to the anesthesiologist an initial' assessment of the injuries.
Curr Probl Surg, August 1996 627
FIG. 6. The temporary control of contamination is achieved with Babcock clamps.
In turn, the anesthesiologist communicates an assessment of the patient's
physiologic status. Blood and blood products should be administered at this
time. The hematocrit and arterial blood gases should be measured. Most
important, the surgeon should use this respite to create a strategic plan for the
operation, including options for definitive control of hemorrhage.
Definitive control of hemorrhage begins with a distinction between pa-
renchymal bleeding and surgical bleeding. Parenchymal bleeding, typi-
cally from the liver or spleen, usually can be controlled with surgical pack-
ing. Surgical bleeding (i.e., bleeding from major blood vessels) requires
either ligation,8 repair,68 or balloon catheter tamponade.
69
-
73
Ligation is the most common method of definitive hemorrhage control.
This technique should be considered for all unnamed vessel bleeding and
for most major vessel hemorrhage in the patient ill extremis. Fig. 5 summa-
rizes the risk of tissue ischemia resulting from major vessel ligation. The
surgeon can deal with the ischemic consequences of ligation subsequently.
This concept is especially important in the patient with multiple bleeding
sites in whom protracted efforts at repair may prove lethal.
42
Exploration. Once control of hemorrhage is achieved and blood is re-
moved from the abdomen, the process of systematic exploration of the
abdomen begins. Careful exploration is designed to identify both intra-"
peritoneal and retroperitoneal injuries and must proceed in a disciplined
fashion. Unfortunately, packing at the site of parenchymal bleeding
may preclude a regimented approach. For each patient the pattern of
exploration is defined by the effectiveness of temporary packing. If
temporary packing does not control hemorrhage, the surgeon must as-
sume a major vessel injury exists, and consequently exploration and
definitive control of that bleeding must become the first priority. In
most instances, however, temporary packing will control hemorrhage,
and exploration can proceed in an orderly fashion. This process begins
628 Curr Probl Surg, August 1996
TABLE 1. Operative treatment of retroperitoneal hematoma
Location
Zone I
Zone II
Zone III
Blunt
Explore
Observe
Observe
Penetrating
Explore
Explore
Explore
with pack removal. Packs remote from suspected injury sites are removed
first. This improves exposure and maximizes working room within the ab-
domen before a major injury is unpacked.
In the patient with a suspected injury to the liver or spleen, initial'maneu-
vers include lifting the transverse colon superiorly and removing the packs
from the right paracolonic gutter and right pelvis. Packs are then removed
from the left lower quadrant, and the remaining blood is suctioned from
the pelvis. A self-retaining retractor (e.g., Balfour) is placed, the small
bowel and transverse colon are eviscerated, and the ligament of Treitz is
identified. Exploration of the entire small bowel and initial control of con-
tamination begin. Starting at the ligament of Treitz, the bowel is inspected
and areas of perforation are controlled with clamps (Fig. 6). Areas of
hematoma in the mesentery are noted. If the mesentery is disrupted and
bleeding freely, hemostasis is achieved by placing clamps or ligatures.
After inspecting the small bowel, the surgeon explores the large bowel,
working in a clockwise fashion. Although small bowel perforations are
usually obvious, the only evidence of a large bowel injury may be a small
pericolonic hematoma. These hematomas must be explored.
At this juncture packs remain in place in both upper quadrants. The small
and large bowel have been explored, and initial control of contamination
has been achieved with clamps or the placement of large silk sutures. In
addition, the presence' of a retroperitoneal hematoma has been determined
by assessing both paracolic gutters and the pelvis.
Injuries to the retroperitoneum are often unsuspected before the opera-
tion.
74
Their presence may profoundly alter the plan of operation. The cru-
cial decision revolves around whether to open and explore the retroperito-
neal hematoma. This decision is based on two pieces of information: the
anatomic location of the hematoma and the mechanism of injury.61.75
Retroperitoneal hematomas are classified into three anatomic zones: (1)
zone I, the centromedial area of the retroperitoneum, which includes the
duodenum and pancreas and the major abdominal vasculature, (2) zone II,
lateral to zone I, including the kidney and retroperitoneal portion of the
colon and its mesentery, and (3) zone III, including the entire pelvis.
60
Table 1 outlines the strategy for retroperitoneal exploration based on the
anatomic zone and mechanism of injury.
Curr Probl Surg, August 1996 629
TABLE 2. Indications for damage control celiotomy
Physiology
Base deficit> -15 mmol/L
Temperature <35
0
C
Coagulopathy
Bowel edema
Host factors
Age >55 yr
Preexisting disease
Associated injuries
Closed head injury
Widened mediastinum
Unstable, complex pelvic fracture
COlltrol of cOlltamillatioll. Definitive control of contamination is per-
formed with either primary repair or resection. Single-layer, primary repair
is appropriate for isolated injuries to the stomach, small bowel, or colon
that involve less than 50% of the bowel diameter. However, in patients with
multiple bowel injuries or large defects with gross contamination, resec-
tion is preferred.
During the initial exploration clamps were placed on the small bowel to
control contamination. Once the decision to resect bowel has been made,
the surgeon lifts these clamps and places a staple line proximal and distal
to the injured area. If there are multiple areas of complex injury and the
amount of injured small bowel is less than 50% of the small bowel length,
a single resection is preferred. The GIA stapler (U.S. Surgical Co., Norwalk,
Conn.) is used proximally and distally to the injured area'. The mesentery is
divided, and hemostasis is achieved with ligatures. No effort is made to
reconstruct the bowel at this juncture. The divided ends are replaced in the
abdomen.
26
The technique of single resection is simple, fast, enhances ex-
posure, and is applicable to both the small bowel and colon.
7
6-78 Further-
more this approach creates a single anastomosis and eliminates grossly
contaminated tissue, decreasing the incidence of an anastomotic leak and
postoperative infection.
79
8o
The Decision
Once the initial control of hemorrhage has occurred, the true abdomen has
been explored, the retroperitoneum has been assessed, and contamination
has been controlled, the decision must be made to proceed with definitive
treatment and reconstruction or to terminate the operative procedure'. This
decision is based on the patient's physiologic reserve and injury pattern
(Table 2). Communication with the anesthesiologist is critical.
The anesthesiologist's role is to maintain and monitor three vital func-
630 Curr Probl Surg, August 1996
TABLE 3. Trauma mortality: preexisting disease"
Condition
Cirrhosis
Congenital coagulopathy
Chronic lung disease
Ischemic heart disease
Diabetes mellitus
Relative odds of mortality
4.6
3.2
1.8
1.8
1.2
tions: oxygen delivery, temperature control, and coagulation. Each of these
critical factors can be assessed with relatively simple techniques in the
operating room, and if anyone of these factors is abnormal, the operation
should be terminatedY35
Base deficit is a sensitive measure of both the degree and the duration of
inadequate oxygen delivery. Rutherford and colleagues
41
demonstrated that
young patients without a closed head injury who had a base deficit of 15
mmollL had a 25% mortality rate. If the base deficit does not promptly
respond to the administration of blood, then the patient's physiologic re-
serve is compromised, and the operation should be terminated.
The core temperature is most effectively monitored in the operating room
with an esophageal temperature probey82 Patients in whom the core tem-
perature falls below 35 C are at high risk for coagulopathy, myocardial
depression, and cardiac arrest.
83
Failure to maintain the core temperature
above 35 C is an indication to terminate the operation.
8ol
In patients who have bled more than 6 units, depletion of clotting factors
is a potential problem.
85
Under ideal circumstances the replacement of clot-
ting factors is based on laboratory data.
83
However, the long turnaround
time combined with the time necessary to thaw the products mandates
empiric administration
3
? of fresh-frozen plasma and platelets to the patient
ill extremis.
The other major determinant of physiologic reserve is host factors.
9
In
patients with preexisting medical conditions
l
l,12 (Table 3) physiologic re-
serve is diminished, so the surgeon should have a low threshold for using a
damage control celiotomy. Patients 55 years of age or older who have sig-
nificant hemodynamic instability at any time during the operation are can-
didates for damage control celiotomy.41
The final factor that influences the decision to terminate the trauma
celiotomy is the pattern of extraabdominal injury. In patients with a wid-
ened mediastinum
42
and a high suspicion for aortic transection, we may
elect to terminate the celiotomy early, take the patient to the angiography
suite, define any aortic injuries, and, if necessary, return the patient to the
operating room for aortic repair. Other injuries that might affect the deci-
Curr Probl Surg. August 1996 631
FIG. 7. The method of ropid towel clip closure of the skin. The superior towel clips have their
handles pointed caudally so as not to interfere with portable chest rodiographs.
sion to terminate the celiotomy are the presence of complex pelvic frac-
tures,86 multiple long bone fractures,87 or a closed head injury.42 The pres-
ence of multiple orthopedic injuries often mandates surgical repair at a
later date, simplifying the decision to terminate the celiotomy.
Definitive Packing
Once the surgeon has elected damage control celiotomy rather than defini-
tive repair, definitive packing is initiated. The packing process is based on
three fundamental principles: (I) pressure stops bleeding, (2) pressure yec-
tors should recreate tissue planes, (3) tissue viability must be protected.
The goal is to stop or slow bleeding temporarily until metabolic derange-
ments can be corrected.
Skin Closure
In the damage control celiotomy, speed and efficiency are important. Tem-
porary closure of the skin spares the fascia for definitive closure at the time
632 Curr Probl Surg, August 1996
of Furthermore skin closure enhances return to normo-
thermia and minimizes fluid loss. Several techniques for damage control clo-
sure have been described in the literature.
33
,88-91 We prefer towel clip closure as
described by Feliciano and Burch,92 \vhich provides a sturdy closure and mini-
mizes skin damage. Towel clips should be placed 1 cm apart and 1 cm from
the skin edges with the upper towel clip handles directed caudal and the lower
towel clip handles directed cephalad (Fig. 7). The wound and towel clips are
then covered with a surgical towel, and a large transparent adhesive drape (3M
Medical, St. Paul, Minn.). This technique provides a watertight seal facili-
tates heat gain and simplifies nursing care.
Open abdomen technique. If at the initial operation the surgeon is
faced with a patient with massively edematous small bowel, an engorged
liver, multiple abdominal packs, and virtually no remaining abdominal
domain, skin closure may not be possible. Several techniques have been
proposed for this particularly difficult problem.
9o
,9I,93-95 The ideal tech-
nique for management of the open abdomen provides protection for the
bowel, minimizes loss of temperature and fluid, and maximizes abdomi-
nal domain. The treatment of the first three issues directly affects sur-
vival. Loss of abdominal domain determines functional outcome and re-
source consumption.
We currently use a three-layer temporary covering of abdominal contents.
The first layer, which is in direct contact with the abdominal viscera, is a
plastic bowel bag (Becton Dickinson Co., San Jose, Calif.). Two sides of the
bag are slit, and the drawstring is removed. This provides a large inexpensive
sheet of inert plastic that is simply draped over the exposed abdominal con-
tents and tucked under the fascia. No attempt is made to secure this sheet to the
fascia, because sutures placed at this time simply weaken the fascia for subse-
quent closure. The plastic bag is then covered with a dry surgical towel, which
also is tucked under the fascia, but care is taken to avoid placing the towel in
direct contact with the bowel. The entire abdominal wall is then covered with
a sterile transparent drape (3M Medical).
This three-layer approach protects the bowel and minimizes bowel edema,
serosal irritation, and the risk of fistula formation while improving the
chances of performing an anastomosis during the reconstruction phase.
Concurrently, temperature and fluid losses are minimized, decreasing skin
irritation and the risk of body fluid contamination of nursing personnel. In
addition, if there is continued swelling of the viscera, the transparent drape
will expand, maintaining some degree of tamponade but preventing the
development of an abdominal compartment syndrome. While the patient's
abdomen is being closed, the intensive care unit is notified to prepare for
rewarming and cardiopulmonary support.
Curr Probl Surg. August 1996 633
Restoration of Physiologic Reserve
The restoration of physiologic reserve in the patient ill extremis begins
once the abdomen is closed. The urgency of resuscitation is dictated by the
presence of the deadly triad of hyp6thermia,96 coagulopathy,97 and acido-
sis.
98
Secondary resuscitation includes aggressive rewarming, replacement
of red blood cells and clotting factors, correction of acid-base imbalance,
and the aggressive use of cardiopulmonary support.
Warming the Patient
Hypothermia is defined as a core body temperature less than 35 C.
i5
Hy-
pothermia leads to progressive abnormalities including dysrhythmias, shifts
in the oxyhemoglobin dissociation curve, and inhibition of the clotting
cascade.
98
-
loo
Both the electrophysiologic and the inotropic functions of the
heart are depressed by cold.
101
This condition is commonly manifested by
a decreased cardiac output and ventricular dysrhythmias.
102
Pulmonary ar-
tery catheters are placed in all patients with hypothermia on arrival in the
intensive care unit. The core temperature is monitored continuously by the
right ventricular temperature probe (Baxter Model 93A-754H, Deerfield,
Ill.). Although the placement of a pulmonary artery catheter in an irritable
heart may cause ventricular dysrhythmias, we have not encountered this
difficulty.
In addition to its detrimental effects on the heart, hypothermia shifts the
oxyhemoglobin dissociation curve to the left. As a result, hemoglobin can-
not release oxygen to the tissues effectively. This complicates the problem
of poor oxygen delivery resulting from hemorrhage. Furthermore the en-
zymes ofthe clotting cascade are Consequently,
hypothermia interferes with an 'already taxed clotting system.
The treatment of hypothermia involves a dual strategy: prevention of
additional heat loss and providing heat gain.
15
In the operating room the
goal is to minimize heat loss. All celiotomies are performed with the room
temperature at approximately SSO F, the thermoneutral zone for humans.
105
Fluids are warmed to 40 C with the Level I counter-current warming sys-
tem. Finally, every effort is made to open as few body cavities as possible
and to keep the initial phase of surgery brief.
In the intensive care unit the goal shifts from preventing heat loss to
providing heat gain. 102 This can be accomplished, in part, by using conduc-
tive warming devices (Bair Hugger, Augustine Medical, Inc., Eden Pra,irie,
Minn.), heating and humidifying air in the ventilator circuit, and counter-
current warming of all intravenous fluids.
Gentilello and colleagues
38
,106 has reported significantly enhanced rewarm-
ing times with continuous arteriovenous rewarming. However, use of this
634 Curr Probl Surg, August 1996
technique is limited. These patients often have profound hypotension, and
their systemic blood pressure is insufficient to drive the system at flow
rates necessary for rewarming. Under these circumstances volume aug-
mentation or vasopressors may reestablish a sufficient systolic blood pres-
sure to drive flow through the rewarrner. Alternative heroic measures for
the treatment of profound hypothermia include continuous veno-venous
bypass and body cavity lavage.
102
,107
Coagulopathy and Massive Transfusion
Coagulopathy is the second component of the deadly triad found in pa-
tients ill extremis. It is first suggested in the operating room by diffuse
oozing from cut surfaces.
29
The presence of coagulopathy in the patient
with trauma results from the complex interaction of multiple factors on the
enzymes of the clotting cascade.
108
The specific activity of these enzymes
is very sensitive to temperature
lO3
and acid-base balance.
98
In addition, de-
ficiencies in anyone of the cascade components severely impairs the body's
ability to control medical bleeding.
I09
The presence of ongoing blood loss is the best clinical monitor of the
coagulopathic patient ill extremis.
15
These patients often require massive
transfusion, now defined as administration of greater than 20 units of red
blood cells in 24 hours. I 10 This type of heroic resuscitation has given rise to
a body of massive transfusion literature
ll
Q..1I3 and the development of llms-
sive transfusion The development of these protocols com-
bined with recent advances in blood banking makes massive transfusion a
viable therapeutic strategy. 1I5 There are, however, risks associated with
massive transfusion including transfusion reaction,1I6,1I7 immunosuppres-
sion,1I8 and virus transmission.
1I9
Mild transfusion reaction occurs in approximately 1% of units transfused.
Severe hemolytic transfusion reaction occurs in approximately 1 per 6000
units transfused and almost universally is associated with administrative er-
ror.
120
The likelihood of administrative error is magnified by the urgency of the
massive transfusion scenario. This underscores the need for creation, imple-
mentation, and strict adherence to massive transfusion protocols.
The concept of transfusion-related immunosuppression emerged from
the transplantation literature and has been confirmed in patients with
oncologic complications, trauma, 12I and burns. 118,122 The critical issue is a
balance between the maintenance of oxygen-carrying capacity and if!lmu-
nosuppression. If oxygen delivery is inadequate or the immunosuppression
is significant, multiple organ failure results.
123
In a report on massive trans-
fusion by Wudel and colleagues,16 only 10% of 92 patients receiving mas-
sive transfusion died of multiple organ failure and sepsis. Consequently,
Curr Probl Surg, August 1996 635
TABLE 4. Risk of posttransfusion hepatitis C associated with levels of blood component
exposure
115
Units of exposure
2
5
10
15
20
25
Risk (%)
0.48
1.2
2.4
3.5
4.7
5.8
From Morris JA Jr. Wiley TR. Reed GN. et al. Safety of the blood supply: surrogate testing and transmis-
sion of Hepatitis C after massive transfusion. Ann Surg 1994;219:51726.
although the indications for minor transfusion may be controversial, it is
clear that despite the risk of immunosuppression, more than 50% of pa-
tients with trauma undergoing massive transfusion survive; approximately
75% of these survivors returned to a productive lifestyle within the year
after injury.12.f
The incidence of viral transmission after massive transfusion is depen-
dent on several factors: the prevalence of viral disease in the blood supply,
the sensitivity of screening techniques, and the competency of the blood
banking system.
115
Although the human immunodeficiency virus has re-
ceived the most widespread attention from the media and general public,
hepatitis is actually the leading cause of disability and death attributable to
transfusion.
115
Hepatitis C accounts for 90% of posttransfusion hepatitis.
115
Table 4 delineates the upper limits of risk for hepatitis transmission per
unit of blood product transfused.
1I5
The treatment of coagulopathy involves the replacement of deficient
soluble (fresh-frozen plasma)12
5
and cellular (platelets)83.126 factors.
37
,97 The
bleeding patient ill extremis requires aggressive replacement of platelets to
maintain a platelet count greater than 100,000 per unit and supplementa-
tion of fresh-frozen plasma to maintain the prothrombin time below 16
seconds.
The concept ofa massive transfusion protocol has been pioneered by Frykberg
and colleagues
37
at the University of Florida. This protocol introduces the con-
cept of a massive transfusion "pack," which is administered only to actively
bleeding patients ill extremis. This pack consists of 5 units of packed red blood
cells, I units of fresh-frozen plasma, and 5 units of platelets. The pack is
supplemented by 10 units of cryoprecipitate, if the fibrinogen level is less than
100 mgldl. After two massive transfusion packs are administered, blood is
drawn for laboratory analysis of the prothrombin and partial thromboplastin
times, platelets, and fibrinogen. With a similar protocol at our institution, we
found that our patients ill extremis had a mean blood product resuscitation
636 Curr Probl Surg, August 1996
requiring 35 units of packed red blood cells, 13 units of fresh-frozen plasma,
and 21 units of platelets for a mean exposure of 72.3 units per patient. I IS ,
In the bleeding patient ill extremis, the aggressive administration of red
blood cells allows time for the surgeon to correct underlying physiologic
causes of coagulopathy. Although replacement therapy of clotting compo-
nents is important, it is not a cure for unrecognized surgical bleeding, nor
will it be helpful in the patient with hypothermia.
Cardiopulmonary Management
The approach to cardiopulmonary resuscitation focuses on the recogni-
tion17 and treatment of oxygen debt.
123
Oxygen debt is defined as the cu-
mulative difference between the amount of oxygen delivered and the amount
of oxygen required by the tissues. When oxygen delivery is inadequate to
support tissue oxygen consumption, cells transition from aerobic to anaero-
bic metabolism and produce lactic acid.
The concept of oxygen debt represents a major shift in the definition of
shock. No longer is the shock state viewed as a decrease in blood pressure,
cardiac output, or tissue perfusion. Instead, shock is viewed as the cumula-
tive imbalance between oxygen delivery and oxygen consumption over
time. The magnitude of the oxygen debt depends not only on the extent of
the imbalance but also on the length of time that the imbalance exists. Thus
even small discrepancies between oxygen delivery and oxygen consump-
tion can create a large oxygen debt in patients who have prolonged trans-
portation times to the hospital.
Oxygen debt, just like bank debt, requires repayment with interest. Shoe-
maker and colleagues
l27
have shown general improvements in survival and
morbidity among patients undergoing complex surgical procedures and
patients with sepsis when supranormal values
l27
of oxygen delivery are
attained.20.I23.128 These observations have led to a strategy for the restora-
tion of physiologic reserve. IS The therapeutic goal is to repay the oxygen
debt, defined as a return to a normal serum lactate level as rapidly as pos-
sible. To achieve this goal, oxygen delivery is maximized and, where pos-
sible, oxygen consumption is minimized. The process of the repayment of
oxygen debt requires between 24 and 36 hours.
lls
,129
Oxygen delivery. Mathematically, the oxygen delivery index is a func-
tion of the cardiac index, arterial oxygen saturation, and hemoglobin con-
centration. All of these parameters are measured easily, and the a u g ~ e n t a
tion of oxygen delivery constitutes the mainstay of our therapeutic strategy.
We begin by raising and then maintaining the hematocrit (a surrogate for
hemoglobin concentration) to 35% to 40%. Although patients who have
undergone an elective operation may tolerate a hematocrit of 20%, patients
Curr Prabl Surg. August 1996 637
in extremis require additional oxygen-carrying capacity to repay the oxy-
gen debt expeditiously.39,4o
The cardiac index is dependent on the interaction of preload, afterload,
and contractility. To enhance cardiac index, we begin by augmenting the
preload. The most accurate indicator of preload in a patient in extremis,
especially the patient requiring high levels of ventilatory support, is the
right ventricular end diastolic volume index (EOVI).130 The EOVI is a func-
tion of right ventricular ejection fraction and is easily measured at the bed-
side with a right ventricular ejection fraction pulmonary artery catheter.
Chang and colleagues13 I have determined that the optimal EOVI for the
patient in extremis is between 80 and 120 mL. The patient with an EOVI
less than 80 mL requires additional volume, whereas the patient with an
EOVI greater than 120 mL rarely benefits from further volume expansion.
Within the 80 to 120 mL range, the patient's optimal preload is variable
over time and must be determined with a ventricular function curve.
Patients in extremis often bleed 3 to 4 total blood volumes during the
first 24 hours after injury. The optimal preload is changing constantly, de-
pending on both the degree of bleeding and capillary leak.
132
Although the
manipulation of preload and optimization of EOVI require the most atten-
tion,133 we also routinely manipulate contractility and afterload by adding
adrenergic agonists (e.g., dopamine, dobutamine, norepinephrine) or, rarely,
vasodilators (e.g., nitroglycerin, nitroprusside).
Oxygen consumption. Oxygen consumption is the difference between
the amount of oxygen presented to the tissues and the amount of oxygen
remaining in the blood after circulation through the t i s s u ~ s . The Fick prin-
ciple states that the product of the difference between arterial and venous
oxygen content and the total cardiac output yields the oxygen con-
sumption. Although oxygen consumption is difficult to measure, the
mixed venous oxygen saturation (Sv0
2
) can be measured continuously
with a pulmonary artery catheter. For the trauma resuscitation continu-
ous Sv0
2
monitoring is the best screening tool for determining whether
the oxygen delivery is meeting the tissue oxygen demand.
134
An Sv0
2
of 65% to 70% suggests' that tissue oxygen needs are being met. An
Sv0
2
of less than 65% suggests either inadequate oxygen delivery or,
occasionally, excessive oxygen consumption (e.g., shivering, fever,
seizure activity).
