Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- gtg60 Cervicalcerclage PDFDocumento21 páginasgtg60 Cervicalcerclage PDFLijoeliyas100% (1)
- Types of Sutures and Their IndicationsDocumento6 páginasTypes of Sutures and Their IndicationsAdina BurciuAinda não há avaliações
- Laser 1Documento22 páginasLaser 1Mantu KumarAinda não há avaliações
- Introducing Identity - SummaryDocumento4 páginasIntroducing Identity - SummarylkuasAinda não há avaliações
- Problem-Solution Essay Final DraftDocumento4 páginasProblem-Solution Essay Final Draftapi-490864786Ainda não há avaliações
- Incremental Analysis 2Documento12 páginasIncremental Analysis 2enter_sas100% (1)
- Live Leak - SSC CGL Tier II English Model Question Paper (Based On Predicted Pattern 2016)Documento44 páginasLive Leak - SSC CGL Tier II English Model Question Paper (Based On Predicted Pattern 2016)Testbook BlogAinda não há avaliações
- Ritual 2 Turning Attraction Into LoveDocumento2 páginasRitual 2 Turning Attraction Into Lovekrlup0% (1)
- Reaction PaperDocumento3 páginasReaction PaperPatrick Ramos80% (15)
- 1Documento13 páginas1Victor AntoAinda não há avaliações
- Edu 536 - Task A2 - pld5Documento3 páginasEdu 536 - Task A2 - pld5api-281740174Ainda não há avaliações
- Lara CroftDocumento58 páginasLara CroftMarinko Tikvicki67% (3)
- Happiness Portrayal and Level of Self-Efficacy Among Public Elementary School Heads in A DivisionDocumento13 páginasHappiness Portrayal and Level of Self-Efficacy Among Public Elementary School Heads in A DivisionPsychology and Education: A Multidisciplinary JournalAinda não há avaliações
- Calculation of % Slip in Mill During Rolling by Ajmal (10.09.2014)Documento15 páginasCalculation of % Slip in Mill During Rolling by Ajmal (10.09.2014)Rakesh Karan SinghAinda não há avaliações
- Basic Statistics For Business AnalyticsDocumento15 páginasBasic Statistics For Business AnalyticsNeil Churchill AniñonAinda não há avaliações
- Caucasus University Caucasus Doctoral School SyllabusDocumento8 páginasCaucasus University Caucasus Doctoral School SyllabusSimonAinda não há avaliações
- Mahabharata Reader Volume 1 - 20062023 - Free SampleDocumento107 páginasMahabharata Reader Volume 1 - 20062023 - Free SampleDileep GautamAinda não há avaliações
- Shreya Keshari PDFDocumento75 páginasShreya Keshari PDFANKIT SINGHAinda não há avaliações
- City Living: Centro de Lenguas ExtranjerasDocumento2 páginasCity Living: Centro de Lenguas Extranjerascolombia RodriguezAinda não há avaliações
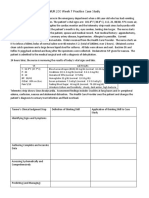
- NUR 200 Week 7 Practice Case StudyDocumento2 páginasNUR 200 Week 7 Practice Case StudyJB NicoleAinda não há avaliações
- When Karl Met Lollo The Origins and Consequences of Karl Barths Relationship With Charlotte Von KirschbaumDocumento19 páginasWhen Karl Met Lollo The Origins and Consequences of Karl Barths Relationship With Charlotte Von KirschbaumPsicoorientación FamiliarAinda não há avaliações
- SANCHEZ V DEMETRIOUDocumento3 páginasSANCHEZ V DEMETRIOUShenna SunicoAinda não há avaliações
- Gesture and Speech Andre Leroi-GourhanDocumento451 páginasGesture and Speech Andre Leroi-GourhanFerda Nur Demirci100% (2)
- Script For Demo TeachingDocumento9 páginasScript For Demo TeachingDindz SurioAinda não há avaliações
- CSWP Practice Test Book: Certified Solidworks ProfessionalsDocumento20 páginasCSWP Practice Test Book: Certified Solidworks ProfessionalsmohamedAinda não há avaliações
- Plate Tectonics QuizDocumento6 páginasPlate Tectonics QuizJordan Santos100% (1)
- Keir 1-2Documento3 páginasKeir 1-2Keir Joey Taleon CravajalAinda não há avaliações
- Engineering Academy: ESE Conventional Revision TEST - IDocumento8 páginasEngineering Academy: ESE Conventional Revision TEST - Ividya chakitwarAinda não há avaliações
- Pakistan's Professor Mafia - Pakistan - DAWNDocumento5 páginasPakistan's Professor Mafia - Pakistan - DAWNMuhammad Bilal A. RAinda não há avaliações
- Ulf Hannerz - Being There and ThereDocumento17 páginasUlf Hannerz - Being There and ThereThomás MeiraAinda não há avaliações