Você também pode gostar
- Long Case Surgery Exam QuestionDocumento25 páginasLong Case Surgery Exam Questionwhee182Ainda não há avaliações
- USA Physician DirectoryDocumento265 páginasUSA Physician Directorysonukarma321Ainda não há avaliações
- Sept Recall PlabDocumento19 páginasSept Recall PlabDr-Jahanzaib GondalAinda não há avaliações
- Friends Ccs CasesDocumento23 páginasFriends Ccs Casesvivekmo100% (2)
- 1700 Files Explained by DRDocumento224 páginas1700 Files Explained by DRSana NabeelAinda não há avaliações
- Med and Surg RecallDocumento15 páginasMed and Surg RecallSherif ElbadrawyAinda não há avaliações
- Plab Big Mock October 2023Documento89 páginasPlab Big Mock October 2023MASONEJIAinda não há avaliações
- September 2023 Part 3Documento238 páginasSeptember 2023 Part 3Fatinha Lucia FC Pinto100% (1)
- MasterDocumento22 páginasMasterAppu ayyala100% (1)
- AMC-2007 Clinical Examination RecallsDocumento156 páginasAMC-2007 Clinical Examination Recallsbreezingthru100% (1)
- March 2021 USMLE Recalls Actual Exam Questions: Click To Get MoreDocumento8 páginasMarch 2021 USMLE Recalls Actual Exam Questions: Click To Get MoreRushi Shah75% (4)
- OSCE Melb11Nov06Documento7 páginasOSCE Melb11Nov06janaka1022Ainda não há avaliações
- CK 9Documento11 páginasCK 9nreena aslamAinda não há avaliações
- M/DN MIS Intramedullary Femoral Fixation Surgical TechniqueDocumento32 páginasM/DN MIS Intramedullary Femoral Fixation Surgical TechniqueVamby SabidoAinda não há avaliações
- Examination: (Look, Listen, Feel !!!!)Documento13 páginasExamination: (Look, Listen, Feel !!!!)Sherif Elbadrawy100% (1)
- TSRA Review of Cardiothoracic PDFDocumento298 páginasTSRA Review of Cardiothoracic PDFvamshidhAinda não há avaliações
- 68 Important Scenarios For ST 5 PracticeDocumento20 páginas68 Important Scenarios For ST 5 PracticeSalem ELsayed Abdel AzizAinda não há avaliações
- Picu Case StudyDocumento3 páginasPicu Case Studyapi-455545776Ainda não há avaliações
- BrisDocumento9 páginasBrisYwagar YwagarAinda não há avaliações
- BrisDocumento9 páginasBrisYwagar YwagarAinda não há avaliações
- Case Clerking ApendicDocumento15 páginasCase Clerking ApendicMelvin Khung100% (1)
- AMC Clinical Recall 138, Sum 16.2.13Documento15 páginasAMC Clinical Recall 138, Sum 16.2.13AMMARAAinda não há avaliações
- Paces Exam Cases 2nd Version PDFDocumento471 páginasPaces Exam Cases 2nd Version PDFMuntadher Kareem100% (1)
- Anesthesia For EntDocumento44 páginasAnesthesia For EntDrshoaib KhanAinda não há avaliações
- Day 13th October 2023 RecallDocumento12 páginasDay 13th October 2023 RecallprathibaAinda não há avaliações
- May 31Documento6 páginasMay 31Sherif ElbadrawyAinda não há avaliações
- PE Recall AMC ExamDocumento9 páginasPE Recall AMC ExamSherif Elbadrawy100% (1)
- MCQ2 QuestionDocumento100 páginasMCQ2 Question9hjk6wpxyfAinda não há avaliações
- Medicine Long CaseDocumento26 páginasMedicine Long Casewhee182Ainda não há avaliações
- December 2008final FRCA VivaDocumento43 páginasDecember 2008final FRCA Vivajahangirealam100% (2)
- GPDocumento3 páginasGPYwagar YwagarAinda não há avaliações
- Powder PharmaceuticsDocumento58 páginasPowder PharmaceuticskishnapraveenAinda não há avaliações
- Feb 2023Documento11 páginasFeb 2023Parsaant SinghAinda não há avaliações