In summary, the therapeutic goal of the cardiac component of the sec-
ondary resuscitation is to repay the oxygen debt, defined as the elimina-
tion of lactic acidosis. This goal is achieved initially by ensuring that oxy-
gen delivery exceeds oxygen consumption, indicated by an Sv0
2
greater
than 65%. If the Sv0
2
is less than 65%, oxygen delivery is inadequate and
638 Curr Prabl Surg, August 1996
TABLE 5. End points of cardiopulmonary resuscitation
Sv0
2
>65%
CI >3 L/min/m
2
EOVI 90 - 120 mL
SVRI >1500 dynes/ems
Sa0
2
>95%
Hematocrit >35%
021 >550 mL/dL
Qs/Q, <20%
SvO,. MIxed venous oxygen saturation; C/. cardiac index; EDV/. end-<liastolic volume index; SVR/. sys-
temIc vascular resistance index; SaO" peripheral arterial oxygen saturation; 00,1. oxygen delivery sys-
tem; OslO,. shunt fraction.
the components of oxygen delivery (e.g., cardiac index, Sa0
2
, hematocrit,
and oxygen consumption) should be reassessed. The hematocrit should be
35% or greater, the Sa0
2
should be greater than 94%, and the cardiac
index should not be less than 3.5 L1min. If the Sv0
2
is depressed, the
cardiac index is most likely the problem. Of the three determinants of
cardiac output (preload, afterload, contractility), the most likely derange-
ment is in preload.
The functions of the heart and the lungs are inextricably interwoven in
the complex dynamic of oxygen delivery. Often, interventions that help the
heart fulfill its delivery function impair the ability of the lungs to transport
oxygen across the pulmonary capillary membrane.
132
The patient with trauma may have pulmonary function abnormalities for
a variety of reasons, including preexisting lung disease,1I pulmonary con-
tusion
l35
or laceration, aspiration pneumonitis, adult respiratory distress
syndrome, or injuries to the chest wall, ribs;H-49 or diaphnigm.
9
.
19
The basic
problem of posttraumatic pulmonary dysfunction can be viewed as severe
mismatching of ventilation and perfusion, resulting in an increased pulmo-
nary venous admixture or shunt fraction. An increased shunt fraction re-
sults in impaired oxygenation. To calculate the shunt fraction, a pulmonary
artery catheter must be used.
For patients with arterial hypoxemia, defined as an Sa0
2
of less than
94%, the ultimate therapeutic goal is a shunt fraction of less than 20%15
while receiving an Fi0
2
of less than 40%. Ventilatory treatment of the
patient ill extremis requires a delicate balance between positive end-expi-
ratory pressure (PEEP), Fi0
2
, and preload. To reduce the shunt fraction,
treatment begins with administration of oxygen with an Fi0
2
of 100% and
5 cm Hp of PEEP.19 The PEEP is increased incrementally by 3 to 5 cm
Hp while the Fi0
2
is decreased while maintaining an Sa0
2
of greater than
94%. However, to attain these goals, many patients ill extremis require
more than 15 cm Hp of PEEP. High levels of PEEP increase intrathoracic
pressure (making pulmonary capillary wedge pressure measurements in-
Curr Probl Surg. August 1996 639
MORTALITY CURVES
1.00
>-
.-::
'iii
0.75
t:
0
:E
-
0.50 0
>-
.:::
:c
etl
0.25
.0
0
~
c.
0.00
0.00
0 5 10 15 20 25 30
Base Deficit
FIG. 8. The probability of mortality associated with a given base deficit. Note the steep nature
of the curve between the base deficit of -15 to -19. In patients older than 55 years of age or in
those with a closed head injury, the curve is shifted to the left, suggesting that damage control
should be initiated at a base deficit of -8 in this subgroup of patients.
accurate), decrease venous return, and, consequently, decrease the cardiac
index. Patients ill extremis may require preload augmentation in excess of
25 L of crystalloid and 20 units of blood products in the' first 24 hours to
maintain adequate cardiac index and oxygen delivery in the setting of high
PEEP and continued bleeding'.19
In summary, the interaction of cardiac and pulmonary function in the
trauma patient ill extremis is complex and dynamic. The short-term thera-
peutic goal is to maintain a constant Sv0
2
greater than 65%. Table 5 out-
lines the cardiopulmonary end points that are necessary to improve perfu-
sion and to repay the oxygen debt.
Acid-Base Balance
The previous sections have described that discrepancies between tissue
oxygen delivery and tissue oxygen consumption lead to an oxygen debt
and a transition from aerobic to anaerobic metabolism. Several indicators
of oxygen debt are useful in the clinical evaluation of the patient ill extremis.
These include the base deficit,39.4
o
.136 serum lactate leveI,2 arterial pH, and
the anion gap. Of these, the base deficit and serum lactate are the most
helpful during the initial resuscitation.
640 Curr Probl Surg, August 1996
The determination of base deficit is a standard part of the routine arterial
blood gas analysis. It is readily available in most emergency departments,
has a rapid turnaround time, and is inexpensive. For these reasons we de-
pend on base deficit as a guide in the initial resuscitation,41 whereas serum
lactate levels are measured every 4 hours during the secondary resuscita-
tion. A normal serum lactate i n d i c a ~ e s that physiologic reserve has been
restored and that the patient can return to the operating room for elective
reconstruction.
31
Base deficit. Base deficit is defined as the amount of base required to
titrate 1 L whole blood to a pH of 7.40 at normal physiologic vaiues of
Pa0
2
, PaC0
2
, and temperature. The normal range of base deficit is +3
to -3 mmollL. The base deficit has been shown to correlate with volume
requirements and mortality in patients with trauma.3IAOAI.136.137 In a hemor-
rhagic canine model the base deficit was demonstrated to be superior to
blood pressure, cardiac output, or serum lactate level in predicting mortal-
ity and estimating the oxygen debt.
13
Base deficit is an expedient sensitive measure of both the degree and the
duration of inadequate perfusion. Rutherford and colleagues
41
demonstrated
that a base deficit of -15 mmollL in a patient younger than 55 years of age
without a head injury is a marker for identifying the patient ill extremis.
The steep slope of the mortality curve (Fig. 8) strongly suggests that all
surgical intervention should be terminated as the base deficit approaches
-15 mmollL. The mortality curve shifts to the left in elderly patients or
patients with a head injury. Yet, the slope of the curve is unchanged, sug-
gesting that in this group of patients procedures should be'terminated if the
base deficit approaches -8 mmollL.
Serum lactate. Elevations of the serum lactate (greater than 2.5 mg/dL)
indicate that the oxygen debt has not yet been fully repaid. Although the
amount of lactic acid does not define the type of intervention needed, it is
extremely helpful for assessing quantitatively the progress of the resuscita-
tion.
20
138
It has been known for some time that the severity of lactic acido-
sis can be used to predict outcome in critically ill patients.
137
Recently,
Abramson and colleagues
139
have expanded their work to demonstrate that
patients who fail to clear lactic acidemia in 48 hours have little chance of
functional survival. In short, if the base deficit or serum lactate is worsen-
ing, then the components of oxygen delivery must be reevaluated.
There are several caveats to using the base deficit and lactate as guides to
resuscitation. First, if exogenous sodium bicarbonate is administered, the
stoichiometric relationship between base deficit and lactate is uncoupled.
In this instance only serum lactate can be used to guide further resuscita-
tion. For this and other physiologic reasons, bicarbonate is administered
Curr Probl Surg. August 1996 641
only if the serum pH is less than 7.09. Second, lactate and hydrogen ions
may not diffuse into the extracellular environment at the same rate. This
may account for some of the quantitative differences between the levels' of
lactate and b'ase deficit. However, trends in lactate and base deficit almost
always move in the same direction. Finally, a "wash-out phenomenon" is
occasionally seen. This is characterized by an initial improvement in the
serum lactate followed by a plateau that lasts for several hours despite all
other indications that the resuscitation is proceeding well. This is believed
to be a transient phenomenon resulting from the reperfusion of previously
ischemic tissue beds.
In summary, the base deficit and serum lactate level are complementary
end points by which to judge the progression of resuscitation, predict out-
come, initiate damage control, and monitor the secondary resuscitation.
Once the serum lactate is normal and the oxygen debt is repayed, the pa-
tient is ready to return to the operating room for reconstruction.
Special Considerations in Secondary Resuscitation
General measures. During the secondary resuscitation all patients ill
extremis receive antibiotics empirically, stress ulcer prophylaxis, and pneu-
matic compression devices. The administration of nutrition should begin
as soon as the patient is no longer receiving vasoactive drugs and the serum
lactic acid levels are normal. An intracranial pressure monitor is placed in
all patients ill extremis with a severe, closed head injury (defined as a
Glasgow coma score of <8 ) once coagulopathy is controlled. loW Recent
evidence suggests that optimizing oxygen delivery minimizes secondary
injury to the brain in these patients.l.fl
Two unique complications of damage control celiotomy may occur dur-
ing the secondary resuscitation: small bowel evisceration and abdominal
compartment syndrome.
31
W
1
.f.f Small bowel evisceration develops in ap-
proximately 10% of patients undergoing towel clip closure. Almost always,
this results from inadequate sedation of the patient. As a preventive mea-
sure patients are sedated aggressively to protect the wound closure, de-
crease oxygen consumption, and maintain comfort. Sedation consists of a
continuous infusion of 10 to 20 mglhr of morphine sulfate or 100 to 500
/lglhr of fentanyl supplemented with intravenous neuroleptics or benzodi-
azepines.
Patients ill extremis commonly require more than 20 units of blood prod-
ucts and 25 L of crystalloid during the secondary resuscitation. This'crys-
talloid load is distributed throughout the extracellular space, resulting in a
generalized edema. This extracellular volume expansion is for the most
part benign and will dissipate over a 7- to IO-day period of posttraumatic
642 Curr Probl Surg, August 1996
diuresis. However, in the abdomen the extracellular volume increase can
be problematic. Massive intraabdominal bleeding compounded by t h i r ~
space fluid shifts increases intraabdominal pressure and may result in the
development of abdominal compartment syndrome.
145
Abdominal compartment syndrome. The abdominal compartment
syndrome is defined as impairment of organ function resulting from
increased intraabdominal pressure. This pressure must be lowered if
organ dysfunction is to be reversed. Richardson and Trinkle
lH
demon-
strated experimentally that increased intraabdominal pressure results
in elevated end-inspiratory pressures and diminished cardiac output,
presumably resulting from impaired venous return. The lungs and kid-
neys are the two organs most profoundly affected by an elevated
intraubdominal pressure. Pulmonary dysfunction results from mechani-
cal impairment of diaphragmatic excursion. Renal dysfunction results
either from impaired cardiac index or compromised renal perfusion
and inadequate venous drainage.
On clinical evaluation the abdominal compartment syndrome is charac-
terized by a tensely distended abdomen, increasing peak inspiratory pres-
sures, intractable hypercarbia, and oliguria.31.142 The diagnosis of abdomi-
nal compartment syndrome is a challenge, because the patient ill. extremis
has other reasons for abdominal distention, pulmonary dysfunction, and
oliguria. Abdominal distention may result from pack placement,
intraabdominal bleeding, extravasation of fluid, and bowel edema result-
ing from reperfusion injury. Hypercarbia may result from the inability of
the ventilator to deliver adequate tidal volumes to ensure 002 excretion. In
our recent series
3
! we found that the most reliable clinical indicator of ab-
dominal compartment syndrome was failure of ventilation. Patients' peak
inspiratory pressures rose to greater than 85 Cm of H
2
0, and the PaC0
2
rose abruptly. Although intravesicular pressure monitoring has been advo-
cated to diagnose the presence of the abdominal compartment syndrome,
we have not found this to be consistently useful. We feel justified in pro-
ceeding to decompressive celiotomy purely on the basis of the findings of
tense abdominal distention, hypercarbia, and peak inspiratory pressures
greater than 85 cm H
2
0.
We have recently reviewed a series of 16 patients with abdominal com-
partment syndromeY One third of these patients were found on explora-
tion to have surgical bleeding within the abdomen. This condition presents
the surgeon not only with the dilemma of when to perform decompressive
celiotomy but also where to perform it-at the bedside or in the operating
room. Patients with abdominal compartment syndrome are undergoing ven-
tilation at the upper limits of the ventilator's mechanical capacity. Con-
Curr Prabl Surg, August 1996 643
TABLE 6. Indications for emergent return to the operating room
Blunt trauma
Normothermic but bleeding >2 units/hr
Abdominal compartment syndrome
with ongoing blood loss
Penetrating trauma
Bleeding >15 and hypothermia
Normothermic but bleeding >2 units/hr
Abdominal compartment syndrome
with ongoing blood loss
sequently, significant risk is associated with transporting these patients to
the operating room. If the patient's transfusion requirements have slowed,
decompressive celiotomy can be performed in the intensive care unit. How-
ever, an operating room must be available should unexpected surgical bleed-
ing or a missed injury be encountered.
Emergent retllrn to the operating room. The central dilemma facing
the surgeon caring for the patient ill extremis with ongoing bleeding is
when to return to the operating room.
31
,129 All patients with surgical bleed-
ing should undergo reexploration in the operating room, where missed in-
can be identified and controlled and packing can be reinforced
or replaced, The problem is distinguishing between medical bleeding and
surgical bleeding in the patient ill extremis. .
The need for emergent return to the operating room during the secondary
resuscitation occurs in approximately 15% of patients (Table 6). We be-
lieve that normothermic patients who bleed more than 2 units per hour
despite adequate clotting factor replacement or hypothermic patients with
penetrating trauma who bleed more than 15 units of packed red blood cells
after the damage control celiotomy is performed should be returned imme-
diately to the operating room. Patients with blunt trauma who remain hy-
pothermic regardless of transfusion requirements should not be returned to
the operating room until the core temperature has normalized.
Angiography with selective embolization of bleeding vessels is a poten-
tial alternative for patients with ongoing Although the
risks of transport remain, angiography can identify and embolization may
control surgical bleeding. This is an attractive alternative in the patient ill
extremis who has not yet had high levels of intraabdominal pressure.
Embolization is appealing when feasible, because emergent return to the
operating room virtually commits the surgeon to postoperative use of the
open abdominal technique, since bowel edema and pack placement may
preclude skin approximation. This complicates postoperative temperature
control and diminishes the tamponade effect of packs.
In summary, after the damage control celiotomy is performed, the pa-
tient ill extremis is transported to the surgical intensive care unit, where the
body temperature is restored, blood products are replaced, and oxygen de-
644 Curr Probl Surg, August 1996
TABLE 7. Indications for elective return to the operating room
Temperature
Coagulation
Cardiovascular
Pulmonary
Acid-base balance
>36
0
C
PT <15
Platelets >75.000jmm
3
SV0
2
>65%
CI >3.5 Ljminjm
2
80 <EDVI <120
Hematocrit >35%
Sa0
2
<:95%'
Fi0
2
<0.45'
Shunt fraction<30%'
Serum lactate normal
*These are relative, not absolute, indications.
PT, Prothrombin time; RD
2
fraction of inspired oxygen.
livery is optimized. The repayment of oxygen debt is heralded by the clear-
ance of lactic acid, signaling that physiologic reserve has been restored and
that the patient is ready to return to the operating room for reconstruction
(Table 7).
Reconstruction
In most cases the unpacking procedure is relatively elective, and its timing
is dictated by the patient's clinical condition. Ideally, the operation occurs
when hypothermia, metabolic acidosis, and coagulopathy have been corrected
and the mixed venous oxygen saturation and serum lactate are normal.
Although one study reports prolonged packing of 7 to 10 days with low
infection and mortality rates,32 little is gained by delaying the unpacking
procedure once the intermediate goals are reached. Further delays may
increase the incidence of abdominal sepsis. Our average time to unpacking
is 2 days, and patients receive broad-spectrum antibiotics during this period.
In the stabilized patient returning electively for unpacking and recon-
struction, consideration must be given to the repair of injuries outside the
abdomen. These associated injuries frequently involve other subspecialties
such as orthopedics and maxiHofacial surgery. Repair of these injuries should
be prioritized, and after abdominal reconstruction is performed, if the
patient's physiologic condition permits, reconstruction of these injuries may
occur. Ideally, all long bone fractures should be repaired within 48 hours
after injury.
Procedure
Once the patient has returned to the operating room for reconstruction, one
experienced person should be assigned specifically to monitor the patient's
physiologic response. This is best accomplished by a person not involved
Curr Probl Surg, August 1996 645
with the technical aspects of the reconstruction or the delivery of anesthe-
sia but intimately knowledgeable about the patient's initial procedure and
secondary resuscitation. '
Before the reconstruction begins, all monitors should be in place and
functioning. These include (1) an arterial line for blood pressure monitor-
ing and blood sampling, (2) pulse oximetry for monitoring of arterial oxy-
gen saturation, (3) capnography for monitoring end-tidal carbon dioxide,
(4) pulmonary artery catheter for monitoring of mixed venous oxygen satu-
ration and hemodynamics, (5) core temperature monitoring, usually through
the pulmonary artery catheter, (6) a urinary catheter, and (7) adequate venous
access defined as two large-bore, 8.5F introducers.
Laboratory data must be followed periodically throughout the recon-
struction including hematocrit, platelet count, prothrombin time, ionized
calcium, magnesium, and arterial blood gas. The room temperature is main-
tained at 8SO F. As in the initial procedure, the abdomen, chest, and both
groins should be prepared and draped in a sterile fashion.
If the patient has abdominal compartment syndrome, the surgeon must an-
ticipate that abdominal decompression will precipitate a potentially lethal
reperfusion syndrome.J1 This syndrome must be treated presumptively with
the administration of 2 L of a solution containing two ampules of sodium
bicarbonate and 50 gm mannitol per liter of Y2 normal saline solution.
Mter adequate volume administration is performed, every other towel
clip is removed, and the assigned person monitors the ventilatory pressures
as the remaining towel clips are removed. Peak inspiratory pressures com-
monly decrease substantially during removal of towel clips. Because the
lungs will have quickly regained room for expansion, CO
2
excretion rises
as previously unventilated areas are now ventilated. The tidal volume and
PEEP should be decreased appropriately.
After the abdomen is opened, peritoneal fluid and clot are evacuated. If
the peritoneal fluid is purulent or foul-smelling, aerobic and anaerobic cul-
tures are obtained. The celiotomy pads, which were placed in the area of
hemorrhage at the initial procedure, are not disturbed at this time.
At this juncture the abdomen is reexplored to identify missed injuries
from the initial operation and to reassess previously identified injuries.
After reexploration is performed, gastrointestinal continuity is reestablished.
If multiple bowel resections were performed at the initial procedure, it is
imperative to ensure that segments are not twisted on their mesentery. Con-
tamination usually is controlled at the initial procedure. Therefore after
adequate irrigation, debridement, and assessment of perfusion are performed,
primary colon anastomosis is almost universally possible.
The final phase of reconstruction involves the removal of the packs placed
646 Curr Probl Surg, August 1996
in the area of hemorrhage at the initial procedure. The celiotomy pads are
slowly and gently removed. The goal is hemostasis and debridement of
devitalized tissue. A Pulsevac (Zimmer, Warsaw, Ind.) is useful for irrigat-
ing and debriding devitalized tissue. Standard techniques of repair are then
instituted.
Drains are placed depending on the organ injured and grade of injury. We
only use a closed-drainage system and preferentially use a Jackson-Pratt
fluted 10 mm drain (Johnson & Johnson, Arlington, Tex.) within the true
abdomen. Establishment of enteral nutrition is a primary goal during the
postreconstruction period. In a review of our experience with feeding
jejunostomy, we found a relatively high complication rate. 140 Consequently,
the placement of a nasojejunal fceding tube is our preferred method of
enteral access.
After unpacking is done but before abdominal closure is performed, a
routine radiograph of the abdomen should be obtained to exclude the pres-
ence of retained celiotomy pads. It is common for the celiotomy count
from the initial procedure to be incorrect. In addition, celiotomy pads from
the initial procedure may be confused with the celiotomy pads placed dur-
ing reconstruction, leading to an inaccurate pack count.
Optionsfor Closure
Primary fascial closure at the termination of the staged celiotomy is pos-
sible in 80% of cases. Primary fascial closure under tension may be tempt-
ing but should be avoided, because this can lead to abdominal compart-
ment syndrome, wound dehiscence, and fascial destruction.
If fascial closure is performed, the choice of suture is essential because
these wounds are contaminated. An absorbable suture limits the duration
of foreign body exposure and the potential for wound infection and fascial
dehiscence.69.149.150 In theory, a monofilament suture is preferred under these
circumstances. However, no. 1 polyglyconate (Maxon; Davis & Geck,
Danebury, Conn.) has been found to achieve the same goals and retain a
higher tensile strength than polyglactin.69.151.152
For similar reasons a continuous rather than interrupted closure is pre-
ferred. A heavy running monofilament absorbable suture has been found to
be more expedient, with greater wound strength and a similar incidence of
wound disruption.
152
.
155
We prefer not to use retention sutures because of
the risk of increasing abdominal pressure and resulting abdominal com-
partment syndrome. If retention sutures are deemed necessary, parallel place-
ment of horizontal mattress sutures is superior to perpendicularly placed
retention sutures. 156
Techniques that may be useful in assisting primary fascial closure in-
Curr Probl Surg, August 1996 647
clude the introduction of relaxing incisions or lengthening procedures with
the anterior and posterior rectus sheaths.
157
Because all of these wounds ,are
contaminated, the skin and subcutaneous tissue should be left open and
prepared for delayed primary closure.
If primary fascial closure cannot be obtained, an alternative mode of
closure is preferable to an open abdomen. In patients with an open abdo-
men, hypothermia will be difficult to correct, and large insensible fluid
losses can be anticipated. Several alternative modes of closure have been
described, including closure of the skin only, closure with synthetic mesh
(both absorbable and nonabsorbable), and formal plastic and reconstruc-
tive techniques of flap closure.
Whenever possible, the abdomen should be closed to prevent ongoing
heat and fluid losses and to provide compression to the viscera, which will
prevent further visceral edema and promote resolution. One alternative is
simply to close the skin, leaving the fascia open. If the skin closure is
performed with a running monofilament suture, this may serve as the de-
finitive closure for this hospitalization. This will leave the patient with a
large ventral hernia, which can then be repaired electively. The advantage
of this technique is the avoidance of further operations during this hospital-
ization. It also preserves the fascia for the definitive closure at a later date.
Nonabsorbable mesh has been used for many years. Polypropylene
(Marlex, Davol, Covington, Ga.) mesh has been used extensively since it
was described in 1959.
158
Since then, its advantages and disadvantages have
been well described. Polypropylene can be used to cover large defects,
even those with gross wound contamination.
159
The mesh fs generally placed
in a subfascial position and sutured to the fascia with a running or inter-
rupted horizontal mattress suture. The disadvantages to the use of polypro-
pylene mesh include enterocutaneous fistulas and mesh extrusion. If pos-
sible, omentum or other tissue should be interposed between the bowel and
polypropylene mesh. Enterocutaneous fistulas and mesh extrusion may also
be prevented by full-thickness myocutaneous flap coverage ofthe mesh rather
than healing by secondary intention or split-thickness skin grafting.
159
The same techniques can be used with absorbable mesh. Dexon mesh
(Davis & Geck) is available in a 7 x 9 inch sheet, and Vicryl mesh (Ethicon,
Somerville, N. J.) is available in 12 x 12 inch sheets. We prefer the smaller
Dexon mesh unless the larger Vicryl mesh is required for surface area.
Although the Vicryl mesh has smaller interstices, it has a tendency to tear
at the sites of suture fixation when placed under tension. Both of these
meshes allow for the egress ofperitoneal exudates and can be used in wounds
with gross contamination. The absorbable meshes can be placed in a
subfascial position similar to the nonabsorbable meshes or can be sutured
648 Curr Probl Surg, August 1996
TABLE 8. Liver injury grading
Grade Description
Capsular tear <1 cm in depth
II Capsular tear 1-3 cm in depth
<10 cm length
III Capsular tear >3 cm in depth
IV Parenchymal disruption 250/0-75% of hepatic
lobe or 1-3 Couinaud's segments within a
single lobe
V Parenchymal disruption
>75% of hepatic lobe or >3 Couinaud's
segments within a single lobe
Injury to retrohepatic vena cava
ICD-9 AIS90
864.02 2
864.12
864.03 2
864.13
864.04 3
864.04 4
864.14
5
5
From Moore EE, Cogbill TH. Malangoni MA, et al. Organ injury scaling. Surg Clin North Am 1995;75:294-
302.
to the skin, preserving the fascia for future use. The use of either type of
absorbable mesh allows for several long-term treatment options, including
mesh removal and primary closure, mobilization of the mesh to an intra-
peritoneal position with fascial closure over the mesh, healing by second-
ary intention, and split-thickness skin grafting. Despite enzymatic degra-
dation of absorbable mesh, not every patient has a hernia, and hernias that
do occur can be repaired electively.
Formal plastic and reconstructive myocutaneous flaps can also be used
to reconstruct the abdominal wall. These procedures should be reserved for
the definitive repair at a later date. The immediate goal is healing without
infection, and a finite rate of late hernia formation is acceptable.
Organ Repair
Introduction
This section details the specific treatment of individual organ injuries and
is divided into two parts: organs of the true abdomen and organs of the
retroperitoneum. The difficult decision to explore the retroperitoneum and
techniques of retroperitoneal exposure are discussed in detail. Each organ
discussion begins with two tables. The first table delineates the American
Association for the Surgery of Trauma (AAST) description of organ injury,
the appropriate ICD-9 code for the injury grade, and the Abbreviated In-
jury Score
l60
of injury severity by grade. To compare treatment outcomes,
surgeons must adopt a common language for grading injuries. The AAST
grading system provides such a severity-based language. The second table
provides a list of treatment options for injuries to individual organs. The
Curr Probl Surg. August 1996 649
TABLE 9. Treatment options: control of hepatic bleeding
Grade Treatment options
I, II Argon beam coagulation
Hemostatic agents
III Argon beam coagulation
Hemostatic agents
Pringle maneuver and hepatotomy with finger fracture and precise ligation
Resectional debridement
Viable omental grafting
IV Argon beam coagulation.
Hemostatic agents .
Pringle maneuver and hepatotomy with finger fracture and precise ligation
Resectional debridement
Viable omental grafting
Perihepatic packing
text describes techniques to enhance surgical exposure to the organs and
the appropriate treatment options for each grade of organ injury.
Organs of the True Abdomen
Liver. The liver is the most commonly injured organ in patients with trauma.
Hepatic trauma has been the subject of two previous volumes of Currellt
Problems ill Surgery. In 1976, Dr. E. Truman Mays161 wrote "Hepatic
Trauma," and in 1989, Feliciano and Pachter
J62
wrote "Hepatic Trauma
Revisited," detailing progress made in the treatment of hepatic injuries during
the intervening 13 years.
Table 8 outlines a grading system for liver injuries. More than 80% of all
liver injuries are grades I, II, or III. If these injuries are isolated and identi-
fied on a preoperative CT scan, they rarely require surgical intervention.
163
Large parenchymal defects (grade IV) and hepatic venous injuries (grade
V) still carry a collective mortality rate of 30% and 66%, respectively, and
present a challenge even to experienced surgeons.
Exposure. All liver injuries are approached initially through a midline
abdominal incision. 1M Extension to the chest by either right anterior
thoracotomy162 or median stemotomy165.166 is rarely necessary and may be
associated with loss of temperature control. Placing the patient in reverse
Trendelenburg position enhances exposure, improves access to the right
lobe of the liver, and allows extravasated blood to collect in the pelvis.
Immediately after entering the abdomen, the surgeon should divide the fal-
ciform ligament,&.t remove clot, and manually explore the liver surface. If a
large defect is encountered, manual compression of the liver parenchyma
will control the bleeding and allow placement of packs. Packs are placed
over the surgeon's hand, protecting the liver surface from further damage.
650 Curr Probl Surg, August 1996
FIG. 9. The Pringle maneuver. A vessel loop on the porta hepatis includes the common bile
duct, portal vein, and hepatic artery. The falciform ligament has been divided.
Therapy. Table 9 outlines the standard procedures for control of hepatic
hemorrhage. Recent experience with nonoperative management of subcap-
sular hematomas
I63
,I67-169 defined by CT scan indicates that contained sub-
capsular hematomas discovered in the operating room slJould not be ex-
plored. In addition, both blunt and penetrating injuries that are not bleeding
at the time of surgery do not r ~ q u i r e treatment.
170
Bleeding grades I and II hepatic injuries can be treated with argon beam
coagulation,171 hemostatic agents,172-176 individual vessel ligation,177 and
the placement of a viable omental graft.
178
,179 Injuries of grade III, IV, or V
require control of the hepatoduodenal ligament (Pringle maneuver) before
definitive control of bleeding can be achieved. The hepatoduodenal liga-
ment contains the three major structures of the porta hepatis: the common
hepatic artery, the portal vein, and the common bile duct.
J. Hogarth Pringle, ISO in 1908, described occlusion of the portal circula-
tion in animals. The Pringle maneuver remains a mainstay of treatment for
severe liver injuries. It is performed by placing an index finger through the
foramen of Winslow and palpating the common hepatic artery between the
thumb and index finger. No attempt should be made to dissect individual
structures within the porta hepatis. Although many authors describe Pringle
control with a vascular clamp, we prefer to encircle the porta hepatis with
an elastic vessel loop and occlude vascular inflow to the liver with the Potts
Curr Probl Surg. August 1996 651
technique or a Rummel tourniquet (Fig. 9). This approach facilitates expo-
sure and keeps the field free of extraneous instruments.
Recently, Pachter and Spencer
l81
documented that warm ischemia time
to the liver in patients with the Pringle maneuver can exceed 60 minutes.
182
This is sufficient time to accomplish repair of grades III and IV injuries.
Failure of the Pringle maneuver suggests a grade V injury or an aberrant
derivation of the lobar hepatic artery.162 Studies of hepatic anatomy suggest
the presence of an aberrant lobar hepatic artery in approximately 25% of
cases. If present, the aberrant lobar hepatic artery must be individually
controlled for the Pringle maneuver to be successful.
After the porta hepatis has been controlled, several minutes are required
for residual blood to drain from the liver. Packs must remain in place dur-
ing this period. Many surgeons use this time to divide the ligamentous
attachments to the liver. However, this should be approached with caution
because the liver, stripped of its capsule, is exceedingly friable. Even small
amounts of shear from a misguided effort to enhance exposure will disrupt
vessels and ducts. Once the injury is exposed, the surgeon must grade it,183
place it in the context of the patient's overall condition, and make the deci-
sion to repair the injury or definitively pack the lesion.
If the decision is made to repair a grade III liver injury, it should be
performed under Pringle control. The coronary ligaments are divided and
the liver is mobilized to the midline. If necessary, the finger fracture tech-
nique
177
is used to expose and ligate vessels deep within the liver paren-
chyma. The argon beam
171
is used extensively to coagulate the entire raw
surface of the injured liver. Once bleeding is controlled: the elastic vessel
loop is released. Areas of breakthrough parenchymal bleeding are identi-
fied and coagulated. A viable omental graft
l78
is then placed. The graft is
based on the epiploic 'vessels and serves several purposes. Most important,
it protects the liver parenchyma from the potentially destructive process of
pack removal and may aid the reparative process by increasing blood sup-
ply,179 combating sepsis;84 decreasing dead space,18S and sealing small bile
leaks.
'86
Grade IV andV injuries are managed with definitive packing under Pringle
control. Definitive packing22.2u4.3s should provide effective hemostasis,
obliterate dead space within the liver, allow for atraumatic pack removal,
and, finally, should be simple to perform. Over the past decade we have
evolved a three-layer technique for definitive liver packing. The firs,t layer
is a viable omental graft, which is secured either to the falciform ligament
or to the liver capsule with only two or three sutures of 3-0 silk. The second
layer is a simple celiotomy pack placed over the entire viable omental
graft. This second layer facilitates pack removal because packs adhere to
652 Curr Probl Surg, August 1996
FIG. 10. A, Avena cavagram demonstrates extravasation of blood from the retrohepatic vena
cava. Note the laparotomy packs in the area and the presence of towel clips. B, Avena cavagram
in the same patient 6 weeks later confirming complete healing of the vena cava after pack
removal on the tenth postoperative day.
tissue, not other packs. The third layer is the pressure layer. The pressure
layer consists of rolled packs, providing tamponade to c<;>ntrol parenchy-
mal bleeding. Packs are placed on either side of the liver defect and on the
inferior surface ofthe liver so that the cumulative vector forces reapproximate
tissue planes. After definitive pack placement is done, the elastic vessel
loop surrounding the porta hepatis is released, and the packs are observed
for breakthrough bleeding. If this does not occur, damage control is com-
pleted, and rapid towel clip closure is initiated.
Retrohepatic caval injuriesI70.'87.192 are rare, complex, and usually are
accompanied by exsanguinating hemorrhage. In patients with blunt trauma
these lesions universally occur just below the diaphragm at the confluence
of the vena cava and hepatic veins (Fig. 10). Table 10 delineates the multiple
therapeutic strategies that have been proposed to approach these injuries. How-
ever, the mortality remains very high. Although our experience with packing
these rare injuries is limited, our evolving strategy includes aggressive pack
placement, postoperative documentation of the caval injury, and delayed re-
construction. At the initial procedure, we place Surgicel (Johnson & Johnson)
over the caval bleeding site. A single celiotomy pad is placed over this mate-
rial, and the liver is then packed in the standard fashion. After the operation,
Curr Probl Surg. August 1996 653
TABLE 10. Techniques for repair of grade V liver injuries
Perihepatic packing
Hepatotomy and direct repair
Atrial caval shunt
Total vascular isolation
Vena-venous bypass
once the patient has stabilized, we perfonn vena cavagraphy to confinn the
presence of a caval injury. If no caval injury is found, the patient is ret.umed to
the operating room after physiologic reserve is restored, and all packs are
removed. If a caval injury is documented, the pressure layer of packs is re-
moved at 48 hours, if possible. However, the Surgicel and its protective pack
remain in place for 7 to 10 days. If there is continued bleeding from the vena
cava and nonnothennia is achieved, the patient may be returned to the operat-
ing room for an attempt at repair with total vascular isolation193-195 of the liver
or veno-venous bypass.
196
Special considerations. Ten millimeter, flat-fluted Jackson-Pratt drains
are placed at .the time of definitive repair for all grade III, IV, or V injuries.
There is no indication for decompression and drainage of the common bile
duct in patients with liver injuries.
Porta hepatis. The hepatoduodenal ligament contains the portal vein,
hepatic artery, and the common bile duct, collectively known as the porta
hepatis. Injuries to this area are rare,197,198 often lethal because of
exsanguination,199 and commonly missed at the initial trauma celiotomy.2oo
Although there may be subtle signs of injuries to the porta hepatis docu-
mented by CT scan,20l the diagnosis of these injuries rarely is made before
the operation.
199
At explor'ation these injuries manifest either with
exsanguinating hemorrhage from the area of the gallbladder or with bile
staining or contained hematoma within the hepatoduodenal ligament.
Temporary control of hemorrhage in the porta hepatis is achieved by
direct pressure, either manually or by pack placement. Exposure is obtained
by mobilizing the right colon, including the hepatic flexure, medially in a wide
Kocher maneuver. The liver and gallbladder are retracted superiorly, and an
index finger is placed into the foramen of Winslow. The structures of the
hepatoduodenal ligament are palpated, and in most cases bleeding from the
portal vein can be controlled with a modified Pringle technique. Definitive
control can then be achieved by placing vessel loops proximally and distally to
the index finger. In certain instances, exposure to the porta hepatis may be
enhanced by ligation and division of the cystic duct.
Injuries to the portal vein. Injuries to the portal vein carry a universally
high mortality rate.
202
,203 In a recent review of porta hepatis injuries from
654 Curr Probl Surg, August 1996
eight level I trauma centers, Jurkovich and others
2
O describe 55 patients
with portal vein injuries and a 64% mortality rate. Two thirds of these
injuries were located in the hepatoduodenal ligament, which is relativCIy
accessible. However, one fourth were located in a retropancreatic position
at the junction of the superior mesenteric and splenic veins. Exposure of
the retropancreatic portal vein may be enhanced by the division of the pan-
creas. However, this technique requires performance of a distal
pancreatectomy and splenectomy either at the initial operation or at the
time of reconstruction.
There are two realistic alternatives for patients with portal vein injuries:
lateral venorrhaphy or ligation. If lateral venorrhaphy is possible, this is
the treatment of choice; however, if simple repair is not possible or if there
are multiple bleeding sources within the abdomen, ligation is the preferred
alternative. Although the literature
l99
,20.J suggests improved survival with
primary repair of portal vein injuries, it is likely that this reflects the fact
that ligation was used only as a treatment of last resort. Stone and col-
leagues
205
report a 13% survival rate in a group of patients with portal vein
ligation used as a last resort. In a second group of patients in whom ligation
was immediately used and simple venorrhaphy was not possible, the sur-
vival rate improved to 80%.
Patients undergoing portal vein ligation have significant sequestration of
fluid in the splanchnic bed and can be expected to have massive bowel
edema lasting for approximately 72 hours. Both abdominal compartment
syndrome and venous infarction of the bowel remain theoretic concerns,
although neither has yet been reported after portal vein'ligation. Fascial
closure at the time of reconstruction may be difficult because of bowel
edema; however, these patients often can be closed at some point during
the initial hospitalization. Two cases of portal hypertension have been re-
ported in long-term follow-up of patients with portal vein ligation.
2
O
Injuries to the hepatic artel)'. Although the repair versus ligation contro-
versy regarding the therapy of portal venous injury remains, ligation is
considered the treatment of choice in isolated hepatic artery injuries. There
are numerous isolated reports of lobar liver necrosis and even total liver
necrosis
2
06,207; however, many of these patients also have concomitant por-
tal venous injuries or periods of prolonged shock. The pioneering studies
ofMays208-211 suggest that hepatic arterial flow is reconstituted via collaterals
in less than 24 hours. Ischemic necrosis of the gallbladder has been re-
ported after ligation of both the right and the left hepatic arteries.
212
This
suggests that thorough evaluation of the gallbladder should be performed
at the time of reconstruction or that cholecystectomy be performed as part
of the initial procedure after hepatic artery ligation.
Curr Probl Surg, August 1996 655
TABLE 11. Spleen injury scale
Grade Injury description ICD9 AIS-90
Capsular tear, <1 cm parenchymal depth 865.02 2
865.12
II Capsular tear, 1-3 cm parenchymal depth that does not
involve a trabecular vessel 865.02 2
865.12
III Laceration of >3 cm parenchymal depth involving 865.03 3
trabecular vessels 865.13
Ruptured subcapsular or parenchymal hematoma;
intraparenchymal hematoma >5 cm or expanding
IV Laceration involving segmental or hilar vessels producing 4
major devascularization (>25% of spleen)
V Shattered spleen or hilar vascular injury that 865.04 5
devascularizes spleen 865.14 5
From Moore EE, Cogbill TH. Malangoni MA. et al. Organ injury scaling. Surg Clin North Am
1995;75:294302.
Injuries to the bile duct. To date, only 160 cases of bile duct injury re-
sulting from trauma have been reported.
2
O Suture repair with 3-0 Vicryl is
suitable for simple injuries involving less than 50% of the circumference of
the duct. Complex injuries with greater than 50% duct transection or with
segmental tissue loss require Roux-en-Y biliary enteric reconstruction.
2
O
Occasionally, destruction of the ampulla or the intraduodenal portion of
the common bile duct will necessitate pancreaticoduodenectomy.213
In summary, injuries to the portal vein have a high mortality and should
be managed either with simple venorrhaphy, if possible, or ligation. Inju-
ries to the hepatic artery should be managed by ligation and carry an ap-
proximately 10% incidence of hepatic lobar necrosis and a higher inci-
dence of ischemic cholecystitis. Unilateral lobar bile duct injury should be
ligated, simple extrahepatic bile duct injuries may be repaired without plac-
ing a stent, and complex bile duct injuries are best managed by Roux-en-
Y biliary enteric anastomosis either at the initial operation or at the time of
reconstruction.
Spleen. The treatment of splenic injuries is based on the degree of injury
to the spleen and the patient's physiologic condition at the time of
tion. Table 11 outlines the AAST grading system for the spleen, and Table 12
summarizes treatment options by injury grade. Isolated grade I, II, and III
injuries rarely require operation. Incidental injuries to the spleen that are not
bleeding require no therapy unless the patient is coagulopathic. For the pa-
tient in extremis, even minor splenic injuries are treated with expeditious
splenectomy. To assess the injury to the spleen completely, it must be mobi-
lized to the This requires sharp division of the phrenolienal and
656 Curr Probl Surg, August 1996
TABLE 12. Treatment options: spleen
Grade Treatment options
I, II Topical agents, argon beam coagulator
III Interrupted sutures, horizontal mattress sutures over a pedicle of omentum or
Teflon pladgets, mesh splenorrhaphy
IV Partial splenectomy, mesh splenorrhaphy, or splenectomy
V Splenectomy
lienorenal ligaments. The lienocolic and gastrolienal ligaments are ligated
and divided. The grade of splenic injury can then be determined.
Topical agents may be sufficient to produce hemostasis for minor splenic
injuries. Possibilities include Gelfoam (Upjohn, Kalamazoo, Mich.), an ab-
sorbable gelatin sponge, Avitine (Alcon, Humaco, Puerto Rico), a micro-
crystalline collagen, Surgicel, oxidized regenerated cellulose, Collastat (Gen-
esis Biopharmaceutical, Inc., Tenafly, N. J.), native collagen from bovine
tendon, ReClot (Johnson & Johnson), and fibrin glue. The argon beam
coagulator is also useful for superficial capsular injuries. For deeper injuries
involving the parenchyma, horizontal mattress sutures placed over pledgets
are effective for achieving hemostasis. For more severe injuries involving
the segmental vessels or a segment of the spleen, a partial splenectomy may
be required. The segmental vessels can be ligated and divided. The devital-
ized splenic tissue can be resected with stapling instruments.
m
-
m
For injuries that are not localized, splenorrhaphy may still be possible
with commercially available absorbable mesh.
218
.
219
This technique requires
mobilization of the spleen to t ~ e midline with division of the short gastrics.
A 7 x 9 inch sheet of Dexon mesh is cut two thirds down the long axis to
create a "pair of pants.;' The hilar vessels are positioned in the "crotch," and
the "pant legs" are sewn together with a running Vicryl suture. The mesh is
then sewn to itself along the greater curvature of the spleen under mild
tension, and the excess is trimmed.
220
Discrete bleeding points can be rein-
forced with horizontal mattress sutures over omental pledgets. This tech-
nique works well for multiple parenchymal injuries but is not useful in
injury to the hilar vessels.
. Special considerations. There is a frequent association between injuries
to the spleen and injuries to the tail of the pancreas; consequently, the left
upper quadrant is often drained. There has been some concern with an
increased incidence of subphrenic abscess formation associated with the
use of a drain after splenectomy. It appears that the duration of drainage
rather than the mere presence of a drain is the factor related to increased
subphrenic abscess formation.
221
If a drain is used, a closed system (e.g.,
Curr Probl Surg, August 1996 657
TABLE 13. Small bowel injury scale
Grade
II
III
IV
V
Injury description
Contusion or hematoma without devascularization
Partial-thickness, no perforation
Laceration <50% of circumference
Laceration >50% of circumference without transection
Transection of small bowel
Transection of small bowel with segmental tissue
loss
Devascularized segment
ICD-9
863.20
863.20
863.30
863.30
863.30
863.30
AIS,90
2
2
3
3
4
4
From Moore EE, Cogbill TH, Malangoni MA, et al. Organ injury scaling. Surg Slin North Am 1995;75:294
302.
Jackson-Pratt) should be used, and the drain should be removed as early as
possible.
Because of the risk of overwhelming sepsis, all patients who have un-
dergone a splenectomy should receive pneumococcal, hemophilus, and
meningococcal vaccines.
222
We prefer to give the vaccines as .>oon as the
patient is hemodynamically stable. In addition, all patients with less than
30% to 50% of the spleen remaining with an intact vascular supply should
be considered for vaccination. All patients shouV . revaccinated with
pneumococcal vaccine at least every 6 years.
222
The. are no recommen-
dations for readministration of hemophilus or me'1ingococcal vaccines.
Autotransplantation of splenic tissue has not been shown to be effective
and is not recommended.
Small bowel. Injuries to the small bowel from blum trauma are difficult
to diagnose (Table 13). On physical examination these 'injuries may be
obscured by other injures, and routine laboratory studies are nonspecific.
Other diagnostic studies also are insensitive. Diagnostic peritoneal lavage
may be negative for blood. The white blood cell count also may be normal
when the diagnostic peritoneal lavage is performed within 4 hours of in-
jury.223 The finding of hollow viscus injury by CT may be subtle and non-
specific.
m
Intraperitoneal free air may be absent: ather findings such as
thickened bowel wall or thickened mesentery may be subtle. The presence
of peritoneal fluid without evidence of solid organ injury documented by
the CT scan may be the most useful sign of isolated intestinal injury. '
E\posltre. At celiotomy, the small bowel is sequentially inspected begin-
.ling at the ligament of Treitz and continuing throughout its entire length to
the ileocecal valve. The most common sites for small bowel
from blunt trauma are the anti mesenteric border of the proximal jejunum
and distal ileum.
225
During exploration, contamination is controlled by plac-
ing Babcock or Allis clamps on intestinal injuries as they are identified.
Treatment. Serosal injuries to the small bowel are treated by imbrication
658 Curr Probl Surg, August 1996
TABLE 14. Treatment options: small bowel
Grade Treatment options
I, II Single-layer transverse closure with Lembert sutures
I, II, 1.11 Closure with stapling instruments, resection, and stapled anastomosis
IV, V Resection and stapled anastomosis
with interrupted 3-0 silk sutures. Full-thickness injuries can be managed
'j
by repair or resection (Table 14). Repair can be performed either in a single-
or double-layer fashion with equal safety. We prefer single-layer interrupted
3-0 silk suture repair because this requires less time to perform. All repairs
are oriented perpendicular to the axis of the bowel to minimize constriction
of the bowel lumen.
We prefer bowel resection over bowel repair unless the bowel injury is
isolated. To begin the resection, the previously placed Babcock clamps are
lifted from the abdomen. This maneuver delineates the proximal and distal
margins of the resection. A small defect is made at the juncture of the
mesentery and the bO',-I:l. The GIA stapler is used to divide the bowel at the
proximal and distal ITlrgins of the resection.
The Babcock clamps. are lifted once again, defining the limits of the
resection, and the peritoneumof the mesentery is scored with electrocautery.
It is helpful to score t h ~ mesentery in a "V" fashion so that the resection is
parallel to major mesenteric vessels. The resection is t h ~ n completed by
dividing the mesentery between the clamps and ligating vessels with 3-0
ties. We do not use the LDS stapler (US Surgical Co., Norwalk, Conn.)
because in the face of massive visceral edema, hemostasis is not secure.
Once the resection is complete, the bowel is replaced into the abdomen. No
attempt at repair is made until all abdominal injuries are defined.
When the patient is physiologically ready for small bowel anastomosis,
continuity of the gastrointestinal tract can be reestablished with a hand-
sewn anastomosis or with stapling devices. We prefer the GIA to create a
side-to-side (functional end-to-end) anastomosis. The enterotomies can be
closed with a TA-55 (US Surgical Co.). After the anastomosis is com-
pleted, the mesenteric defect is closed to prevent future internal hernias.