- Sydney 2008 MarchDocumento8 páginasSydney 2008 MarchYwagar YwagarAinda não há avaliações
- Long Case Mmbs 06 11Documento110 páginasLong Case Mmbs 06 11whee182Ainda não há avaliações
- Recall Brisbane February 2008Documento7 páginasRecall Brisbane February 2008Ywagar YwagarAinda não há avaliações
- Meniere's Disease - Case StudyDocumento3 páginasMeniere's Disease - Case StudyZORANASNAinda não há avaliações
- MED4000Documento28 páginasMED4000eunice_lee_48Ainda não há avaliações
- April 21st Recalls With Approaches and AMC Feedback Recollected From Several Posted MaterialsDocumento6 páginasApril 21st Recalls With Approaches and AMC Feedback Recollected From Several Posted MaterialsqurbanAinda não há avaliações
- Next Step Advanced Medical Coding and Auditing 2017 2018 Edition 1st Edition Buck Test BankDocumento25 páginasNext Step Advanced Medical Coding and Auditing 2017 2018 Edition 1st Edition Buck Test BankAllisonPowersrjqo100% (49)
- Attending Osteomyelitis ModuleDocumento9 páginasAttending Osteomyelitis ModuleMrLarry DolorAinda não há avaliações
- 9 RFTCXDocumento24 páginas9 RFTCXpotnic44Ainda não há avaliações
- 1 A 2018 March RecallsDocumento16 páginas1 A 2018 March RecallsqurbanAinda não há avaliações
- Brisbane February 2008: Peanut Induced AnaphylaxisDocumento7 páginasBrisbane February 2008: Peanut Induced AnaphylaxisYwagar YwagarAinda não há avaliações
- HHD 9 Accident EmergencyDocumento6 páginasHHD 9 Accident Emergencymusy9999Ainda não há avaliações
- Mel 2005 Jun 4 RetestDocumento5 páginasMel 2005 Jun 4 RetestZweAinda não há avaliações
- Clinical Signs in PaediatricsDocumento24 páginasClinical Signs in PaediatricsNURUL AFZA MOHD SHAMSUL KAMALAinda não há avaliações
- Case StudyDocumento3 páginasCase StudyAmila RahmahAinda não há avaliações
- Pathology I Review 10Documento30 páginasPathology I Review 10i_areinamoAinda não há avaliações
- "Don't Take My Breath Away" A Case Presentation On Pneumocystis PneumoniaDocumento20 páginas"Don't Take My Breath Away" A Case Presentation On Pneumocystis PneumoniaNikki DiocampoAinda não há avaliações
- Dha GP 2 July 2018Documento8 páginasDha GP 2 July 2018Nilufar EasminAinda não há avaliações
- 2019 IteDocumento188 páginas2019 IteBHAinda não há avaliações
- Clerk GCPDocumento19 páginasClerk GCPNikki DiocampoAinda não há avaliações
- MS Case PresDocumento33 páginasMS Case PresShaine_Thompso_6877Ainda não há avaliações
- Case Report Tuberculous Otitis MediaDocumento23 páginasCase Report Tuberculous Otitis MediahwelpAinda não há avaliações
- Home Assignment I - Adrian Crișan and Istrate Cristian (Series A, Group 4)Documento9 páginasHome Assignment I - Adrian Crișan and Istrate Cristian (Series A, Group 4)Istrate CristianAinda não há avaliações
- TCD Thyroid-6-1Documento72 páginasTCD Thyroid-6-1amrsameerAinda não há avaliações
- Melbourne 14 May 2005: Case 1: Rotator Cuff InjuryDocumento9 páginasMelbourne 14 May 2005: Case 1: Rotator Cuff InjuryZweAinda não há avaliações
- Contoh Soal MCQDocumento13 páginasContoh Soal MCQrororukmiAinda não há avaliações
- Abuajela Sreh - St5 Gastroenterology - Sheffield Teaching Hospitals 1 4 / 0 1 / 2 0 2 2Documento48 páginasAbuajela Sreh - St5 Gastroenterology - Sheffield Teaching Hospitals 1 4 / 0 1 / 2 0 2 2sryh2012Ainda não há avaliações
- Azazim 2012 PDFDocumento27 páginasAzazim 2012 PDFShowmik PaulAinda não há avaliações
- Thornton 2016Documento5 páginasThornton 2016AfdhalRuslanAinda não há avaliações
- Mitral Stenosis Case PresentationDocumento7 páginasMitral Stenosis Case PresentationOM BAWNEAinda não há avaliações
- Metabolic Disease Case Study Learning ActivityDocumento8 páginasMetabolic Disease Case Study Learning ActivityKhali Sciola0% (1)
- Nursing Management of A Patient With: HyperthyroidismDocumento31 páginasNursing Management of A Patient With: Hyperthyroidismember parkAinda não há avaliações
- Acute Hypotonia in An Infant (2017)Documento3 páginasAcute Hypotonia in An Infant (2017)nikos.alexandrAinda não há avaliações
- Walhalla Gold MineDocumento1 páginaWalhalla Gold MineYwagar YwagarAinda não há avaliações
- Clinical Tutorial 2008.11.05Documento31 páginasClinical Tutorial 2008.11.05Ywagar Ywagar100% (1)
- Sydney 2008 MarchDocumento8 páginasSydney 2008 MarchYwagar YwagarAinda não há avaliações
- Recall Brisbane February 2008Documento7 páginasRecall Brisbane February 2008Ywagar YwagarAinda não há avaliações
- Clinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeDocumento14 páginasClinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeYwagar YwagarAinda não há avaliações
- Adelaide, 5 April, 2008: PaediatricsDocumento17 páginasAdelaide, 5 April, 2008: PaediatricsYwagar YwagarAinda não há avaliações
- Brisbane July 2008 RecallDocumento11 páginasBrisbane July 2008 RecallYwagar YwagarAinda não há avaliações
- Draft May 08 WES ProgramDocumento2 páginasDraft May 08 WES ProgramYwagar YwagarAinda não há avaliações
- Adelaide 13th September 2008Documento16 páginasAdelaide 13th September 2008Ywagar YwagarAinda não há avaliações
- Adelaide, 5 April, 2008: PaediatricsDocumento17 páginasAdelaide, 5 April, 2008: PaediatricsYwagar YwagarAinda não há avaliações
- Melb RetestDocumento4 páginasMelb RetestYwagar YwagarAinda não há avaliações
- ACln2007!09!08MEL Retest Wd97Documento6 páginasACln2007!09!08MEL Retest Wd97Ywagar YwagarAinda não há avaliações
- Melbourne 2008 Nov 8Documento10 páginasMelbourne 2008 Nov 8Ywagar YwagarAinda não há avaliações
- Paediatrics:: Case 1nsionDocumento16 páginasPaediatrics:: Case 1nsionYwagar YwagarAinda não há avaliações
- Brisbane February 2008: Peanut Induced AnaphylaxisDocumento7 páginasBrisbane February 2008: Peanut Induced AnaphylaxisYwagar YwagarAinda não há avaliações
- Clinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeDocumento14 páginasClinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeYwagar YwagarAinda não há avaliações
- 15th March 2008 SydneyDocumento3 páginas15th March 2008 SydneyYwagar YwagarAinda não há avaliações
- Melbourne, 9 February 2008: AMC Feedback: Paranoid Schizophrenia (Relapse)Documento13 páginasMelbourne, 9 February 2008: AMC Feedback: Paranoid Schizophrenia (Relapse)Ywagar YwagarAinda não há avaliações
- 3rd May 2008 SydneyDocumento9 páginas3rd May 2008 SydneyYwagar YwagarAinda não há avaliações
- Grammar and VocabularyDocumento2 páginasGrammar and Vocabularythiên bình trầnAinda não há avaliações
- Andrew Eastman Resume 3Documento2 páginasAndrew Eastman Resume 3api-281509868Ainda não há avaliações