Special cOllSideratiollS.Patients with traumatic bowel injury have a 26% inci-
dence of wound infections.
n
Therefore consideration should be given to delayed
primary closure of the skin. These patients frequent!y have other injuries associated
with a protracted hospitalization. Nutritional support can be delivered via the en-
teral route, even if the catheter is proximal to a small bowel anastomosis.
Nutritional support should begin as soon as the patient is no longer receiving
Curr Probl Surg, August 1996 659
TABLE 15. Colon injury scale
Grade Injury description ICD-9 AI5-90
Contusion or hematoma 863.40- 2
Serosal injury, no perforation 863.44
II Laceration <50% of circumference 863.50- 3
863.54
III Laceration >50% of circumference without 863.50- 3
transection 863.54
IV Transection of colon 863.50- 4
863.54
V Transection of colon with segmental tissue loss 863.50- 4
863.54
From Moore EE, Cogbill TH, Malangoni MA, et al. Organ injury scaling. Surg Clin North Am 1995;75:294-
302.
vasoactive medications. It is not necessary to wait for bowel sounds or flatus.
Complications of small bowel injuries are related predominantly to con-
tamination and the magnitude of the injury. All patients receive preoperative
antibiotics and a single postoperative dose for noncolonic gastrointestinal
injuries. Intraabdominal abscesses are uncommon and usually can be man-
aged percutaneously.226 Enterocutaneous fistulas occur rarely after small
bowel injuries, but they may arise even in the absence of an intestinal in-
jury. Management of enterocutaneous fistulas in the patient with trauma is
identical to that in the patient without trauma. Sepsis control is particularly
important. Thirty-three percent of small bowel fistulas will close spontane-
ously with nutrition support.
227
Bailollt. After exsanguinating hemorrhage has been controlled, small
bowel injuries are addressed. If the patient is approaching physiologic ex-
haustion, injured small bO\vel is resected with the GIA stapler. If there are
multiple injury sites, a single resection encompassing less than 50% of the
small bowel is preferred. Blind ends are returned to the peritoneal cavity,
and the patient is left with a "complete bowel obstruction" for several days.
Therefore nasogastric decompression is required.
Colon. Full-thickness colonic injuries in blunt abdominal trauma are
rare (0.6% to 3%), and the diagnosis is seldom made before the opera-
tion.
76
Both diagnostic peritoneal lavage and CT scan have a high inci-
dence of false-negatives. Celiotomy usually is performed for associated
injuries or for the development of peritoneal signs. In patients with pen-
etrating colon injuries, surgical delays of up to 12 hours are not associated
with undue morbidity related to infection (Table 15).228
ExposlIre. At celiotomy, the entire intraabdominal colon should be in-
spected beginning at the ileocecal valve and progressing distally to the
peritoneal reflection. Full-thickness injuries can be controlled with Babcock
660 Curr Probl Surg, August 1996
TABLE 16. Treatment options: colon
Grade Treatment options
I No intervention, invagination with transverse Lembert sutures
II Single-layer transverse closure with Lembert sutures
III Closure as grade II, stapled anastomosis
IV Stapled anastomosis
V Resection and stapled anastomosis or, rarely, colostomy
TABLE 17. Rectum injury scale
Grade
II
III
IV
V
Injury descriptIon
Contusion or hematoma without devascularization
Partial-thickness laceration
Laceration <50% of circumference
Laceration >50% of circumference
Full-thickness laceration with extension to perineum
Devascularized segment
ICD9
863.45
863.45
863.55
863.55
863.55
863.55
AIS90
2
2
3
4
5
5
From Moore EE, Cogbill TH, Malangoni MA, et al. Organ injury scaling. Surg Clin North Am 1995;75:294-
302.
clamps. If a pericolonic hematoma is identified, the colon must be mobi-
lized, the hematoma opened, and the serosal surface carefully inspected to
exclude the presence of an injury.229
Treatment. Military experience with high-velocity missile injuries dic-
tated that colon injuries should be managed with a diverting colostomy or
exteriorization. Until recently, civilian colonic injuries were managed in a
similar fashion. However, because most civilian penetrating colon injuries
are low-velocity injuries, tissue destruction is less severe. Single-layer pri-
mary repair or resection and' primary anastomosis without diversion has
been shown to be the preferred method for most patients (Table 16).76,80.230-242
An increased complication rate is associated with the presence of shock,
transfusion of 6 or more units of packed red blood cells, prolonged con-
tamination, or multiple associated injuries.
235
For patients in extremis con-
tamination and tissue injury can be controlled rapidly with stapling instru-
ments.Anastomosis can be deferred until the patient's physiologic condition
has improved. At the time of reconstruction almost all patients can receive
a primary anastomosis rather than colostomy.
Rectum. Rectal examination should be performed routinely as a part of
any trauma evaluation. Gross blood on the examining finger is a useful
diagnostic finding indicative of a rectal injury (Table 17). Guaiac testing is
not sensitive or specific for rectal injuries.
243
If a rectal injury is suspected,
sigmoidoscopy should be perforined to identify the location and extent of
the rectal injury.
Curr Probl Surg, August 1996 661
TABLE 18. Treatment options: rectum
Grade Treatment options
I, II Primary repair; broad-spectrum antibiotics
III Primary repair; diversion; broad-spectrum antibiotics
IV Primary repair; diversion; distal irrigation and presacral drains; broad-spectrum
antibiotics
V Resection; diversion; distal irrigation and presacral drains; broad-spectrum
antibiotics
Surgical dogma in the management of rectal injuries includes (1)
fecal diversion, (2) closure of the rectal wound, (3) distal irrigation, (4)
presacral drains, and (5) broad-spectrum antibiotics (Table 18). Re-
cently this approach for all rectal injuries has been challengedy-t A
diverting colostomy is necessary in most cases, especially if the rectal
wound cannot be repaired easily. A loop colostomy appears to be as
efficacious as an end colostomy to completely divert the fecal
stream.
245
-
W
Distal irrigation may not be necessary2-t6,W except in pa-
tients with pelvic fractures and high-energy gunshot wounds.
2
-t8 Presacral
drainage is controversial and should be considered in those patients
with a significant posterior rectal laceration and a wide dissection of
the perirectal spacesy6 Daily inspection and repeated surgical
debridement is necessary for an optimal outcome.
2
-t9
Diaphragm. Injuries to the diaphragm are notoriously difficult to diag-
nose outside of the operating room (Table 19). In the case of penetrating
trauma, the path of the knife or missile may suggest a'diaphragmatic in-
jury. In blunt trauma, left-sided diaphragmatic injuries are detectable by
the chest radiograph in one 'third of cases. Right-sided injuries often are
missed altogether. Any trauma celiotomy should include inspection and
palpation of both diaphragms.
Grade I injuries do not require repair (Table 20). If the integrity of the
injured area is in doubt, it may be imbricated with a heavy (0 or 1), braided,
nonabsorbable suture. Grade II and III injuries are managed with an inter-
rupted closure in a single layer using a heavy, braided, nonabsorbable su-
ture. It will facilitate the repair if the sutures are placed and left long, start-
ing from the most accessible end of the laceration. As the repair progresses,
the previously placed stitch may be used to apply upward traction, drawing
the site for the next suture into the field where it may be reached more
easily.
Grade IV and V injuries may require replacement of the lost portion of
the diaphragm with a patch. This is bes't determined after the accessible
ends have been approximated (without tension). At this time, if the tissue
662 Curr Probl Surg, August 1996
TABLE 19. Diaphragm injury scale
Grade Injury description
I Contusion
II Laceration ,;2 cm
III Laceration 2- 10 cm
IV Laceration >10 cm with tissue loss ,;25 cm'
V Laceration with tissue loss >25 cm'
ICD9 AIS-90
862.0 2
862.1 3
862.1 3
862.1 3
862.1 3
Note: Advance one grade for bilateral injuries up to grade III. From Moore EE, Cogbill TH. Malangoni
MA, et al. Organ injury scaling. Surg Clin North Am 1995;75:294-302.
TABLE 20. Treatment options: diaphragm
Grade Treatment options
I Observation
II. III Primary closure
IV Primary closure if possible; PTFE patch if primary repair not possible
V Primary closure if possible; PTFE patch if primary repair not possible
defect is large, a material for replacement of the diaphragm should be se-
lected. Our preference is a polytetrafluoroethylene (PTFE) patch. Although
expensive, this material is nonreactive and does not promote soft tissue
incorporation, an important consideration when one surface of the graft
faces the lung and the other faces the liver.
Bailollt. It is not mandatory that the diaphragm be repaired during the
damage control celiotomy. However, it may be difficult to pack the liver in
the absence of an intact diaph,ragm. One should consider inserting a patch
in grade IV and V injuries to the right hemidiaphragm.
Special consideration. Some lacerations involve the periphery of the dia-
phragm where it inserts onto the ribs. In this situation diaphragmatic con-
tinuity may be reestablished by taking a "bite" of the muscle edge and
passing the needle around the adjacent rib, drawing the suture through to
allow for a complete stitch.
At the conclusion of any diaphragmatic repair, the ipsilateral hemithorax
must be evacuated of air. If there is another reason to do so, a thoracostomy
tube should be inserted. If there is no other reason to place a thoracostomy
tube, then a red rubber catheter may be inserted through a pursestring stitch,
the air aspirated, and the catheter withdrawn as the pursestring is tied. A
chest radiograph should be obtained after the operation.
Stomach. Injuries to the stomach from blunt trauma are rare, occurring
injust 0.9% to 1.7% of cases.250.251 The diagnosis may be difficult to make,
because free intraperitoneal air may be absent and peritoneal findings on
Curr Probl Surg. August 1996 663
physical examination are obscured by associated injuries. Blood from the
nasogastric tube in blunt trauma usually is from facial injuries. However,
in penetrating trauma, blood from the stomach suggests an upper gastrointes-
tinal tract injury. Penetrating injuries to the stomach are more common and
less difficult to diagnose.
The operative intervention for gastric injuries includes complete visual-
ization of both the anterior and posterior gastric walls. This requires open-
ing the lesser sac. The gastric wall usually is well vascularized, but devital-
ized tissue should be debrided. Small wounds can be closed with single
layer of polyglactic acid or polyglactin. Larger wounds may require sta-
pling for both resection and closure. If gastrointestinal continuity is not
reestablished at this time, a nasogastric tube should be positioned in the
proximal gastric remnant. After contamination is controlled, the peritoneal
cavity should be irrigated copiously with warm crystalloid.
The mortality rate for patients with blunt trauma and gastric injuries
ranges up to 66%251; however, the mortality rate is related to the associated
injuries. The most common complication related to gastric injuries is
intraabdominal abscess formation. The risk of abscess formation increases in
the presence of increasing age, gunshot wounds, and multiple transfusions.
252
Empyema is associated with combined gastric and diaphragmatic injuries,
and pleural lavage should be considered for this injury combination.
Organs of the Retroperitoneum
The symptoms of injury to retroperitoneal structures are often delayed in
onset, obscured by other more dramatic injuries, or Conse-
quently, the presence of retroperitoneal injury is often overlooked. The keys
to diagnosis of retroperitoneal injuries include a high index of suspicion
and an organized diagnostic approach. The hallmark of retroperitoneal in-
jury, both on radiography and in the operating room, is the retroperitoneal
hematoma.
60
Ideally, the presence of retroperitoneal hematoma is detected
before the operation. More commonly, however, retroperitoneal hematoma
is discovered at the time of celiotomy.54
Patients with penetrating trauma to the torso who are hemodynamically
unstable or who have peritoneal signs require immediate celiotomy with-
out radiographic assessment of the retroperitoneum. In patients with blunt
trauma, the preoperative diagnosis of a retroperitoneal hematoma may be
suspected by physical examination or the anteroposterior pelvis film and
confirmed by CT scans.
The CT scan is the most effective tool for the preoperative diagnosis of
retroperitoneal injuries. The CT scan defines the size of the retroperitoneal
hematoma associated with pelvic fracture and suggests the need for early
664 Curr Probl Surg, August 1996
FIG. 11. The three zones of the retroperitoneum. Zone I is the central medial zone, containing
the pancreas, duodenum, and major vessels. Zone II contains the kidneys and the retroperitoneal
colon. Zone III contains the major vessels of the pelvis and the redum.
stabilization of the fracture or embolization of pelvic bleeding. The CT
scan also is exquisitely sensitive for diagnosing and grading injuries to the
kidneys.253
Most retroperitoneal hematomas are discovered serendipitously at op-
eration. The keys to the management of these injuries include the patient's
hemodynamic status and the location and mechanism of injury. The crucial
operative decision revolves around whether to open and explore the
hematoma. To make this decision, retroperitoneal hematomas are classi-
fied into three anatomic zones (Fig. 11).60
Zone I is defined as the central medial portion of the retroperitoneum
and includes two visceral organs, the duodenum and pancreas, and the
major abdominal vasculature. Zone II is lateral to zone I and incorporates
the kidney and retroperitoneal portion of the colon and its mesentery. Zone
III includes the entire pelvis; pelvic fractures cause the overwhelming pro-
Curr Probl Surg, August 1996 665
portion of injuries in this area. In clinical practice, large retroperitoneal
hematomas may overlap zones, but the source of the injury is usually ap-
parent.
Zone I extends from the diaphragmatic hiatus of the aorta and esophagus
to the sacral promontory, encompassing the aorta, vena cava, proximal re-
nal vessels, pancreas, and duodenum. In general, all central medial
hematomas require exploration, independent of mechanism of injury (blunt
or penetrating).61 The most common zone I hematomas involve the pan-
creas and duodenum. Inspection of this area may reveal crepitus 01: visible
bile staining under the hematoma. Zone I hematomas resulting from pen-
etrating injuries to the abdominal vascular system are dramatic and associ-
ated with a high mortality rate.
60
Affected patients frequently arrive in the
emergency room moribund and require immediate celiotomy to have
any chance of survival. The keys to the management of this devastating
injury are exposure and control. Feliciano and colleagues
254
have di-
vided the midline retroperitoneal hematoma into inframesocolic and
supramesocolic components. Initial control of the supramesocolic ret-
roperitoneal hemorrhage requires compression or clamping of the su-
prarenal aorta. This may be obtained by one of two methods:
thoracotomy performed in the operating room or opening the gastric he-
patic ligament. Operating room thoracotomy64 is primarily used in pa-
tients with hemorrhage that remains uncontrolled despite an aggressive
attempt at resuscitation. Alternatively, control of the suprarenal aorta may
be obtained by dividing the gastric hepatic ligament ~ n d retracting the
esophagus and stomach to the left. Then the muscle fibers of the crura are
split below the hiatus, expos!ng the supraceliac aorta.
Zone II is located l.ateral to the psoas muscle, above the iliac crest, and
below the diaphragm. A zone II retroperitoneal hematoma indicates a po-
tential injury to the kidney255 or colon.
256
A direct blow to the flank may
lead to renal contusion, laceration, avulsion, or rupture. These injuries are
often associated with hematuria (greater than 100 red blood cellslhpf) and
are best evaluated before the operation by CT scan. The CT scan has en-
hanced our ability to define the anatomy of these lesions accurately and has
decreased the nephrectomy rate. Approximately 95% of patients with blunt
perirenal hematomas can be treated without operation.
257
Isolated blunt
injury to the colon is rare
76
; however, pericolic hematoma must be explored
to ensure that the colonic wall is intact and that there is no injury, to the
mesocolon.
Zone III or pelvic hematomas are located below the bladder anteriorly,
the sacral promontory posteriorly, and the iliac crest laterally. Zone III
hematomas are the most common retroperitoneal injuries associated with
666 Curr Probl Surg. August 1996
TABLE 21. Duodenum injury scale
Grade Injury description ICD-9 AiS90
Hematoma involving single portion of duodenum or 863.21 2
serosal injury, no perforation 863.21 3
II Hematoma involving more than one portion 863.21 2
Disruption <50% circumference 863.31 4
III Disruption 50% 75% circumference of 02 863.31 4
Disruption 50% - 100% circumference of 01, 03. D4
IV Disruption >75% circumference 02 863.31 5
Involving ampulla or distal common bile duct
V Massive disruption of duodenopancreatic complex 863.31 5
Devascularization of duodenum
01, First portion of duodenum; 02, second portion of duodenum; 03, third portion of duodenum; 04,
fourth portion of duodenum. From Moore EE. Cogbill TH, Malangoni MA. et al. Organ injury scaling. Surg
Clin North Am 1995;75:294-302.
blunt trauma. In patients with blunt trauma, the hematoma is not explored.
Retroperitoneal hematomas caused by penetrating injury often expand rap-
idly as a result of iliac vessel damage. Control of the infrarenal abdominal
aorta and inferior vena cava proximally and iliac vessels distally should be
obtained before the hematoma is opened and the injury is repaired.
Duodenum. General considerations. Three mechanisms account for
duodenal injury: crushing, bursting, and shearing forces.258-26o Deaths asso-
ciated with duodenal trauma are generally due to hemorrhagic shock from
major vascular or hepatic injury.213.261 Injuries involving t ~ e second portion
of the duodenum, the distal common bile duct, or the ampulla are associ-
ated with increased rates of mortality and morbidity (Table 21). Late deaths
in the setting of duodenal injury result from duodenal dehiscence and un-
controlled sepsis.
213
THere is a high incidence of associated injury accom-
panying pancreaticoduodenal injuries.
262
Preoperative diagnosis. The preoperative diagnosis of duodenal in-
jury is challenging. Plain radiographs of the abdomen may provide
clues to the presence of duodenal injury. Findings include obliteration
of the psoas shadow, the presence of retroperitoneal air, or air in the
perinephric or subphrenic space.
263
Contrast gastroduodenography is
helpful, although the false-negative rate may be high.263.264 Plain radio-
graphs and contrast enhanced films may miss as many as 60% to 80%
of cases of duodenal injury.264.265 CT is a useful diagnostic tool for
revealing duodenal injuries. The right anterior pararenal space should
be examined closely for extravasated contrast material or extraluminal
gas.
266
Intraperitoneal fluid, thickening of the duodenum, and fluid in
the right perirenal space are nonspecific and do not distinguish patients
Curr Probl Surg, August 1996 667
TABLE 22. Treatment options: duodenum
Grade Injury description
Hematoma involving single portion of duodenum
Partial-thickness laceration, no perforation
II Hematoma involving more than one portion
Disruption involving <50% circumference
III Disruption involving 50%-75% circumference of D2
Disruption involving 500/0-100% circumference of D1,
D3, or D4
IV Disruption>75% circumference of D2 involving
ampulla or distal common bile duct
V Massive disruption of duodenopancreatic complex
Devascularization of duodenum
Treatment
Observation
Closure
Observation
Closure; drainage
Closure; drainage;
pyloric exclusion
Closure; drainage;
pyloric exclusion;
pancreatoduodenectomy
Pancreatoduodenectomy
with duodenal perforation from those with duodenal or periduodenal
hematoma.
Intraoperative diagnosis. In the vast majority of patients, the diagnosis
of duodenal injury is made during the operation. Surgeons should suspect
duodenal injury when they find blood, air, or bile in the periduodenal tis-
sues. The duodenum should be Kocherized if there is injury to periduodenal
structures including the vena cava, gallbladder, pancreas, or kidney. The
Kocher maneuver begins with incision of the peritoneumlateral to the duode-
num. Then the duodenum and the pancreatic head are mobilized toward the
aorta. Mobilization of the hepatic flexure of the colon improves exposure.
The retroperitoneum is incised along the lateral border of the colon, and
the colon is then bluntly mobilized toward the midline. If necessary, the
ligament of Treitz can be divided so that the third and fourth portions of the
duodenum can be examined thoroughly. Having obtained adequate expo-
sure, injuries can be identified, graded, and prioritized for repair.
Management by grade. Four factors associated with duodenal injury in-
crease morbidity: (1) injury to the common bile duct or proximal duode-
num, (2) injury to greater than 75% of the circumference of the duodenal
wall, (3) delay to repair of greater than 24 hours, and (4) mechanism of
injury of either high-velocity gunshot wound or blunt trauma. The fistula
rate was 10% among patients with high-risk criteria but only 2% among
patients without these criteria.
2M
Consequently, the surgeon's first task is
to determine the location of the duodenal injuries and to estimate the de-
gree of wall surface area involved (Table 22). '
Grades I, ll, and lll. Duodenal hematomas without full- thickness injury
do not require surgical repair. Patients are maintained on nasogastric suc-
tion, parenteral fluid replacement, and nutrition as necessary. The hematoma
668 Curr Probl Surg, August 1996
resolves in 10 to 21 days. Duodenal lacerations involving the first, third,
and fourth portions can be managed with debridement and closure. Lacera-
tions involving the second portion of the duodenum are also often ame-
nable to simple repair, as long as less than 75% of the circumference of the
bowel wall is injured and there are no concomitant injuries to the common
bile duct, ampulla, or pancreatic head. In a review of 164 duodenal injuries
reported from eight referral trauma centers, 67% of grade II and III injuries
were amenable to simple closure.
213
Intraabdominal abscess was a compli-
cation in approximately 12% of patients and was not related to the extent
of the procedure performed. The use of a serosal patch of jejunum to but-
tress or complete the duodenal repair has been advocated but has not been
shown to be superior to simple closure.
267
Grade IV and V. Cases of extensive loss of duodenal wall in the second
portion present a special problem in management, because this is an area in
which extensive mobilization and resection are neither easy nor safe. One
option for those duodenal injuries that involve loss of substantial portions
of the wall is a duodenojejunostomy, with a Roux-en-Y limb used to mini-
mize reflux.
268
Grade V injuries require pancreatoduodenectomy.
In summary, injuries to the first, third, and fourth portions of the duode-
num are treated with simple repair or segmental resection with primary
end-to-end anastomosis. We reserve pyloric exclusion for delayed repairs,
significant tissue destruction, or involvement of the common bile duct.
Resection is not an option at the level of the second portion of the duode-
num because of the shared blood supply between the duodenum and the
pancreatic head and the presence of the ampulla of Vater. Injuries in this
area require use of a retroc.olic duodenojejunostomy with a 40 cm
defunctionalized Roux-en-Y jejunal limb. Pancreaticoduodenectomy is re-
served for cases that involve massive tissue destruction of the
pancreaticoduodenal complex or the distal common bile duct.
For the patient in extremis the ends of the duodenum can be left stapled,
provided there is some conduit for the removal of bile, pancreatic juice,
and duodenal secretions. This can be achieved by placing a nasogastric
tube through the pylorus.
Special considerations. Historically, decompression of the duodenum is
mentioned as an adjunct to the healing of duodenal injuries. The reported
results have been mixed. Stone and Fabian
269
have advocated the triple-
tube system for management of duodenal injuries and found a reduction in
duodenal complications. Other investigators, however, have not found this
technique to be advantageous.264.2690271 The results of a recent multicenter
review indicate that duodenal decompression probably does not alter the
rate of duodenal wound complications,213 fistula formation, duodenal de-
Curr Probl surg. August 1996 669
hiscence,213 or duodenal suture line complications.
213
2
6.t.272.273
Diversion of flow around the duodenum has been proposed to minimize
suture line complications. This has generally taken two forms:
diverticulization and pyloric exclusion. Berne
2733
proposed the concept of
duodenal diverticulization to minimize flow across a duodenal repair, pro-
mote healing, and prevent a lateral duodenal fistula. The procedure he de-
scribed consisted of antrectomy, truncal vagotomy, and gastrojejunostomy.
We find this requires more tissue sacrifice than patients are able to tolerate,
and lesser procedures will often suffice. We reserve a formal diverticular-
ization for severe distal gastric injuries.
Pyloric exclusion is the other technique used to divert duodenal flow.
This concept is generally attributed to Vaughn and colleagues,m although
Berg
275
actually first described pyloric exclusion with gastrojejunostomy
in 1907 for the management of lateral duodenal fistulae. The classic py-
loric exclusion is performed by closure of the pylorus through a gastrotomy,
with reestablishment of gastrointestinal continuity via a gastrojejunostomy.