- 2012 West Central Ohio Medical Directory - Fall and WinterDocumento64 páginas2012 West Central Ohio Medical Directory - Fall and WinterThe Lima NewsAinda não há avaliações
- Katherine E. Paton Honored As 2018 Professional of The Year in Ocular OncologyDocumento2 páginasKatherine E. Paton Honored As 2018 Professional of The Year in Ocular OncologyPR.comAinda não há avaliações
- 2 1 Acute InflammationDocumento5 páginas2 1 Acute InflammationFaten AwadAinda não há avaliações
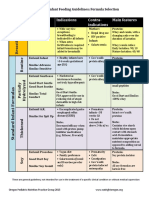
- Formula Selection OPNPGDocumento2 páginasFormula Selection OPNPGRina PratiwiAinda não há avaliações
- Failure Patterns of Different Bracket Systems and Their Influence On Treatment Duration - A Retrospective Cohort StudyDocumento10 páginasFailure Patterns of Different Bracket Systems and Their Influence On Treatment Duration - A Retrospective Cohort StudyHuma SaleemAinda não há avaliações
- Periodic Medical ExaminationDocumento4 páginasPeriodic Medical ExaminationAndreeaRedheadAinda não há avaliações
- Library GenesisDocumento10 páginasLibrary Genesismusic cisumAinda não há avaliações
- The DentistDocumento4 páginasThe DentistuvkiniAinda não há avaliações
- Academic Coach Resource List - Jan 2020Documento2 páginasAcademic Coach Resource List - Jan 2020OsamaAinda não há avaliações
- Evaluation of Primigravida in Labour Using Modified WHO Partograph: Comparative Study of 100 CasesDocumento6 páginasEvaluation of Primigravida in Labour Using Modified WHO Partograph: Comparative Study of 100 CasesShobhitAinda não há avaliações
- AprobacijaDocumento4 páginasAprobacijaMario Marco Del TintorettoAinda não há avaliações
- Anatomy of The KidneyDocumento13 páginasAnatomy of The KidneyChristi NaldoAinda não há avaliações
- Can Rotation PlanDocumento18 páginasCan Rotation PlanMadhuAinda não há avaliações
- Tu IomDocumento10 páginasTu Iomtsc madanpurAinda não há avaliações
- Guideline For Establishing Emergency Medical and Trauma CentersDocumento32 páginasGuideline For Establishing Emergency Medical and Trauma CentersHoussein YoussoufAinda não há avaliações
- ResumeDocumento2 páginasResumeJune TorrionAinda não há avaliações
- February April 2009 Part 2 FRCOphth Examination Final ReportDocumento20 páginasFebruary April 2009 Part 2 FRCOphth Examination Final Reportsafasayed0% (1)
- Managing Medical and Obstetric Emergencies and Trauma A Practical Approach 4Th Edition Rosamunde Burns Editor Full ChapterDocumento65 páginasManaging Medical and Obstetric Emergencies and Trauma A Practical Approach 4Th Edition Rosamunde Burns Editor Full Chaptersteven.webb781100% (4)
- Prevention and Management of Acute Kidney InjuryDocumento30 páginasPrevention and Management of Acute Kidney InjuryIren DawsonAinda não há avaliações
- Case Report: Aesthetic Depigmentation of Gingival Smoker's Melanosis Using Carbon Dioxide LasersDocumento6 páginasCase Report: Aesthetic Depigmentation of Gingival Smoker's Melanosis Using Carbon Dioxide LasersAsy-syifa Brillian AvicennaAinda não há avaliações
- Hospital Management TaskDocumento3 páginasHospital Management TaskJoecelyn AnastasiaAinda não há avaliações
- Mock CodeDocumento4 páginasMock CodeKrezielDulosEscobarAinda não há avaliações