The important technical point is to be certain that no antrum is included in
the closure, lest ulcerogenic secretions be stimulated. Although pyloric ex-
clusion does not prevent duodenal suture line complications, it may sim-
plify the management of such complications with percutaneous drains rather
than reoperation.
The need for vagotomy in the setting of pyloric exclusion with
gastrojejunostomy has been suggested. In the series by Vaughn and c o l ~
leagues,m three marginal ulcers developed in 75 patients undergoing py-
loric exclusion. One of these patients had a history of peptic ulcer disease
and was treated medically; the other two had gastric hypersecretion and
required surgical treatment. Vaughn and colleagues did note that their per-
cent incidence of postoperative marginal ulceration was lower than the re-
ported ulcer rate associated with vagotomy and pyloroplasty or vagotomy
and jejunostomy used in the treatment of peptic ulcer disease. However,
Feliciano and colleagues
276
reported 180 patients who had pyloric exclu-
sion and gastrojejunostomy, with no identified marginal ulcers. These sur-
geons did not routinely treat their patients with H
2
-receptor antagonists,
nor did they perform vagotomy. In the series of 128 patients by Martin and
colleagues,277 vagotomy was not used as an adjunct to the pyloric exclu-
sion. Forty-two patients underwent postoperative gastrointestinal tract evalu-
ation, and four patients were found to have marginal ulceration. Thus it
seems unnecessary to add the morbidity associated with vagotomy 'to pre-
vent marginal ulceration, which can generally be managed medically.
One concern when pyloric exclusion is used is that the pylorus remain
closed long enough to allow healing of the duodenal repair. The pyloric
670 Curr Probl Surg, August 1996
TABLE 23. Pancreas injury grading
Grade Injury description ICD9 AIS90
Minor contusion without duct injury
Superficial laceration without duct injury
II Major contusion without duct injury or tissue loss
863.81-
863.84
863.81
863.84
2
2
4
3
3 863.92-
863.94
863.91
Major laceration without duct injury or tissue loss
Distal transection or parenchymal injury with duct
parenchymal injury with duct injury
Proximal transection or parenchymal injury
involving ampulla
V Massive disruption of pancreatic head 863.91 5
IV
III
From Moore EE. Cogbill TH. Malangoni MA. et aJ. Organ injury scaling. Surg elin North Am 1995;75:294-
302.
closure is not pennanent, regardless of the type of suture material chosen
for closure. Pyloric exclusions perfonned with absorbable sutures open up
sooner than those with nonabsorbable sutures, but even stapled closures
will eventually open.
278
Martin and colleagues
217
reported 42 patients with
pyloric exclusion and gastrojejunostomy who had upper gastrointestinal
contrast studies perfonned 21 days or more after operation; 94% were found
to have a patent pylorus. DeSantis and colleagues,279 in a dog model, deter-
mined time to pyloric patency for the different suture materials. At 6 weeks
one out of four polypropylene closures was still secure, whereas pyloric
patency had been reestablished in all of the dogs in the polyglycolic acid
and polydiaxinone groups.
Nutritional support is critical in these patients. The enteral route is pref-
erable to parenteral nutrition,280 and the needle catheter jejunostomy has
been used with success in critically injuredpatients. A note of caution has
been sounded regarding-the use of needle catheter jejunostomy in patients
with massive edema after they undergo secondary resuscitation or in pa-
tients with injuries of the pancreaticoduodenal complex or portal vein. A
high rate of leakage was noted in one retrospective review. 140 These authors
suggested intraoperative passage of a feeding tube, with positioning at the
desired level by the surgeons at the time of operation. This is our current
practice if the patient is believed to be at risk for leakage around the needle
catheter jejunostomy site.
Pancreas. Intraoperative diagnosis. The pancreas should be explored in
all patients with peripancreatic hematoma (Table 23). Peripancreatic fluid
without hematoma, particularly in a patient with edematous tissues, does
not by itself demand retroperitoneal exploration.
281
The anterior surface of
the pancreatic head should be visualized within the duodenal C-loop. In-
spection of the posterior aspect of the head of the pancreas requires a Kocher
Curr Probl Surg. August 1996 671
maneuver, as described previously. The anterior aspect of the body of the
pancreas is exposed by entering the lesser sac through the gastrocolic omen-
tum below the gastroepiploic vessels. The stomach is reflected
and adhesions between the posterior surface of the stomach and the pancre-
atic body are divided. The tail of the pancreas is in close association with
the splenic hilum, and care must be exercised when dissecting in this area
because the spleen or its vascular supply can be damaged.
Intraoperative pancreatography is a useful adjunct to diagnose occult duc-
tal injuries in the head of the pancreas. This technique requires duodenotomy,
cannulation of the ampulla of Vater, and gentle injection of a water;soluble
contrast material. Successful visualization of the duct has been reported in
90% of patients in one series.
282
Another series reported a reduction of pan-
creatic complications from 55% without pancreatography to 15% when
pancreatography was used to identify major ductal injuries. Some authors
argue against the use of intraoperative pancreatography because of the risk of
duodenal fistula.
283
On the other hand, two series have reported the use of
intraoperative pancreatograms with no such Intraoperative
endoscopic retrograde pancreatography is time- consuming and requires skills
and equipment not immediately available during a trauma celiotomy.
Diagnostic studies. Because of its retroperitoneal location, pancreatic
injury can be difficult to diagnose with peritoneal lavage. In the absence of
clinical deterioration, hyperamylasemia alone does not constitute an indi-
cation for operation.281.283 CT has the advantage of allowing visualization
of the retroperitoneum. Signs suggestive of pancreatic injury include pan-
creatic swelling, fluid in the lesser sac, fluid between'the pancreas and
splenic vein,285 and pancreatic laceration. The accuracy of CT scan diagno-
sis in pancreatic injury is' variable.283.286.287 Endoscopic retrograde
cholangiopancreatography is primarily useful for diagnosis of late pancre-
atic complications. Its successful use in the acute stages has been reported
in stable patients.
288
Endoscopic retrograde cholangiopancreatography has
no role during a damage control celiotomy.
Treatment by grade. The treatment strategy for pancreatic injuries in-
cludes a determination of the presence of peripancreatic hematoma and
ductal injury (Table 24). Occasionally splenectomy is necessary for ad-
equate exposure and management. The small risk of postsplenectomy sepsis
is accepted. In the more stable patient, however, distal pancreatectomy with
splenic preservation can be accomplished safely.289
Simple grade I and II contusions of the pancreas are best managed with
placement of a soft-closed suction drain.281.282 For grade III injuries the
distal end of the pancreas should be amputated. The duct, if visible, should
be oversewn with fine nonabsorbable suture, and the end of the pancreas
672 Curr Probl Surg, August 1996
TABLE 24. Treatment options: pancreas
Grade Injury description
Minor contusion without duct injury;
Superficial laceration without duct injury
II Major contusion without duct injury or tissue loss
Major laceration without duct injury or tissue loss
III Distal transection or parenchymal injury with
duct injury
IV Proximal transection or parenchymal injury
involving ampulla
V Massive disruption
Treatment
Observation
Drainage
Drainage
Drainage
Pancreatoduodenectomy if
ampulla destroyed; closure
of proximal duct; qistal
pancreatojejunostomy
Pancreatoduodenectomy vs
excision of pancreatic head
should be closed with a stapler or with monofilament running suture. Cur-
rent trends suggest replacement of pancreaticojejunostomy with pancreatic
resection. Pancreatic resection improves morbidity, reduces fistula and ab-
scess formation, and may decrease late septic deaths.
i82
For grade IV and V injuries in which resection of more than 80% of the
pancreas is required, a Roux-en-Y pancreaticojejunostomy wiII reduce the
incidence ofendocrine and exocrine pancreatic insufficiency.283 TheWhipple
procediIre is reserved for injuries that involve the ampulla, ductal injury in
the pancreatic head with associated common duct and duodenal injuries, or
massive devascularization of the duodenum. These unusual situations oc-
cur in 2% to 3% of all pancreatic injuries.
276
Mortality rates for
pancreatoduodenectomy in patients with trauma is 30% to 40%.290.291 How-
ever, under appropriate circumstances pancreaticoduodenectomy can be
performed safely in patients with trauma.
292
293
The Whipple operation is
inappropriate in a patient who is unstable; these patients should be consid-
ered for a bailout procedure with delayed establishment ofpancreaticobiliary
drainage. Total pancreatectomy generally is unnecessary except in the case
of extreme disruption of the entire gland. This procedure is associated with
complex endocrine and exocrine complications.
29
.t
Bailollt. Complex pancreaticoenteric reconstructions are never appropriate
in unstable patients. Distal resection of the injured pancreas usually can be
carried out rapidly with a stapler. In extreme situations, especially if grade IV
or V injuries are present in unstable patients, placement of drains and packing
may be required to allow restitution of physiologic reserve. The patient can be
returned to the operating roomfor definitive reconstruction. This type of staged
procedure has been described with acceptable results.
295
Curr Probl Surg, August 1996 673
TABLE 25. Kidney injury grading
Grade Injury description ICD9 AIS90
2
2
2
2
4
4
3
866.01
866.11
866.01
866.11
866.02
866.12
866.02
Microscopic or gross hematuria, urologic studies normal
Subcapsular hematoma, nonexpanding without
parenchymal laceration
Nonexpanding perirenal hematoma confined to
renal retroperitoneum
Laceration of <1 cm parenchymal depth of renal
cortex without urinary extravasation
Laceration of >1 cm parenchymal depth of renal
cortex without collecting system rupture or
urinary extravasation
Parenchymal laceration extending through the
renal cortex, medulla, and collecting system
Main renal artery or vein injury with contained
hemorrhage
Completely shattered kidney 866.03 5
Avulsion of renal hilum that devascularizes kidney 866.13
IV
II
V
III
From Moore EE, Cogbill TH, Malangoni MA, et al. Organ injury scaling. Surg Clin North Am 1995;75:294
302.
Special considerations. Combined pancreaticoduodenal injuries are man-
aged based on the criteria described for management of trauma to the indi-
vidual organs. Pancreatoduodenectomy is avoided, if possible. Pyloric ex-
clusion is an important component of the management of these injuries.
Octreotide acetate has been shown to be beneficial in a randomized, con-
trolled, prospective study of patients undergoing elective pancreatic resec-
tions.
296
Nutritional support is essential. Although contrOersy has persisted
regarding the intravenous versus enteral route, feeding jejunostomy has
been found to be safe in the setting of pancreatic injuries,m and enteral
support is associated .with fewer septic complications than total parenteral
nutrition.
280
Kidney. The presence of hematuria is neither sensitive nor specific
for renal injury.297 Although intravenous urography is frequently rec-
ommended as the imaging study of choice, CT scanning is now the
best diagnostic study for renal trauma.
298
Operative indications for re-
nal exploration include large perinephric hematoma,299 pulsatile
hematoma, or radiographic study suggestive of a major pedicle or pa-
renchymal injury (Table 25).300
Exposure of the right kidney is obtained by reflecting the duodenum and
ascending colon medially, whereas access to the left kidney requires me-
dial reflection of the left colon. Gerota's fascia is incised laterally, and the
plane posterior to the kidney is developed (Table 26). Vascular injuries at the
hilum require vascular repair or nephrectomy. Collecting system injuries at or
674 Curr Probl Surg, August 1996
TABLE 26. Treatment options: kidney
Grade Injury description
Microscopic or gross hematurio, urologic studies normal
Subcapsular hematoma, nonexpanding
II Nonexpanding perirenal hematoma confined to renal
retroperitoneum
laceration of <1 cm parenchymal depth of renal cortex
III Laceration> 1 cm parenchymal depth of renal cortex
IV Parenchymal laceration extending through the renal cortex,
medulla, and collecting system
Main renal artery or vein injury with contained hemorrhage
V Completely shattered kidney
Avulsion of renal hilum (devascularization)
Treatment
Observation
Observation
Observation;
perinephric drain
Debridement;
closure; perinephric
drain; omental patch
Repair collecting
system;
debridement;
cortical closure;
perinephric drain;
omental patch
repair; nephrectomy
Nephrectomy
Nephrectomy vs
repair
near the hilum will likewise require repair with fine absorbable suture. Grade
I injuries and nonbleeding parenchymal lacerations may be managed with
observation or simple drainage.
297
Direct renorrhaphy with capsular approxi-
mation is required for grade II and III injuries. The defect often can be closed
primarily. This procedure is facilitated by debriding injured tissue in aV-shaped
beveled fashion, with the apex of the V placed within the depth of the lacera-
tion. An omental pedicle or free-fat graft may be placed into the laceration.
Pledgets of Dexon mesh may be used when suturing the kidney to prevent
tearing of the parenchyma. Mesh renorrhaphy is a technique gaining in popu-
larity?99 This technique involves making a kidney-sized envelope out of a sheet
of Dexon mesh and tightly wrapping the kidney within the envelope, suturing
the free edge so as to provide pressure.
Bailollt. For patients ill extremis, nephrectomy may be a life-saving ma-
neuver. Before nephrectomy is performed, it is important to ascertain
whether the contralateral kidney is functional. Although it may be neces-
sary to render a patient anephric to preserve life, one would prefer to do so
with foreknowledge.
Special considerations. There is much debate about whether it is neces-
sary to gain vascular control at the hilum before exploring an injured kid-
ney. There are those who believe that this maneuver reduces the nephrectomy
rate
301
and those who argue that it does no1.
299
Curr Probl Surg, August 1996 675
TABLE 27. Ureter injury grading
Grade Injury description ICD9 AlSo90
Contusion or hematoma without devascularization 867.2 2
867.3
II <50% transection 867.2 2
867.3
III >50% transection 867.2 3
867.3
IV Complete transection 867.2 3
with <2 cm devascularization 867.3
V Avulsion with >2 em devascularization 867.2 3
867.3
From Moore EE, Cogbill TH, Malangoni MA, et al. Organ injury scaling. Surg Clin North Am 1995;75:294
302.
Intravenous pyelography is not necessary before exploration for pen-
etrating trauma; this test may waste valuable time and can be performed in
the operating room (dose: 30 gm of elemental iodine, wait 5 to 7 minutes).
The only purpose of the "one-shot intravenous pylography" is to ascertain
the status of the other kidney. We routinely drain renal injuries with soft
closed-suction drains. Nephrostomy tubes are rarely indicated in the acute
setting.
302
Ureter. Treatment by grade. Ureteral injury (Table 27) is relatively un-
common. In penetrating trauma the incidence ranges from 2.3% to 17%.303.306
In blunt trauma this injury is exceedingly unusual,37 The diagnosis is chal-
lenging. Urinalysis will fail to show either gross or microscopic hematuria
in 23% to 45% of cases of ureteral injury.257,299.305,307,308 Intravenous
pylography abnormalities indicating ureteral injury include extravasation
of contrast, occlusion 'of a ureter, or deviation of the ureter. The IVP will be
nondiagnostic in 70% to 75% of ureteral injuries.307.309
Operative exposure of the ureter is facilitated by locating the ureter as it
crosses over the iliac bifurcation. The ureter can then be traced proximally
and distally. Care should be taken to avoid devascularizing the ureter by
excessive skeletonization. Grade I injuries may be observed (Table 28).
However, contusions can progress to full-thickness injuries
31O
,3Il; conse-
quently, we place a soft closed-suction drain adjacent to a contused ureter.
Grade II and III injuries are managed by simple closure. The injured
ends are debrided back to viable tissue, and closure is performed with fine
(3-0 or 4-0) absorbable suture material over a double-j stent. Grade IV
injuries are debrided back to healthy tissue. Each end is spatulated in a
complimentary fashion, and closure is performed in a single layer over a
double-j stent. Caudal grade V injuries, if low, can be managed with
676 Curr Probl Surg, August 1996
TABLE 28. Treatment options: ureter
Grade
I
II
III
IV
V
Injury description
Hematoma without devascularization
<50% transection
>50% transection
Complete transection with <2 cm devascularization
Avulsion with >2 cm devascularization
Treatment
Observation drainage
Repair over stent; drainage
Repair over stent; drainage
Debride devitalized ends;
repair over stent; drainage
Ureteroneocystostomy
psoas hitch or Boari flap for
lower one third; trans-
ureterostomy for upper two
thirds or if uretero-
neocystostomy produces
tension
ureteroneocystostomy with or without a psoas hitch, depending on the level
of the injury. Proximal injuries may require autotransplantation,
ureteropyeloplasty, or nephrectomy.307.312
Bailout. Even during an abbreviated celiotomy, ureteral continuity should
be reestablished. When ureteral injuries are left unrepaired, there is a high
incidence of sepsis and loss of renal function.307.309.3IJ If it appears that a
complex or lengthy urologic repair will be needed in an unstable patient,
nephrectomy is an option. This situation is most common in patients with
ureteropelvic disruption.
Special considerations. Urologic injuries should be drained routinely.
We prefer a soft closed-suction system. The use of intravenous indigo
Carmen dye (5 to 10 mt) is a helpful adjunct for diagnosis of occult ureteral
injuries.
Bladder. The continuum of bladder injuries extends from contusion to
rupture (Table 29). Intraperitoneal rupture is thought to be due to an abrupt
rise in pressure within the bladder at the time of injury, producing a burst-
ing mechanism.
313
Approximately 75% of extraperitoneal ruptures result
from direct laceration by a bony fragment from a pelvic fracture.
313
,314 Com-
bined intraperitoneal and extraperitoneal injuries do occur but are uncom-
mon.
315
The diagnosis of bladder rupture is difficult. Gross hematuria should
prompt further evaluation. Microscopic hematuria should also raise the
level of suspicion, particularly in the setting of pelvic fracture. If the stan-
dard of greater than 50 red blood cells/hpf is used to mandate
cystography, the chances of missing a serious urologic injury is very
IOW.
316
Unfortunately, CT scanning is an insensitive test for bladder
injury and may fail to detect up to one third of these injuries.316.317 Our
Curr Prabl Surg, August 1996 677
TABLE 29. Bladder injury grading
Grade Injury description ICD-9 AIS90
Contusion, intramural hematoma 867.0 2
Partialthickness laceration 867.1
II Extraperitoneal bladder wall laceration <2 cm 867.0 4
867.1
III Extraperitoneal >2 cm or 867.0 4
intraperitoneal <2 cm bladder wall laceration 867.1
IV Intraperitoneal bladder wall laceration >2 cm 867.0 4
867.1
V Intraperitoneal or extraperitoneal bladder wall 867.0 4
laceration extending into the bladder neck or 867.1
ureteral wall orifice
From Moore EE, Cogbill TH, Malargoni MA, et al. Organ injury scaling. Surg Clin North Am 1995;75:294-
302.
TABLE 30. Treatment options: bladder
Grade Injury description
Contusion, intramural hematoma
Partial-thickness laceration
II Extraperitoneal walllaeeration <2 em
III Extraperitoneal walllaeeration >2 cm
Intraperitoneal wall laceration <2 cm
IV Intraperitoneal walllaeeration >2 cm
V Intraperitoneal or extraperitoneal wall
laceration extending to the bladder neck
or ureteral orifice
Treatment
Observation
Closure; Foley catheter drainage
Closure; Foley catheter drainage
Closure; Foley catheter drainage
Closure; Foley catheter drainage
Closure; Foley catheter drainage;
ureteral repair stent
experience is that perivesical hematoma demonstrated by CT scan
should prompt cystography.
The gold standard for the diagnosis of bladder mpture is two-shot retro-
grade contrast cystography. This study, to be accurate, must fulfill two key
technical points. First, at least 300 ml of contrast must be used to distend
the bladder appropriately. Second, the study consists of two shots: a maxi-
mal distension shot and a postdrainage shot. It is important that both of
these criteria be met. One series found a 4.3% incidence of false-negative
studies that did not meet both of these criteria.
318
Treatment by grade. The AAST grading system, although useful fqr de-
scribing injuries, does not lend itself to a simple management approach
(Table 30). Instead, we prefer to first classify the injury according to whether
it is intraperitoneal or extraperitoneal. Intraperitoneal mptures generally
require operation. The bladder is closed in two layers, with a mnning 3-0
678 Curr Probl Surg, August 1996
absorbable suture incorporating all layers, followed by a second layer of
interrupted 3-0 absorbable sutures for the seromuscular layer. Partial-thick-
ness lacerations may be closed with seromuscular sutures.
Extraperitoneal injuries, on the other hand, may be managed with simple
catheter drainage alone, if there is no other reason to operate.
3I9
Suprapubic
catheter drainage of the bladder is not necessary unless clot formation is
excessive and impairs drainage from the Foley catheter. The key in suc-
cessful nonoperative management of extraperitoneal bladder injuries is
adequate bladder drainage by either the Foley catheter or suprapubic tube.
Bailout. Repair of the ruptured b.Iadder is not absolutely mandatory dur-
ing the course of celiotomy for the patient in extremis. As noted, an impor-
tant decision point is whether the rupture is intraperitoneal or extraperitoneal.
An intraperitoneal rupture is usually technically easy to manage and does
not require much repair time. Extraperitoneal ruptures can be left undis-
turbed, particularly if there is an associated pelvic fracture and the injury is
recent 24 hours).
Special considerations. Because bladder injuries are encountered so fre-
quently in association with pelvic fractures, a common point of confusion
is how much bladder evaluation a patient with pelvic fracture requires.
Fnictures of the symphysis pubis or pubic rami are associated most com-
monly with bladder rupture, and 98% of these patients had gross
hematuria.
320
Vascular
.
Although the AAST system is useful for guiding surgical management in
most abdominal trauma situations, it is not well suited for use in making
management decisions in patients with abdominal vascular trauma (Table
31). Our management approach to abdominal vascular trauma is dictated
by anatomy. Zone I retroperitoneal hematomas suggest aortic or caval lac-
erations, and these injuries should be explored. A leftward extension of the
hematoma would indicate that the search begin with exposure of the aorta,
whereas a rightward extension would raise concern about the vena cava. If
after adequate inspection neither of these vessels is found to have been
damaged, visceral vascular injuries should be sought.
Exposure. When confronted with major abdominal vascular injuries, ad-
equate exposure is essential. These injuries inspire a degree of respect in
even the most seasoned trauma surgeon. One must resist the temptation to
explore a hematoma before adequate exposure has been obtained.
Access to the abdominal aorta is gained by making an incision in the
posterior parietal peritoneum lateral to the left colon (along the white line
of Toldt). If needed, this incision may be carried superiorly, dividing the
Curr Probl Surg, August 1996 679
TABLE 31. Vascular injury grading
Grade Injury description ICD-9 AIS-90
Nonnamed superior mesenteric artery 902.20/.39 NS
or superior mesenteric vein branches
Nonnamed inferior mesenteric artery 902.27/.32 NS
or inferior mesenteric vein branches
Phrenic artery/vein 902.89 NS
Lumbar artery/vein 902.89 NS
Gonadal artery/vein 902.89 NS
Ovarian artery/vein 902.81/.82 NS
Other nonnamed small arterial or venous 902.90 NS
structures requiring ligation
II Right, left, or common hepatic artery 902.22 3
Splenic artery/vein 902.23 3
Right or left gastric arteries 902.21 3
Gastroduod,enal artery 902.24 3
Inferior mesenteric artery, trunk or inferior 902.27/.32 3
mesenteric vein, trunk
Primary named branches of mesenteric artery (e.g., 902.26/.31 3
ileocolic artery) or mesenteric vein
Other named abdominal vessels requiring 902.89 3
ligation/repair
III Superior mesenteric vein, trunk 902.31 3
Renal artery/vein 902.41/.42 3
Iliac artery/vein 902.53/.54 3
Hypogastric artery/vein 902.51/.52 3
Vena cava, infrarenal 902.10 3
IV Superior mesenteric artery, trunk 902.25 3
Celiac axis proper 902.24
Vena cava, suprarenal and infrahepatic 902.10
Aorta, infrarenal 902'.00 4
Portal vein 902.33 3
Extraparenchymal hepatic vein 902.11 3/5
Vena cava, retrohepatic or suprahepatic 902.19 5
Aorta, suprarenai, subdiaphragmatic 902.00 4
Note: If vascular injury within 2 em of specific organ, refer to that organ's injury scale.
Increase one grade for multiple grade III or IV injuries involving >50% vessel circumfer-
ence. Downgrade one grade if <25% vessel circumference laceration for grades IV or V.
From Moore EE, Cogbill TH, Malangoni MA, et al. Organ injury scaling. Surg Clin North Am 1995;75:294-
302.
splenorenal and splenophrenic ligaments. The small bowel is retracted
medially, and the colon is reflected rightward. The left kidney may be left
in place or reflected medially if needed for exposure, as may be the pan-
creas, stomach, distal esophagus, and spleen. The ligament of Treitz may
be divided. Control of the suprarenal aorta also may be obtained via the
lesser sac through the lesser omentum, retracting the esophagus and stom-
ach leftward. Proximal control may be achieved with a vascular clamp, an
aortic occluder, or a Richardson retractor placed directly on the aorta through
680 Curr Probl Surg, August 1996
the gastrohepatic ligament with pressure directed posteriorly. In some cases,
if the injury is high enough, proximal control can be achieved above the
diaphragm via radial phrenotomy or left thoracotomy. This approach has
the additional advantage of avoiding the dense network of nerve and lym-
phatic tissue that overlies the aorta at the level of the celiac axis.
The possibility of injury to the inferior vena cava should be considered
in any patient who has a zone I retroperitoneal hematoma, particularly on
the right side. Exposure of the infrahepatic inferior vena cava is best ob-
tained by making an incision in the posterior parietal peritoneum lateral to
the right colon (along the white line of Toldt) and the duodenum. These
organs are then reflected medially to the level of the aorta. The first assis-
tant must be ready to occlude the cava manually when the injury is discov-
ered; this is best accomplished initially with one or two crumpled celiotomy
pads applied firmly and directly over the injury. The anesthesia personnel
must be informed when the cava is occluded. At this point the operative
field will most likely consist of the right colon, duodenum, and small bowel
reflected to the left, a large amount of clot within the areolar tissues of the
retroperitoneum, and a hand holding celiotomy pad directly atop the cava.
The vena cava itself is then meticulously exposed. This is accomplished by
starting at either end of the field and working in tum toward the celiotomy
pads, gradually exposing the inferior vena cava and clearing off overlying
clot and tissue. Keeping the dissection on the absolute anterior surface of
the cava is the best way to avoid injuring tributaries, which generally enter
laterally (with the exception of the right gonadal vein). .
Access to the iliac veins is particularly difficult. One helpful technique is
to divide the internal iliac artery at the level of the bifurcation of the inter-
nal and external i1iacs from the common iliac artery. The internal iliac
artery is then reflected medially, allowing exposure of the iliac vein. A
similar approach to the common iliac vein or inferior vena cava with divi-
sion of the right c o m m ~ n iliac artery has been described.
321
It is conceptually useful to divide the superior mesenteric vein (SMV)
into the retropancreatic and infrapancreatic portions. If an SMV injury is
suspected, exposure is facilitated by division of the ligament of Treitz and
elevation of the fourth portion of the duodenum. If the bleeding appears to
be retropancreatic, the pancreas should be divided with a stapler to allow
exposure. In cases of infrapancreatic SMV injuries, division of the colon
and tracing of the middle colic vein proximally may facilitate identifica-
tion of the SMV.
Repair of an aortic injury begins with vascular control proximal and
distal to the injury. Primary repair of the aorta is preferred whenever pos-
sible. This is performed with 3-0 or 4-0 monofilament polypropylene su-
Curr Prabl Surg, August 1996
681
ture and standard vascular technique. Bleeding lumbar arteries should be
ligated. If two lacerations are located very close together, they may be
connected, debrided, and closed as a single suture line.
Special considerations. Preceliotomy thoracotomy for cross-clamping
of the aorta is controversial. Improvement in survival has been re-
ported,65.66.322-325 but this maneuver has the disadvantage of promoting hy-
pothermia by opening another body cavity and the additional disadvantage
of creating new cut surfaces from which the patient may bleed. Intraaortic
balloon occlusion has been described as a method of achieving proximal
aortic control,7o.72.326 if exposure is particularly difficult. Distal control of
the infrarenal aorta usually is not difficult, but if direct placement of a
clamp is not possible, intraluminal balloon occlusion may allow control
while exposure is improved.
When extensive aortic damage prevents primary repair, a 12 or 14 mm
polytetrafluoroethylene interposition graft should be used. It is important
to realize that polytetrafluoroethylene can be used safely even in the face of
contamination with gastrointestinal contents.70.72.326.327 Suture lines should
be covered with well-vascularized tissue in all circumstances. Although
saphenous vein has been traditionally recommended for use in contami-
nated fields, it has a tendency to digest and blowout when infected.
328
Furthermore the saphenous vein is too small for use as an aortic substitute
without the use of complex and lengthy spiral suture techniques. Intimal
flaps can be managed with flap suture.
329
Inferior vena cava (nonhepatic). General considerations. Once expo-
sure and control have been achieved, the inferior vena' cava is carefully
inspected to determine the magnitude of injury. After the area of injury has
been identified, the celiotomy pads previously placed over the vena cava
may be removed and the injury directly occluded with a finger. Other op-
tions for direct control include the use of a sponge stick to occlude the vena
cava on either side of the laceration, a side-biting vascular clamp, or Allis
clamps applied in series along the laceration. No attempt should be made
to encircle the inferior vena cava, because this will result in avulsion of
lumbar veins, worsening an already complex situation. If it appears that
there is only a single anteriorly located injury, the interior ofthe cava should
be examined to exclude a posterior laceration. Such a laceration will be
suggested by persistent bleeding despite apparently adequate control.
Simple venorrhaphy with 4-0 or 5-0 monofilament vascular suture will
adequately repair simple anterior or lateral lacerations. Posterior lacera-
tions may be repaired either by gentle rotation of the inferior vena cava, or,
preferably, transluminally. The transluminal repair may require extension
of the anterior laceration for good exposure. Repair may be performed
682 Curr Probl Surg, August 1996
either with a double- or single-armed suture, but in any event knots must be
situated extraluminally.
Complete transection is ideally managed with end-to-end anastomosis
without tension. This may require debridement of injured vein. If end-to-
end anastomosis is not possible, successful repair with prosthetic mate-
riaP30 or spiral saphenous vein grafts has been described, although these
are too time-consuming to be useful in the patient in extremis.
Special considerations. With extensive injuries to the infrarenal vena
cava, ligation provides rapid hemostasis.
33
o,331 This may be associated with
venous gangrene.
331
Because of the risk of renal infarction, suprarenal caval
injuries must be repaired.
Iliac vessels. General considerations. The common iliac artery should
be repaired when possible, but this may be limited by the feasibility of
aortic and distal iliac mobilization.
332
Synthetic grafts have been used with
success even in the face of contamination.
333
33
-l Either end-to-end or end-
to-side iliac to iliac anastomosis may be used. Another choice is to perform
an anastomosis from the ipsilateral internal iliac artery to the external iliac
artery.335 The internal iliac artery may be ligated without impunity, but
ligation of the external or common iliac artery is associated with an unac-
ceptable limb ischemia rate.
Iliac veills. Experience from the Vietnam Vascular Registry led to the
recommendation that iliac venous injuries be repaired.
336
Arguments in fa-
vor of repair were avoidance of acute venous gangrene, and later chronic
venous hypertension. It has been proposed that even though these venous
repairs often have thrombosis, even a few days of patency may allow col-
lateral paths of venous outflow to develop.336 More recent reports, how-
ever, indicate that pelvic veins may be ligated with an acceptably low inci-
dence of morbidity.337.338 These reports emphasize that venous ligation should
be accompanied by the use of limb elevation and compression stockings.
Abdomillal visceral vessels. The celiac axis is well collateralized via the
superior mesenteric artery (SMA)339; injuries here are best ligated. There
appear to be no short-term complications resulting from ligation of the
celiac artery in young patients.
5
SMA. Injuries to the SMA are classified as retropancreatic 'or
infrapancreatic. Extensive collaterals to the retropancreatic SMA via the
celiac system allow for safe ligation of these injuries if necessary,5 although
repair is recommended, if possible. The infrapancreatic SMA is distal to
these collaterals and should be repaired to avoid midgut ischemia. This
may involve simple arteriorrhaphy, or if the damage is extensive, a bypass
graft from the aorta. Felician0
5
suggests that the proximal anastomosis
should be placed distally on the aorta because of the possibility of pancre-
Curr Probl Surg. August 1996 683
atic digestion of a juxtapancreatic suture line. Care should be taken to avoid
kinking of the graft. Repairs usually produce good results, although
thrombosis of the SMA with massive small bowel necrosis and short gut
syndrome have been reported after repair in one patient.
340
Our practice is
to return patients with SMA injuries to the operating room for a "second
look" at the bowel. Because these patients are usually in shock and have
coagulopathy, we do not include anticoagulation as part of the immediate
postoperative management.
Inferior mesenteric artery. The inferior mesenteric artery may be l!gated.
Collateral flow is provided via the left colic and upper rectal vessels. The
single exception is the patient with evidence of atherosclerotic disease of
the visceral vessels in whom a large meandering mesenteric vessel is noted.
In this situation consideration must be given to repair or aortic reimplantation
of the inferior mesenteric artery.
8MY. Ideally, the SMV should be repaired, if possible. It is important to
realize, however, that the SMV can be ligated with a low rate of small
bowel necrosis.
5
,205,338 In a collected series of 110 patients with 33 SMV
ligations and 77 SMV repairs, ligation was associated with an overall mor-
tality of 15% versus a mortality of 36% for repair.
341
We therefore recom-
mend that the SMV be repaired only if the injury is simple and easily
exposed and the patient is stable. All other SMV injuries should be ligated.
Whether repair or ligation is selected, exposure is difficult because of the
location of the vessel and attendant hematoma. Large fluid needs can be
anticipated in patients who have had SMV ligation because of significant
bowel edema and fluid sequestration. Support of the intravascular volume
must be maintained.
References
1. Shackford SR, Bagram SGA, Rozycki GS, et al. On developing a career in
trauma and surgical critical care. J Trauma 1994;37:700.4.
2. Morris JA Jr, Auerback P, Marshall GA, et al. The trauma score as a triage tool
in the prehospital setting. JAMA 1986;256: 1319-25.
3. American College of Surgeons. ACS Optimal Resource Document. Chicago:
ACS, 1993.
4. Fallon WF, Morris JAJr, Scalea TM, eds. The trauma patient in extremis. Trauma
Quarterly 1993;10: 1-105.
5. Feliciano D. Abdominal vascular injuries. Surg Clin North Am 1988;68:741-55.
6. Adkins RB, Bitseff EL, Meacham PW. Abdominal vascular injuries. South Med
J 1985;78:1152-60. '
7. Jackson MR, Olson DW, Beckett WC, et al. Abdominal vascular trauma: a
review of 106 injuries. Am Surg 1992;58:622-6.
8. McMillan RW, Landreneau RM, McCormick GM, et al. Major vascular injuries
of the torso. South Med J 1992;85:375-7.
684 Curr Probl Surg, August 1996
9. Morris JA Jr, MacKenzie EJ, Damiano AM, et 01. Mortality in trauma
patients: the interaction between host factors and severity. J Trauma
1990;30: 1469-75.
10. Von Aalst J, Morris JA Jr, Yates HK, et 01. Severely injured geriatric patients
return to independent living: a study of factors influencing function and
independence. J Trauma 1991 ;31: 1096- 102.
11. Morris JA Jr, MacKenzie EJ, Edelstein SL. The effect of pre-existing conditions
on mortality in trauma patients. JAMA 1990;263: 1942-6.
12. MacKenzie EJ, Morris JA Jr, Edelstein SL. Effect of pre-existing disease on
length of hospital stay in trauma patients. J Trauma 1989;29:757-65.
13. Dunham CM, Siegel JH, Weireter L, et 01. Oxygen debt and metabolic
acidemia as quantitative predictors of mortality and the severity of the ischemic
insult in hemorrhagic shock. Crit Care Med 1991;19:231-43.
14. Rotondo MF, Schwab CW, McGonigal MD, et al. "Damage control": an
approach for improved survival in exsanguinating penetrating abdominal
injury. J Trauma 1993;35:375-82.
15. Eddy VA, Morris JA Jr. Secondary resuscitation: an organ systems approach.
Trauma Quarterly 1993;10:71-87.
16. Wudel J, Morris JA Jr, Bass SM. Massive transfusion: outcome in blunt trauma
patients. J Trauma 1991 ;31 :1-7.
17. Nelson LD, Rutherford EJ. Monitoring mixed venous oxygen. Respir Care
1991;37:747-54.
18. Miller RS, Nelson LO, Rutherford EJ, et al. Synchronized independent lung
ventilation in the management of a unilateral pulmonary contusion with
massive hemoptysis when traditional ventilatory treatment failed: case report.
J Tenn Med Assoc 1992;83:374-5.
19. Miller RS, Nelson LD, DiRusso SM, et 01. High-level positive end-expiratory
pressure management in trauma-associated adult respiratory distress
syndrome. J Trauma 1992;33:284-90.
20. Cady LO, Weil MH, Afifi M. Quantification of severity of critical illness with
special reference to blood lactate. Crit Care Med 1983; 1:75.
21. Caine RY, McMaster p, P e n t l o ~ BD. The treatment of major liver trauma by
primary packing with' transfer of the patient for definitive treatment. Br J Surg
1979;66:228-9.
22. Carmona RH, Peck DZ, Miller FB, et 01. The role of packing in planned
reoperation in severe hepatic trauma. J Trauma 1984;94:779-84.
23. Feliciano DV, Mattox KL, Burch JM, et 01. Packing for control of hepatic
hemorrhage. J Trauma 1986;26: 738-43.
24. Ivatury RR, Nallathambi M, Gunduz Y, et 01. Liver packing for uncontrolled
hemorrhage: a reappraisal. J Trauma 1986;26:744-53.
25. Svoboda JA, Peter ET, Dang Cv, et 01. Severe liver trauma in the face of
coagulopathy: a case for temporary pocking and early reexploration. Am J
Surg 1982;144:717-2l.
26. Carrillo C, Fogler RJ, Shaftan Gw. Delayed gastrointestinal reconstruction
following massive abdominal trauma. J Trauma 1993;34:233-5.
27. Cue GI, Cryer HG, Miller FB, et 01. Packing and planned reexploration for
hepatic and retroperitoneal hemorrhage: critical refinements of a useful
technique. J Trauma 1990;30: 1007-13.
Curr Probl Surg, August 1996 685
28. Talbert S, Trooskin S, Scalea T, et al. Packing and reexploration for patients
with nonhepatic injuries. J Trauma 1992;33: 121-5.
29. Stone HH, Strom PR, Mullins RJ. Management of the major coagulopathy
with onset during laparotomy. Ann Surg 1983;197:532-5.
30. Burch JM, Oritz VB, Richardson RJ. Abbreviated laparotomy and planned
reoperation for critically injured patients. Ann Surg 1992;215:476-84.
31. Morris JA Jr, Eddy VA, Blinman TA, et al. The staged celiotomy for trauma:
issues in unpacking and reconstruction. Ann Surg 1993;217:576-86.
32. Baracco-Gandolfo V, Vidarte 0, Barocco-Miller V, et 01. Prolonged closed
liver packing in severe hepatic trauma: experience with 36 patients. J Trauma
1986;26:754-6.
33. Bender JS, Bailey CE, Saxe JM, et al. The technique of visceral'packing:
recommended management of difficult fascial closure in trauma patients. J
Trauma 1994;36: 182-5.
34. Krige JEJ, Bornman PC, Terblanche J. Therapeutic perihepatic packing in
complex liver trauma. Br J Surg 1992;79:43-6.
35. Sharp i<MI, Locicero RJ. Abdominal packing for surgically uncontrollable
hemorrhage. Ann Surg 1992;215:467-74..
36. Collins JA. Problems associated with the massive transfusion of stored blood.
Surgery 1974;75:274-93.
37. Frykberg ER, Dennis JW, Butcher JL. Massive transfusion: history,
pathophysiology, and management. Trauma Quarterly 1993;10: 12-31.
38. Gentilello LM, Cobean RA, Offner PJ, et al. Continuous arteriovenous
rewarming: rapid reversal of hypothermia in critically ill patients. J Trauma
1992;32:316-27.
39. Davis JW, Shackford SR, Holbrook TL. Base deficit as a sensitive indicator of
compensated shock and tissue oxygen utilization. Surg Gynecol Obstet
1991;173:473-6.
40. Davis Jw, Shackford SR, Mackersie RC, et 01. Base deficit as a guide to volume
resuscitation. J Trauma 1988;28: 1464-7.
41. Rutherford EJ, Morris JA Jr, Reed GW, et 01. Base deficit stratifies mortality and
determines therapy. J Tra'uma 1992;33:417-23.
42. Hoyt DB, Bulger'EM, Knudson MM, et 01. Death in the operating room: an
analysis of a multi-center experience. J Trauma 1994;37:426-32.
43. Gundry SR, Williams S, Burney RE, Cho KJ, Mackenzie JR. Indications for aor-
tography in blunt thoracic trauma: a reassessment. J Trauma 1982;22:664-71.
44. Schwab Cw, Lawson RB, Lind JF, Garland LW. Aortic injury: comparison of
supine and upright portable chest films to evaluate the widened mediastinum.
Ann Emerg Med 1984;13:896-9.
45. Dalldorf PG, McCarthy MC, Tarver RD, et al. Traumatic rupture of the aorta:
indications for aortography. Am Surg 1990;56:500-3. '
46. Hoff SJ, Shotts SO, Eddy VA, et 01. Outcome of isolated pulmonary contusion
in blunt trauma patients. Am Surg 1994;60: 138-42.
47. Lee RB, Morris JA Jr. Current concepts in the management of flail chest. J
Tenn Med Assoc 1988;83:631-3. '
48. Lee RB, Morris JA Jr, MacKenzie EJ, et al. Three or more rib fractures as an
indicator for transfer to a level I trauma center: a population-based study. J
Trauma 1990;30:689-94.
686 Curr Probl Surg, August 1996
49. Lee RB, Morris JA Jr, Parker RS. Presence of three or more rib fractures as an
indicator of need for interhospital transfer. J Trauma 1989;29:795-800.
50. American College of Surgeons. Advanced Trauma Life Support Course Book.
Chicago: ACS, 1990.
51. Merrill WH, Lee RB, Hammon JW Jr, Frist WH, Stewart JR, Bender HW Jr.
Surgical treatment of acute traumatic tear of the thoracic aorta. Ann Surg
1988;207:699-706.
52. Richardson JD, Wilson ME, Miller FB. The widened mediastinum: diagnostic
and therapeutic priorities. Ann Surg 1990;211 :731-6.
53. Smith M, Cassidy J, Souther S, et 01. Transesophageal echocardiography in
the dignosis of traumatic rupture of the aorta. N Engl J Med 1995;332:356-62.
54. Feliciano DV. Management of traumatic retroperitoneal hematoma. Ann Surg
1990;211: 109-23.
55. Goins WA, Rodriguez A, Brathwaite CEM. Retroperitoneal hematoma after
blunt trauma. Surg Gynecol Obstet 1992; 174:281-90.
56. Grieco JG, Perry JF. Retroperitoneal hematoma following trauma: its clinical
importance. J Trauma 1980;20:733-6.
57. Richardson JD, Miller RB. Splenic injury. In: Gay S, editor. Current surgical
therapy. St Louis: Mosby-Year Book, Inc, 1992:858-61.
58. Jurkovich GJ, Esposito TJ, Maier RV. Resuscitative thoracotomy performed in
the operating room. Am J Surg 1992;163:463-8.
59. Scalea TM, Mann R. Resuscitative thoracotomy. Trauma Quarterly 1993;10:32-44.
60. Selivanov V, Chi HS, Alverdy JC, Morris JA Jr, Sheldon GF. Mortality in
retroperitoneal hematoma. J Trauma 1984;24: 1022-7.
61. Miller RS, Morris JA Jr. Retroperitoneal injury. In Cameron J, editor. Current
surgical therapy. St Louis: BC Decker, 1992:861-5.
62. Canizaro PC, Pessa ME. Management of massive hemorrhage associated
with abdominal trauma. Surg Clin North Am 1990;70:621-34.
63. Conn JJ, Trippel 0, Bergan J. A new atraumatic aortic occluder. Surgery
1968;64: 1158-60.
64. Millikan J, Moore E. Outcome of resuscitative thoracotomy and descending
aortic occlusion performed in the operating room. J Trauma 1984;
24:387-92.
65. Sankaran 5, Lucas C, Walt AJ. Thoracic aortic clamping for prophylaxis against
sudden cardiac arrest during laparotomy for acute massive hemoperitoneum.
J Trauma 1975;15:290-6.
66. Ledgerwood AM, Kazmers M, Lucas CEo The role of thoracic aortic occlusion
for massive hemoperitoneum. J Trauma 1976; 16:610-5.
67. Oyama M, McNamara JJ, Suehiro GT, Suehiro A, Sue-Ako K. The effects of
thoracic aortic cross-clamping and declamping on visceral organ blood flow.
Ann Surg 1983; 197:459-63.
68. Austin OM, Redmond Hp, Burke PE, Grace PA, Bouchier-Hayes DB. Vascular
trauma: a review. J Am Call Surg 1995;181:91-108.
69. Gallup DG, Nolan TE, Smith RP. Primary mass closure of midline incisions
with a continuous polyglyconate monofilament absorbable suture. Obstet
Gynecol 1990;76:872-5.
70. Gupta BK, Khaneja SC, Flores L, et 01. The role of intra-aortic balloon occlusion
in penetrating abdominal trauma. J Trauma 1989;29:861-5.
Curr Probl Surg, August 1996 687
71. Paggetti RS, Moore EE, Moore FA, et 01. Balloon tamponade for bilobar
transfixing hepatic gunshot wounds. J Trauma 1992;33:694-7.
72. Scalea TM, Scalfani SJA. Angiographically placed balloons for arterial control:
a description of a technique. J Trauma 1991 ;31: 1671-7.
73. Thomas S, Dulchavsky S, Diebel l. Balloon tamponade for liver injuries: case
report. J Trauma 1993;33:448-9.
74. Baumgartner F, White GH, White RA, et al. Delayed, exsanguinating pelvic
hemorrhage after blunt trauma without bony fracture: case report. J Trauma
1990;30: 1603-5.
75. Miller RS, Morris JA Jr. Retroperitoneal hematoma: a case report. J Tenn Med
Assoc 1991;84:227-9.
76. Ross SE, Cobean RA, Hoyt DB, et al. Blunt colonic injury: a multicenter review.
J Trauma 1992;33:379-84.
77. Strasen KM, Berne Tv. Wound infection in patients with traumatic small intestinal
injuries. Am Surg 1991 ;57:803-5.
78. Talton OS, Craig MH, Hauser CJ, et 01. Major gastroenteric injuries from
blunt trauma. Am Surg 1995;61 :69-73.
79. Ivatury RR, Zubowski R, Psarras P, et 01. Intra-abdominal abscess after
penetrating abdominal trauma. J Trauma 1988;28: 1238-43.
80. George SM, Fabian TC, Voeller GR, et 01. Primary repair of colon wounds.
Ann Surg 1989;209:728-34.
81. Livingstone SO, Grayson J, Frim J, et 01. Effect of cold exposure on various
sites of temperature measurements. J Appl Physiol 1983;54:R1025-31.
82. Webb G. Comparison of esophageal and tympanic temperature monitoring
during cardiopulmonary bypass. Anesth Analg 1973;52:729-33.
83. Reed RL, Ciavarella 0, Heimbach OM. Prophylactic platelet administration
during massive transfusion: a prospective, randomized double-blind clinical
study. Ann Surg 1986;203:40-8.
84. Morris JA Jr, Eddy VA, Rutherford EJ. The staged celiotomy: damage control.
Trauma Quarterly 1993;10:60-70.
85. Harke H, Rahman S. Hemostatic disorders in massive transfusion. Bibl
Haematol 1980;4.6: 179-88.
86. Miller FB, Richardson JO, Seligson D. Pelvic fracture. In: Cameron JL, editor.
Current surgical therapy. St Louis: BC Decker, 1992:873-9.
87. Johnson KD, Cadambi A, Seibert GB. Incidence of adult respiratory distress
syndrome in patients with multiple musculoskeletal injuries: effect of early
operative stabilization of fractures. J Trauma 1985;25:375-84.
88. Greene MA, Mullins RJ, Malangoni MA, et 01. Laparotomy wound closure
with absorbable polyglycolic mesh. Surg Gynecol Obstet 1993; 176:
213-8.
89. Aprahamian C, Whittman DH, Bergstein JM, et 01. Temporary abdominal
closure (lAC) for planned relaparotomy (ettapenlavage) in trauma. J Trauma
1990;30:719-23.
90. Saxe JM, Ledgerwood AM, Lucas CEo Management of the difficult abdominal
closure. Surg Clin North Am 1993;73:243-51.
91. Smith PC, Tweddell JS, BesseyPQ. Alternative approaches to abdominal wound
closure in severely injured patients with massive visceral edema. J Trauma
1992;32: 16-20.
688 Curr Probl Surg, August 1996
92. Feliciano DY, Burch JM. Towel clips, silos, and heroic forms of abdominal
closure. In: Maull KI, editor. Advances in trauma and critical care. Chicago:
CV Mosby, 1991 :231-50.
93. Voyles CR, Richardson JD, Bland KJ. Emergency abdominal wall reconstruction
with polypropylene mesh. Ann Surg 1981;194:219-23.
94. Mathes SJ, Stone HH. Acute traumatic losses of abdominal wall substance. J
Trauma 1975;15:386-91.
95. Boyd W. Use of marlex mesh in acute loss of the abdominal wall due to
infection. Surg Gynecol Obstet 1977;144:251-2.
96. Jurkovich GJ, Greiser WB, Luterman A, et 01. Hypothermia in trauma victims:
an ominous predictor of survival. J Trauma 1987;27:1019-22.
97. Heimbach D. Hemostasis in massively transfused trauma patients. In: Fresh
frozen plasma: indications and risks. Bethesda: NIH Consensus Development
Conference, 1984:38-9.
98. Ferrara A, MacArthur JD, Wright HK, et 01. Hypothermia and acidosis worsen
coagulopathy in the patient requiring massive transfusion. Am J Surg
1990;160:515-8.
99. Ralph-Slotman GJ, Jed EH, Birchard J<YV. Adverse effects of hypothermia in
postoperative patients. Am J Surg 1985;149:495-501.
100. Steineman S, Shackford SR, Davis Jw. Implications of admission hypothermia
in trauma patients. J Trauma 1990;30:200-2.
101. Genti/ello LM, Jurkovich GJ, Moujaes S. Hypothermia and injury:
thermodynamic principles of prevention and treatment. Perspectives in General
Surgery 1991;2:25.
102. Gentilello L. Advances in the management of hypothermia. Surg Clin North
Am 1995;75:243-56.
103. Reed RL, Bracey AW, Hudson JD, et al. Hypothermia and blood coagulation:
dissociation between enzyme activity and clotting factor levels. Circ Shock
1990;32: 141-52.
104. Kurrek MM, Reed RL. Effect of hypothermia on enzymatic activity of thrombin
and plasmin. Surg Forum 1987;38:221-3.
105. Roizen MF, Sohn YJ, L:Hommedieu CS. Operating room temperature prior to
surgical draping-effect on patient temperature in recovery room. Anesth Analg
1980;59:852-7.
106. Gentilello LM, Rifley WJ. Continuous arteriovenous rewarming: report of a
new technique for treating hypothermia. J Trauma 1991 ;31 :1151-4.
107. Otto RJ, Metzler MH. Rewarming from experimental hypothermia: comparison
of heated aerosol inhalation, peritoneal lavage, and pleural lavage. Crit
Care Med 1988;16:869-75.
108. Harrigan C, Lucas CE, Ledgerwood ANI. The effect of hemorrhagic shock on
the clotting cascade in iniured patients. J Trauma 1989;29: 1416-22.
109. Harrigan C, Lucas CE, Ledgerwood ANI, et al. Primary hemostasis after massive
transfusion for injury. A ~ Surg 1982;29: 1416-22.
110. Phillips TF, Soulier G, Wilson RF. Outcome of massive transfusion exceeding
two blood volumes in trauma and emergency surgery. J Trauma 1987;27:
903-10.
111. Wilson RF, Dulchavsky SA, Soulfier G, et al. Problems with 20 or more blood
transfusions in 24 hours. Am Surg 1987;53:410-7.
Curr Probl Surg, August 1996 689
112. Wilson RF, Mammen E, Walt AJ. Eight years experience with massive blood
transfusion. J Trauma 1971;11 :275-85.
113. Krivioja A, Myllynen P, Rokkanen P. Survival after massive transfusions exceeding
20-unit blood transfusion need. Iniury 1991 ;57:398-40l.
114. Counts RB, Heimbach KL, Jordan GL. Hemostasis in massively transfused
trauma patients. Ann Surg 1979;190:91-9.
115. Morris JA Jr, Wilcox TR, Reed Gw, et 01. Safety of the blood supply: surrogate
testing and transmission of Hepatitis C after massive transfusion. Ann Surg
1994;219:517-26.
116. Sloop GO, Friedberg RC. Complications of blood transfusion: how to recognize
and respond to noninfectious reactions. Postgrad Med 1995;98:159.-72.
117. Welborn JL, Hersch J. Blood transfusion reactions. Which are life-threatening
and which are not? Postgrad Med 1991 ;90: 125-8.
118. Rosemurgy AS, Hart MB, Murphy CG, et al. Infection after injury: association
with blood transfusion. Am Surg 1992;58:104-7.
119. Alter HJ, Holland PY, Morrow AG, Purcell RH, Feinstone SM, Moritsugu Y.
Clinical and serological analysis of transfusion-associated hepatitis. Lancet
1975;2:838-4l.
120. American College of Surgeons. Indications for transfusion. In: Wilmore 0,
Brennan M, Harken A, et 01., editors. Care of the surgical patient. New York:
Scientific American, Inc, 1992:4.
121. Cue JI, Peyton JC, Malangoni MA. Does blood transfusion of hemorrhagic
shock induce immunosuppression? J Trauma 1992;32:613-7.
122. Waymack Jp, Rapien J, Garnett 0, et al. Effect of transfusion on immune
function in a traumatized animal model. Arch Surg 1986;121 :50-5.
123. Shoemaker WC, Appel PC, Kram HB, et al. Tissue oxygen debt as a
determinant of lethal and nonlethal postoperative organ failure. Crit Care
Med 1988;16:1117-20.
124. Morris JA Jr, Sanchez A, Boss SM, et al. Trauma patients return to productivity.
J Trauma 1991 ;31 :827-34.
125. Martin OJ, Lucas CE, Ledgerwood AM. Fresh frozen plasma supplement to
massive red blood cell transfusion. Ann Surg 1985;202:505-11.
126. Noe DA, Graham SM, Luff R, et al. Platelet counts during rapid massive
transfusion. Transfusion 1982;22:392-5.
127. Shoemaker WC, Appel PL, Kram HB, et 01. Prospective trial of supranormal
values of survivors as therapeutic goals in high.risk surgical patients. Chest
1987;94: 1176-86.
128. Edwards JO, Brown CS, Nightingale P, et al. Use of survivors cardiorespiratory
values as therapeutic goals in septic shock. Crit Care Med 1989; 17: 1098-1 03.
129. Hirshberg A, Wall MJ, Mattox KL. Planned reoperation for trauma: a two year
experience with 124 consecutive patients. J Trauma 1994;37:365-9.
130. Diebel LN, Wilson RF, Tagett MG, et al. End-diastolic volume: a better indicator
of preload in the critically ill. Arch Surg 1992;127:817-2l.
131. Chang M, Blinman P, Rutherford E, Nelson L, Morris JA, Jr. Preload assessment
in trauma patients during large volume resuscitation. Arch Surg (in press).
132. Cheatham ML, Nelson LD, Chang MC, et al. Right ventricular end-diagnostic
volume index as a predictor of preload status in patients on positive end
expiratory pressure. Crit Care Med (in press).
690 Curr Probl Surg, August 1996
133. Cheatham ML, Chang MC, Eddy VA, et al. Right ventricular end-diagnostic
volume index and pulmonary artery occlusion pressure vs cardiac index during
titration of PEEP. Chest (in press).
134. Nelson L. Continuous venous oximetry in surgical patients. Ann Surg
1986;203:329-33.
135. Hoff SJ, Reilly MK, Merrill WH, et a!. Analysis of blunt and penetrating injury
of the innominate and subclavian arteries. Am Surg 1994;60: 151-4.
136. Chang MC, Rutherford EJ, Morris JA Jr. Base deficit as a guide to injury severity
and volume resuscitation. J Tenn Med Assoc 1993;86:59-61.
137. Siegel JH, Rivkind AI, Dalal S, et a!. Early physiologic predictors of injury
severity and death in blunt multiple trauma. Arch Surg 1990; 125;498-
508.
138. Weil MH, Afifi AA. Experimental and clinical studies on lactate and pyruvate
as indicators of the severity of acute circulatory failure (shock). Circulation
1970; 10:989-1001.
139. Abramson D, Scalea TM, Hitchcock R, et al. Lactate clearance and survival
following injury. J Trauma 1993;35:584-9.
140. Eddy VA, Vitski JL, Rutherford EJ, et 01. Aggressive use of ICP monitoring is
safe and alters patient care. Am Surg 1995;61 :24-9.
141. Cruz J, Gennarelli T, Alves W. Continuous monitoring of cerebral hemodynamic
reserve in acute brain injury: relationship to changes in brain swelling. J Trauma
1992;32:629-34.
142. Eddy VA, Key Sp' Morris JA Jr. Abdominal compartment syndrome: etiology,
detection, and management. J Tenn Med Assoc 1994;87:55-7.
143. Richardson JD, Trinkle JK. Hemodynamic and respiratory alterations with
increased intra-abdominal pressure. J Surg Res 1976;20:401-4.
144. Kron IL, Harman PK, Nolan SP. The measurement of intra-abdominal pressure
as a criterion for abdomial reexploration. Ann Surg 1984; 199:28-30.
145. Cullen DJ, Coyle Jp, Teplick R, et al. Cardiovascular, pulmonary, and renal
effects of massively increased intra-abdominal pressure in critically ill patients.
Crit Care Med 1989;17:118-21.
146. Scalea TM, Phillips TF, Goldstein AS, et 01. Injuries missed at operation: nemesis
of the trauma surgeon. J Trauma 1988;28:962-7.
147. De Toma G, Mingoli A, Modini C, et 01. The value of angiography and selective
hepatic artery embolization for continuous bleeding affer surgery in liver
trauma: case reports. J Trauma 1994;37:508-11.
148. Fandrich BL, Gnanadev DA, Jaecks R, et a!. Selective hepatic artery
embolization as an adjunct to liver packing in severe hepatic trauma: case
report. J Trauma 1989;29: 1716-8.
149. Krukowski ZH, Cusick EL, Engeset J, et al. Polydioxanone or polypropylene
for closure of midline abdominal incisions: a prospective comparative clinical
trial. Br J Surg 1987;74:828-30.
150. Schoetz DJ, Coller JA, Veidenheimer Me. Closure of abdominal wounds with
polydioxanone. Arch Surg 1988; 123: 72-4.
151. Orr Jw, Orr PF, Barrett JM, et al. Continuous or interrupted fascial closure: a
prospective evaluation of no. 1 Maxon suture in 402 gynecologic procedures.
Am J Obstet 1990;163:1485-9.
152. Trimbos JB, Smit /8, Holm JP, et al. A randomized clinical trial comparing two
Curr Probl Surg. August 1996 691
methods of fascia closure following midline laparotomy. Arch Surg
1992;127: 1232-4.
153. Richards PC, Balch CM, Aldrete JS. Abdominal wound closure: a randomized
prospective study of 571 patients comparing continuous vs interrupted suture
techniques. Ann Surg 1983; 197:238-43.
154. Carlson MA, Ludwig KA, Condon RE. Ventral hernia and other complications
of 1,000 midline incisions. South Med J 1995;88:450-3.
155. Seid MH, McDaniel-Owens M, Poole GY, et al. A randomized trial of
abdominal incision suture technique and wound strength in rats. Arch Surg
1995;130:394-7.
156. Rappaport W, Allen R, Chvapil M, et al. A comparison of parallel versus
perpendicular placement of retention sutures in abdominal wound closure.
Am Surg 1990;56:618-23.
157. Fabian TC, Croce MA, Stewart RM, Pritchard FE, Minard G, Kudsk KA. A
prospective analysis of diagnostic laparoscopy in trauma. Ann Surg
1993;217:557-64.
158. Usher FC, Bannon JP. Marlex mesh, a new plastic mesh for replacing tissue
defects. Arch Surg 1959;78:131-7.
159. Fansler RF, Taheri P, Cullinane C, et al. Polypropylene mesh closure of the
complicated abdominal wound. Am J Surg 1995;170: 15-8.
160. Baker Sp' O'Neill B, Haddon W Jr, et al. The injury severity score: a method
for describing patients with multiple injuries and evaluating emergency care.
J Trauma 1974;14:187-96.
161. Mays E. Hepatic trauma. Curr Probl Surg 1976;13:1-73.
162. Feliciano DY, Pachter HL. Hepatic trauma revisited. Curr Probl Surg
1989;26:453-524.
163. Pachter. H, Knudson M, Esrig B, et al. Status of nonoperative management of
blunt adult hepatic injuries: a multi-center experience with 404 patients. J
Trauma 1996;40:31-8.
164. Feliciano D. Surgery for liver trauma. Surg Clin North A ~ 1989;69:273-84.
165. Miller D. Median sternotomy extension of abdominal incision for hepatic
lobectomy. Ann Surg 1972;185:613-8.
166. Fullen WD, McDonough JJ, Popp MJ, et al. Sternal splitting approach for
major hepatic or retrohepatic vena cava injury. J Trauma 1974; 14:903-11.
167. Cheatham JE Jr, Smith EI, Tunell Wp, et al. Nonoperative management of
subcapsular hematomas of the liver. Am J Surg 1980;140:852-7.
168. Knudson MM, Lim RC, Oakes DD, et al. Nonoperative management of blunt
liver injuries in adults: the need for continued surveillance. J Trauma
1990;30: 1494-500.
169. Sherman HF, Savage BA, Jones LM, et al. Nonoperative management of
blunt hepatic injuries: safe at any grade? J Trauma 1994;37:616-21.
170. Cogbill TH, Moore EE, Jurkovich GJ, et al. Severe hepatic trauma: a multi-
center experience with 1335 liver injuries. J Trauma 1988;28: 1433-8.
171. Go PM, Goodman GR, Bruhn EW, et al. The argon beam coagulator provides
rapid hemostasis of experimental hepatic and splenic hemorrhage in
anticoagulated dogs. J Trauma 1991 ;31 :1294-300.
172. Ochsner MG, Maniscalco-Therberge ME, Champion HR. Fibrin glue as a
hemostatic agent in hepatic and splenic trauma. J Trauma 1990;30:884-7.
692 Curr Probl Surg, August 1996
173. De 10 Garza J, Rumsey E. Fibrin glue and hemostasis in liver trauma: a case
report. J Trauma 1990;30:512-3.
174. Kram HB, Rerben BI, Fleming AW, et 01. Use of fibrin glue in hepatic trauma.
J Trauma 1988;28: 1195-201.
175. Berguer R, Staerkel RL, Moore EE, et 01. Warning: fatal reaction to the use of
fibrin glue in deep hepatic wounds: case reports. J Trauma 1991 ;31 :408-11.
176. Feliciano DY, Mattox KL, Jordan GL, et 01. Management of 1000 consecutive
cases of hepatic trauma (1974-1984). Ann Surg 1986;204:438-45.
177. Pachter HL, Spencer FC, Hofstetter SR, et 01. Experience with the finger fracture
technique to achieve intra-hepatic hemostasis in 75 patients with severe injuries
ofthe liver. Ann Surg 1983;197:771-8.
178. Fabian TC, Stone HH. Arrest of severe liver hemorrhage by an omental pack.
South Med J 1980;73: 1487-90.
179. Stone HH, Lamb JM. Use of pedicled omentum as an autogenous pack for
control of hemorrhage in major injuries of the liver. Surg Gynecol Obstet
1975; 141 :92-4.
180. Pringle J. Notes on the arrest of hepatic hemorrhage due to trauma. Ann
Surg 1908;48:5418.
181. Pachter HL, Spencer Fe. Recent concepts in the treatment of hepatic trauma:
facts and fallacies. Ann Surg 1979;190:4239.
182. Huguet C, Nordlinger B, Galopin JJ, et 01. Normothermic hepatic vascular
exclusion for extensive hepatectomy. Surg Gynecol Obstet 1978; 147:689-93.
183. Moore EE, Shackford SR, Pachter HL, et 01. Organ injury scaling: spleen, liver,
and kidney. J Trauma 1989;29: 1664-6.
184. Beelen RHJ, Fluitsma OM, Hoefsmit ECM. The cellular composition of omentum
milky spots and the ultra-structure of milky spot macrophages and reticulum
cells. J Reticuloendoth Soc 1980;28:585-99.
185. Jurkiewicz MJ, Nahai F. The omentum: its use as a free vascularized graft for
reconstruction of the head and neck. Ann Surg 1982;195:756-65.
186. Trooskin SZ, Pierce RA, Deak SB, et al. The effect of viable omentum on early
bile leakage and healing of liver lacerations. J Trauma 1989;29:47-50.
187. Beal S. Fatal hepatic hemorrhage: an unresolved problem in the management
of complex liver injuries'. J Trauma 1990;30: 163-9.
188. Beal SL, Ward RE. Successful atrial caval shunting in the management of
retrohepatic venous injuries. Am J Surg 1989;158:409-13.
189. Buechter KJ, Sereda 0, Gomez G, et al. Retrohepatic vein injuries: experience
with 20 cases. J Trauma 1989;29:1698-704.
190. Menegaux F, Langlois P, Chigot JP. Severe blunt trauma of the liver: study of
mortality factors. J Trauma 1993;35:865-9.
191. Moore EE. Critical decisions in the management of hepatic trauma. Am J
Surg 1984;148:712-6.
192. Pachter HL, Spencer FC, Hofstetter SR, et 01. The management of juxtahepatic
venous injuries without an atriocaval shunt: preliminary clinical observations.
Surgery 1986;99:569-75.
193. Yellin AE, Chaffee CB, Donovan AJ. Vascular isolation in treatment of
juxtahepatic venous injuries. Arch Surg 1971;102:566-73.
194. Edwards MJ, Bentley FR. Major hepatic resection under total vascular exclusion
with extracorporeal venovenous bypass. Am Surg 1994;60:231-3.
Curr Probl Surg, August 1996 693
195. Huguet C, Addario-Chieco P, Gavelli A, et 01. Technique of hepatic vascular
exclusion for extensive liver resection. Am J Surg 1992;163:602-5.
196. Launois B, De Chateaubriant P, Rosat P, et 01. Repair of suprahepatic caval
lesions under extracorporeal circulation in major liver trauma. J Trauma
1989;29:127-8.
197. Bourque MD, Spigland N, Bensoussan AL, et 01. Isolated completed transection
of the common bile duct due to blunt trauma in a child, and review of the
literature. J Pediatr Surg 1989;24: 1068-70.
198. Blunt TJ, Weimar R, Malone JM. Porta hepatis disruption from blunt trauma.
Am Surg 1990;56:695-6.
199. Dawson DL, Johansen KH, Jurkovich GJ. Injuries to the portal tria.d. Am J
Surg 1991; 161 :545-5l.
200. Jurkovich G, Hoyt D, Moore F, et 01. Portal triad injuries. J Trauma 1995;39:
426-34.
201. Yokota J, Sugimoto T. Clinical significance of periportal tracking on computed
tomographic scan in patients with blunt liver trauma. Am J Surg
1994;168:247-50.
202. Williams LN, Vu LH, Bragg W. Portal vein injuries: case report and review of
operative treatment options. J Tenn Med Assoc 1989;Oct:525-6.
203. Ivatury RR, Nallathambi M, Lankin DH, et 01. Portal vein injuries: noninvasive
follow-up of venorrhaphy. Ann Surg 1987;206: 733-7.
204. Pachter HL, Drager S, Godfrey N, et al. Traumatic injuries to the portal vein:
the role of acute ligation. Ann Surg 1979;189:383-5.
205. Stone HH, Fabian TC, Turkleson ML. Wounds of the portal venous system.
World J Surg 1982;6:335-41.
206. Lucas CE, Ledgerwood AM. Liver necrosis following hepatic artery transection
due to trauma. Arch Surg 1978;113:1107.
207. Mays ET. Observations in management affer hepatic artery ligation. Surg
Gynecol Obstet 1967;124:801-7.
208. Mays ET, Wheeler CS. Demonstration of collateral arterial flow after
interruption of hepatic a r t ~ r i e s in man. N Engl J Med 1974;290:993-6.
209. Mays El, Conti S, Fallahzadeh H, et 01. Hepatic artery ligation. Surgery
1979;86:536-43:
210. Mays ET. The hepatic artery. Surg Gynecol Obstet 1974;139:595-6.
211. Mays ET. Lobar dearterialization for exsanguinating wounds of the liver. J
Trauma 1972;12:397-407.
212. Dawson DL, Jurkovich GJ. Hepatic duct disruption from blunt abdominal
trauma: case report and literature review. J Trauma 1991 ;31: 1698702.
213. Cogbill lH, Moore EE, Feliciano DV, et 01. Conservative management of
duodenal trauma: a multicenter perspective. J Trauma 1990;30: 1469-
75.
214. Borlase Be, Moore EE, Moore FA. Mobilization of the spleen in splenic salvage.
Surg Gynecol Obstet 1988;16:279-80.
215. Raschbaum G, HarnarTJ, Canizaro Pc. The use of a stapler in splenic salvage
as an alternative to the sutured partial splenectomy or splenorrhaphy. Surg
Gynecol Obstet 1988; 166: 179-80.
216. Ravo B, Ger R. Splenic preservation with the use of a stapling instrument: a
preliminary communication. J Trauma 1988;28: 115-7.
694 Curr Probl Surg. August 1996
217. Uranus S, Kronberger L, Kraft-Kline J. Partial splenic resection using the TA-
Stapler. Am J Surg 1994; 168:49-53.
218. Delany HM, Rudavsky Al, Lan S. Preliminary clinical experience with the use
of absorbable mesh splenorrhaphy. J Trauma 1985;25:909-13.
219. Delany HM, Porreca F, Mitsudo S, et 01. Splenic capping: an experimental
study of a new technique for splenorrhaphy using woven polyglycolic acid
mesh. Ann Surg 1982;196:187-93.
220. Tribble CG, Joob AW, Barone Gw, et 01. A new technique for wrapping the
injuredspleen with polyglactin mesh. Am Surg 1987;53:661-3.
221. Pachter HL, Hofstetter SR, Spencer Fe. Evolving concepts in splenic surgery:
splenorrhaphy versus splenectomy and post-splenectomy drainage: experience
in 105 patients. Ann Surg 1981;194:262-9.
222. Rutherford EJ, Livengood J, Higginbotham M, et 01. Efficacy and safety of
pneumococcal revaccination after splenectomy for trauma. J Trauma
1995;39:448-52.
223. Chiang W. Isolated jejunal perforation from nonpenetrating abdominal
trauma. Am J Emerg Med 1993; 11 :473-5.
224. Sherck J, Oakes D. Intestinal injuries missed by computed tomography. J
Trauma 1990;30:1-7.
225. Wisner DH, Chun Y, Blaisdell FW. Blunt intestinal injury:keys to diagnosis and
management. Arch Surg 1990;125: 1319-23.
226. Hemming A, Davis N, Robins R. Surgical versus percutaneous drainage of
intra-abdominal abscesses. Am J Surg 1991; 161 :593-5.
227. Buechter KJ, Leonovicz 0, Hastings PR, et 01. Enterocutaneous fistulas following
laparotomy for trauma. Am Surg 1991 ;57:354-8.
228. Martin RR, Burch JM, Richardson R, et al. Outcome for delayed operation of
penetrating colon injuries.J Trauma 1991 ;31 :1591-5.
229. Thompson JS, Moore EE, Moore JB. Comparison of penetrating injuries of
the right and left colon. Ann Surg 1981;193:414-8.
230. Beall AC, Bricker DL, Alessi FJ, Whisennand HH, DeBakey ME. Surgical
considerations in the management of civilian colon injuries. Ann Surg
1971; 173:971-8.
231. LoCicero J, Tajima T, Drapanas T. A half-century of experience in the
management of colon injuries: changing concepts. J Trauma 1975;115:575-9.
232. Stone HH, Fabian Te. Management of perforating colon trauma. Ann Surg
1979; 190:430-6.
233.Burch JM, Brock JC, Gevirtzman L, et 01. The injured colon. Ann Surg
1986;203:701-11.
234. Nallathambi MN, Ivatury RR, Shah PM, et 01. Penetrating right colon trauma.
Am Surg 1987;53:209-14.
235. George SJ, Fabian T, Mangiante E. Colon trauma: further support for primary
repair. Am J Surg 1988; 156: 16-20.
236. Nelken N, Lewis F. The influence of injury severity on complication rates after
primary closure or colostomy for penetrating colon trauma. Ann Surg
1989;209:439-47.
237. Frame SB, Redgeway CA, Rice JC, et 01. Penetrating injuries to the colon:
analysis by anatomic region of injury. South Med J 1989;82:1099-102.
238. Levison MA, Thomas DO, Wiencek RG, et a!' Management of the injured
Curr Probl Surg, August 1996 695
colon: evolving practice at an urban trauma center. J Trauma 1990;30:247-53.
239. Chappuis C, Frey D, Dietzen C, Panetta T, Buechter K, Cohn IJ. Management
of penetrating colon injuries: a prospective randomized trial. Ann Surg
1991;213:492-7.
240. Bugis Sp' Blair Np, lelwin ER. Management of blunt and penetrating colon
injuries. Am J Surg 1992; 163:547-50.
241. Sasaki lS, Mittal Y, Allaben RD. Primary repair of colon injuries: a retrospective
analysis. Am Surg 1994;60:522-7.
242. Stewart RM, Fabian TC, Croce MA. Is resection with primary anastomosis
following destructive colon wounds always safe? Am J Surg 1994;168:316-9.
243. Levine H, Simon RJ, Smith TR, Ivatury R, Stahl W Guaiac testing in the diagnosis
of rectal trauma: what is its value? J Trauma 1992;32:210-2.
244. Thomas DD, Levison MA, Dykstra BJ, Bender JS. Management of rectal injuries:
dogma versus practice. Am Surg 1990;56:507-10.
245. Mangiante EC, Graham AD, Fabian TC. Rectal gunshot wounds. Am Surg
1986;52:37-40.
246. levy RD, Strauss P, Aladgem D, Degiannis E, 'Bofford KD, Saadia R.
Extraperitoneal rectal gunshot injuries. J Trauma 1995;38:273-7.
247. Tuggle D, Huber PJ. Management of rectal trauma. Am J Surg 1984;148:806.8.
248. Shannon FL, Moore EE, Moore FA, et 01. Value of distal colon washout in
civilian rectal trauma-reducing gut bacterial translocation. J Trauma
1988;28:989-94.
249. Kudsk KA, McQueen MA, Voeller GR, Fox MA, Mangiante EC Jr, Fabian TC.
Management of complex perineal soft-tissue injuries. J Trauma 1990;30: 1155-9.
250. Yajko RD, Seydel F, Trimble C. Rupture of the stomach from blunt abdominal
trauma. J Trauma 1975;15:177-83.
251. Brunsting LA, Morten JH. Gastric rupture from blunt abdominal trauma. J
Trauma 1987;27:887-90.
252. Durham RM, Olsen S, Weigelt JA. Penetrating injuries to- the stomach. Surg
Gynecol Obstet 1991;172:298-302.
253. Lang EK. Intra-abdominal and retroperitoneal organ injuries diagnosed on
dynamic c o m p u t e ~ tomograms obtained for assessment of renal trauma. J
Trauma 1990;30: 1161-8.
254. Feliciano DY, Burch JM, Graham JM. Abdominal vascular injury. In: Mattox
KL, Moore EE, Feliciano DY, editors. Trauma. Norwalk: Appleton & lange,
1988:519-36.
255. Holcroft Jw, Trunkey DD, Minagi H, et 01. Renal trauma and retroperitoneal
hematomas: indications for exploration. J Trauma 1975;15: 1045-52.
256. Shapiro MJ, Wolverson MK. Perforation of the retroperitoneal sigmoid colon
secondary to fracture-dislocation of the left sacroiliac joint: case report. J
Trauma 1989;29:694-6.
257. McAninch JW, Carroll PR, Armenakas NA, et 01. Renal gunshot wounds:
methods of salvage and reconstruction. J Trauma 1993;36: 179-284.
258. Flint LM, McCoy M, Richardson JD, et 01. Duodenal injury: analysis of common
misconceptions in diagnosis and treatment. Ann Surg 1980;191:697-702.
259. Phillips TF, Brotman S, Cleveland S, et 01. Perforating injuries of the small
bowel from blunt abdominal trauma. Ann Emerg Med 1983;12:75-9.
260. Weigelt JA. Duodenal injuries. Surg Clin North Am 1990;70:529-39.
696 Curr Probl Surg, August 1996
261. Shorr RM, Greaney GC, Donovan AJ. Iniuries of the duodenum. Am J Surg
1987;154:93-8.
262. Fischer Rp, Miller-Crochett P, Reed RL. Gastrointestinal disruption: the hazard
of nonoperative management in adults with blunt abdominal injury. J Trauma
1988;28: 1445-9.
263. Fabian TC, Mangiante EC, Millis M. Duodenal rupture due to blunt trauma:
a problem in diagnosis. South Med J 1984;77: 1078-82.
264. Snyder WH 3d, Weigelt JA, Watkins WL, et 01. The surgical management of
duodenal trauma: precepts based on a review of 247 cases. Arch Surg
1980;115:422-9.
265. Corley RD, Norcross WJ, Shoemaker WC. Traumatic iniuries to the duodenum:
a report of 98 patients. Ann Surg 1975; 181 :92-8.
266. Kunin JR, Korobkin M, Ellis JH, et al. Duodenal injuries caused by blunt
abdominal trauma: value of CT in differentiating perforation from hematoma.
AJR Am J Roentgenol 1993;160:1221-3.
267. Mcinnis WD, Aust JB, Cruz AB, et al. Traumatic injuries of the duodenum: a
comparison of primary closure and the jejunal patch. J Trauma 1975; 15:847-58.
268. Montgomery CE 2d, Frame SB, Enderson BL. Blunt duodenal trauma. J Tenn
Med Assoc 1993;86:303-5.
269. Stone HH, Fabian Te. Management of duodenal wounds. J Trauma
1979;19:334-9.
270. Ivatury RR, Nallathambi M, Gaudino J, Rohman M, Stahl WM. Penetrating
duodenal injuries: analysis of 100 consecutive cases. Ann Surg 1985;202: 153-8.
271. Hasson JE, Stern D, Moss GS. Penetrating duodenal trauma. J Trauma
1984;24:471-4.
272. Ivatury RR, Nallathambi M, Guadino J, et al. Penetrating duodenal injuries:
analysis of 100 consecutive cases. Ann Surg 1985;202: 153-8.
273. Ivatury RR, Guadino J, Ascer E, et 01. Treatment of penetrating duodenal
injuries: primary repair vs repair with decompressive ente'rostomy/ serosal
patch. J Trauma 1985;25:337-41.
273a. Berne CJ, Donovan AJ, White EJ, et al. Duodenal "diverticulization" for
duodenal and pancreatic inju'ry. Am J Surg 1974;127:503-7.
274. Vaughan GD 3d, Fraiier OH, Graham DY, et al. The use of pyloric exclusion
in the management of severe duodenal injuries. Am J Surg 1977;134:785-90.
275. Berg A. Duodenal fistula: its treatment by gastrojejunostomy and pyloric
occlusion. Ann Surg 1907;45:721-9.
276. Feliciano DV, Martin TD, Cruse PA. Management of combined pancreato-
duodenal injuries. Ann Surg 1987;205:673-80.
277. Martin TD, Feliciano DV, Mattox KL, et al. Severe duodenal injuries: treatment
with pyloric exclusion and gastrojejunostomy. Arch Surg 1983;118:631-5.
278. Buck JR, Sorensen VJ, Fath JJ, et al. Severe pancreato-duodenal injuries:
the effectiveness of pyloric exclusion with vagotomy. Am Surg
1992;58:557-61.
279. DeSantis M, Devereaux DF, Thompson D. Pyloric exclusion: suture material of
choice. Am Surg 1987;53:711-4.
280. Kudsk KA, Croce MA, Fabian TC, et 01. Enteral versus parenteral feeding:
effects on septic morbidity after blunt and penetrating abdominal trauma.
Ann Surg 1992;215:503-11.
Curr Probl Surg, August 1996 697
281. Smego DR, Richardson JD, Flint LM. Determinants of outcome in pancreatic
trauma. J Trauma 1985;25:771-6.
282. Ivatury RR, Nallathambi M, Roo P, 'et al. Penetrating pancreatic injuries. Am
Surg 1990;56:90-5.
283. Jones RC. Management of pancreatic trauma. Am J Surg 1985;150:698-704.
284. Berni GA, Bandyk OF, Oreskovich MR, et 01. Role of intraoperative
pancreatography in patients with injury to the pancreas. Am J Surg
1982; 143:602-5.
285. lane MJ, Mindelun RE, Sandhu JS, et 01. CT diagnosis of blunt pancreatic
trauma: importance of detecting fluid between the pancreas and the splenic
vein. AJR Am J Roentgenol 1994;163:833-5.
286. Cook DE, Walsh Jw, Vick CW et 01. Upper abdominal trauma: pitfalls in CT
diagnosis. Radiology 1986; 159:65-9.
287. Jeffrey RB, Federle Mp, Cross RA. Computed tomography of pancreatic trauma.
Radiology 1983;147:491-4.
288. Whitwell AE, Gomez GA, Byers P, et 01. Blunt pancreatic trauma: prospective
evaluation of early endoscopic retrograde pancreatography. South Med J
1989;82:586-91.
289. Pachter HL, Hofstetter SR, Liang HG, et al. Traumatic injuries to the pancreas:
the role of distal pancreatectomy with splenic preservation. J Trauma
1989;29:1352-5.
290. Graham JM, Mattox KL, Jordan GL. Traumatic injuries of the pancreas. Am J
Surg 1978;136:744-8.
291. Cogbill TH, Moore EE, Kashuk JL. Changing trends in the management of
pancreatic trauma. Arch Surg 1982; 117:722-8.
292. Oreskovich MR, Carrico CJ. Pancreaticoduodenectomy for trauma: a viable
option? Am J Surg 1984;47:618-23.
293. Heimensohn DA, Canol OF, McCarthy MC, et al. The role of pancreatico-
duodenectomy in the management of traumatic injuries.to the pancreas and
duodenum. Am Surg 1990;56:511-4.
294. Mansour MA, Moore JB, Moore EE, et al. Conservative management of
combined pancreatoduodenal injuries. Am J Surg 1989;158:531-5.
295. Eastlick L, Fogler RJ, Shaftan Gw. Pancreaticoduodenectomy for trauma:
delayed reconstruction: a case report. J Trauma 1990;30:5035.
296. Buchler M, Freiss H, Klmepa I, et al. Role of octreotide in the prevention of
postoperative complications following pancreatic resection. Am J Surg
1992;163: 125-3l.
297. Cass AS, Bubrick M,'Luxenberg M, et al. Renal trauma found during
laparotomy for intra-abdominal injury. J Trauma 1985;25:997-1000.
298. Carroll PR, McAninch Jw. Operative indications in penetrating renal trauma.
J Trauma 1985;25:587-93.
299. Corriere IN, McAndrew JO, Benson GS. Intraoperative decision-making in
renal trauma surgery. J Trauma 1991 ;31: 1390-2.
300. Carroll PR, Klosterman PW, McAninch JW. Surgical management of renal
trauma: analysis of risk factors, technique, and outcomes. J Trauma
1988;28: 1071-7.
301. McAninch JW, Carroll PRo Renal trauma: kidney preservation through improved
vascular control: a refined approach. J Trauma 1982;22:285-90.
698 Curr Probl Surg, August 1996
302. McAninch Jw. Genitourinary trauma. In: Moore EE, Mattox KL, Feliciano Ov,
editors. Trauma. Norwalk: Appleton & Lange, 1991 :571-86.
303. Spirnak Jp, Persky L, Resnick MI. The management of civilian ureteral gunshot
wounds: a review of 8 patients. J Urol 1985;134: 733-6.
304. Holden S, Hicks CC, O'Brien Op' et 01. Gunshot wounds of the ureter: a 15
year review of 63 consecutive cases. J Urol 1976;116:562-4.
305. Walker JA. Injuries of the ureter due to external violence. J Uro11969; 102:410-3.
306. Fisher 5, Young OA, Malin JM, et 01. Ureteral gunshot wounds. J Urol
1972; 108:2;38-9.
307. Campbell EW, Filderman PS, Jacobs Sc. Ureteral injury due to blunt and
penetrating trauma. Urology 1992;40:216-20.
308. Presti JC, Carroll PR, McAninch JW. Ureteral and renal pelvic injuries
from external trauma: diagnosis and management. J Trauma
1989;29:370-4.
309. Brandes SB, Chelsky MJ, Buckman RF, et a!. Ureteral injuries from penetrating
trauma. J Trauma 1994;36:766-9.
310. Cass AS. Ureteral contusion with gunshot wounds. J Trauma 1984;24:59-60.
311. Toporoff S, Scalfani 5, Scalea T, et a!. Percutaneous antegrade ureteral stenting
as an adjunct for treatment of complicated ureteral injuries. J Trauma
1992;32:534-8.
312. Rober PE, Smith JB, Pierce JM, et a!. Gunshot injuries of the ureter. J Trauma
1990;30:83-6.
313. Cass AS, Luxenberg M. Features of 164 bladder ruptures. J Urol
1987;138:743-5.
314. Wolk OJ, Sandler CM, Corriere IN Jr. Extraperitoneal bladder rupture without
pelvic fracture. J Urol 1985;132:1199-201.
315. Carroll PR, McAnninch Jw. Major bladder trauma: mechanisms of injury and
a unified method of diagnosis and repair. J Urol 1984;132:254-7.
316. Rehm CG, Mure AJ, O'Malley KF, et 01. Blunt traumatic bladder rupture: the
role of cystogram. Ann Emerg Med 1991 ;20:845-7.
317. Mee SL, McAnninch Jw, Federle. MP. Computerized tomography in bladder
rupture: diagnostic limitations. J Urol 1987;137:207-9.
318. Cass AS. False negative retrograde cystography with bladder rupture owing
to external trauma. J Trauma 1984;24: 168-9.
319. Kotkin L, Koch MO. Morbidity associated with nonoperative management of
extraperitoneal bladder injuries. J Trauma 1995;38:895-8.
320. Fallon B, Wendt JC, Hawtrey CEo Urology injury and assessment in patients
with fractured pelvis. J Urol 1984; 131 :712-4.
321. Burch JM, Richardson RJ, Martin RR, Mattox KL. Penetrating iliac vascular
injuries: recent experience with 233 consecutive patients. J Trauma
1990;30: 1450-9.
322. Wiencek RG, Wilson RF. Injuries to the abdominal vascular system: how much
does aggressive resuscitation and prelaparotomy thoracotmy really help?
Surgery 1987;102:731-6.
323. Lucas AE, Richardson JO, Flint LM, et 01. Traumatic injury of the proximal
superior mesenteric artery. Ann Surg 1981;193:30-4.
324. Millikan JS, Moore EE. Critical factors in determining mortality from abdominal
aortic trauma. Surg Gynecol Obstet 1985; 160:313-6.
Curr Probl Surg. August 1996 699
325. Wasserberger J, Ordog GJ, Dang C, et 01. Emergency department
thoracotomy. Emerg Med Clin North Am 1989;7:103-15.
326. Low RB. Preliminary report on the use of the Percluder occluding aortic balloon
in human beings. Ann Emerg Med 1986;15: 1466-9.
327. Shah OM, Leather Rp, Carson JD, et 01. PTFE grafts in rapid reconstruction of
acute contaminated peripheral vascular injuries. Am J Surg 1984;148:229-33.
328. Bricker DL, Beall AC, DeBakey ME. The differential response of infection of
autogenous vein versus Dacron arterial prosthesis. Chest 1970;58:566-70.
329. Reisman JD, Morgan AS. Analysis of 46 intra-abdominal aortic injuries from
blunt trauma: case reports and literature review. J Trauma 1990;30: 1294-7.
330. Klein SR, Baumgartner FJ, Bongard FS. Contemporary management strategy
for major inferior vena caval injuries. J Trauma 1994;37:35-42.
331. Pasch AR, Bishara RA, Schuler JJ, et 01. Results of venous reconstruction after
civilian vascular trauma. Arch Surg 1986;121 :607-1l.
332. Low RB, Schmidt CS, Wilder RJ, et 01. Control of intra-abdominal hemorrhage:
a comparison of methods. J Oklo State Med Assoc 1984;77:356-60.
333. Accola KD, Feliciano DV, Mattox KL. Management of iniuries to the superior
mesenteric artery. J Trauma 1986;26:313-9.
334. Feliciano DV, Maltox KL, Graham JM, et 01. Five-year experience with PTFE
grafts in vascular wounds. J Trauma 1985;25:71-82.
335. Duncan TO, Phillips TF, Scalea TM. Management of transpelvic gunshot
wounds. J Trauma 1989;29: 1335-40.
336. Rich NM, Hughes CW, Baugh JH. Management of venous injuries. Ann Surg
1970i171 :724-30.
337. Yelon JA, Scalea TM. Venous injuries of the lower extremities and pelvis: repair
versus ligation. J Trauma 1992;33:532-6.
338. Machado MAC, Ikejiri CI, Borrelli M, et 01. An unusual case of four iliac veins
injured by gunshot: case report and review of the literature. J Trauma
1994;36:442-3.
339. Shakleford RT, Zuidema GO. Surgery of the alimentary tract. 2nd ed.
Philadelphia: WB Saunders Company, 1982.
340. Collins PS, Golo:covsky M, Salander JM, et 01. Intra-abdominal vascular injury
secondary to penetrating trauma. J Trauma 1988;28:S165-70.
341. Donahue TK, Strauch GO. Ligation as definitive management of injury to the
superior mesenteric vein. J Trauma 1988i28:541-3.
700 Curr Probl Surg, August 1996
Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Lower Extremity Stretching and Warm Up ExercisesDocumento7 páginasLower Extremity Stretching and Warm Up ExercisesTenny TAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Taylor 168 User ManualDocumento47 páginasTaylor 168 User ManualFama Banks EdrevopmacAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Distal Radius Fractures (Broken Wrist) - OrthoInfo - AAOSDocumento4 páginasDistal Radius Fractures (Broken Wrist) - OrthoInfo - AAOSmuhammad iqbal mahfuzhAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Toolbox Talk 4 Manual HandlingDocumento2 páginasToolbox Talk 4 Manual HandlingSajid HussainAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Forensic Medicine Multiple Choice Question BankDocumento20 páginasForensic Medicine Multiple Choice Question BankGIST (Gujarat Institute of Science & Technology)54% (13)
- 45 Web BK, Karate JutsuDocumento71 páginas45 Web BK, Karate Jutsudiamond68100% (5)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Locked in SyndromeDocumento52 páginasLocked in SyndromeFarrukh Ali KhanAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Husqvarna 345 ManualDocumento36 páginasHusqvarna 345 ManualTom FergusonAinda não há avaliações
- Gujarat High Court Ordered Probe in Custodial Death Case - Shwetang Patel Murder Case - Patidar Agitation - Police Atrocity - (Read The Order)Documento9 páginasGujarat High Court Ordered Probe in Custodial Death Case - Shwetang Patel Murder Case - Patidar Agitation - Police Atrocity - (Read The Order)Manan BhattAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- EELPWAEN0413 Electrical Safety Handbook 20131Documento72 páginasEELPWAEN0413 Electrical Safety Handbook 20131abdul samadAinda não há avaliações
- Penis Sonography. A Pictorial Review: Poster No.: Congress: Type: AuthorsDocumento35 páginasPenis Sonography. A Pictorial Review: Poster No.: Congress: Type: AuthorsOky Sutarto PutraAinda não há avaliações
- Topic Sentences and Supporting DetailsDocumento2 páginasTopic Sentences and Supporting DetailsBuhle JoyAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Gait AssessmentDocumento71 páginasGait Assessmentelenita702100% (2)
- AnatomyDocumento42 páginasAnatomyMohamed Rikarz Ahamed RikarzAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- p1k Pde2577tcuk 052009 PDFDocumento20 páginasp1k Pde2577tcuk 052009 PDFwalid8311Ainda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Prisnr of The Daleks - TBaxendaleDocumento279 páginasPrisnr of The Daleks - TBaxendaleRachelle McDonald100% (1)
- Fixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFDocumento4 páginasFixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFThomas BowersAinda não há avaliações
- Osteogenesis Imperfecta Power PointDocumento29 páginasOsteogenesis Imperfecta Power PointJonathan Jeffry Pratama100% (1)
- Dog AdoptionDocumento3 páginasDog Adoptionkjh267267Ainda não há avaliações
- Retrograde Urethrography Examination in Penile Fracture: Case ReportDocumento3 páginasRetrograde Urethrography Examination in Penile Fracture: Case Reportsofia ayu lestariAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Vanishing Throne: Book Two of The Falconer Trilogy (Excerpt)Documento24 páginasThe Vanishing Throne: Book Two of The Falconer Trilogy (Excerpt)ChronicleBooks0% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- FlipCutter A Pin That Changes Arthroscopic Tunnel Drilling Forever...Documento12 páginasFlipCutter A Pin That Changes Arthroscopic Tunnel Drilling Forever...andrelbportoAinda não há avaliações
- Fase de Campo Rehabilitacion de AclDocumento11 páginasFase de Campo Rehabilitacion de AclSergio Garcia AngelAinda não há avaliações
- Merrell BarefootTrainingPlanDocumento20 páginasMerrell BarefootTrainingPlanSophene MarshallAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Kiteboarding Exercises Complete Training Guide V2Documento19 páginasKiteboarding Exercises Complete Training Guide V2notrealcriticalAinda não há avaliações
- Cove Point LNG Terminal Expansion Project Risk StudyDocumento77 páginasCove Point LNG Terminal Expansion Project Risk StudyjomafebaAinda não há avaliações
- Dental Graft ProceduresDocumento43 páginasDental Graft ProcedureskishanAinda não há avaliações
- WYFL Physical FormDocumento2 páginasWYFL Physical FormAshley Nabors TalbotAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Special Arthrology of The ForelimbDocumento37 páginasSpecial Arthrology of The ForelimbTheBoss 20Ainda não há avaliações
- Bone Fracture Concept MapDocumento1 páginaBone Fracture Concept MapJette Charmae OlboAinda não há avaliações