Você também pode gostar
- Pentra XLR Daily Guide PDFDocumento44 páginasPentra XLR Daily Guide PDFflorentyna78100% (3)
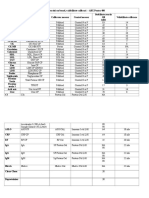
- Stabilitate OB Reactivi Si Valabilitate Calibrari P400Documento2 páginasStabilitate OB Reactivi Si Valabilitate Calibrari P400florentyna78Ainda não há avaliações
- Thursday, August 15, 2013 3:54 PM: Unfiled Notes Page 1Documento95 páginasThursday, August 15, 2013 3:54 PM: Unfiled Notes Page 1florentyna78Ainda não há avaliações
- Terapia LaserDocumento124 páginasTerapia Laserflorentyna78Ainda não há avaliações
- Anatomia VenelorDocumento4 páginasAnatomia Venelorflorentyna78Ainda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- MollyDocumento7 páginasMollyapi-534233456Ainda não há avaliações
- Top 50 Global Stem Cell InfluencersDocumento25 páginasTop 50 Global Stem Cell InfluencersranasoftAinda não há avaliações
- Physical Assessment SampleDocumento6 páginasPhysical Assessment Samplecarlylove33% (3)
- Advanced Trauma Life Support (Atls)Documento44 páginasAdvanced Trauma Life Support (Atls)Danar Syahrial PradhiptaAinda não há avaliações
- Oplan Kalusugan Sa DepEd SY 2019Documento4 páginasOplan Kalusugan Sa DepEd SY 2019Klaribelle Villaceran100% (1)
- ECAM2015 324369 PDFDocumento6 páginasECAM2015 324369 PDFLuiz Otavio CostaAinda não há avaliações
- ACETYLCYSTEINEDocumento2 páginasACETYLCYSTEINEAubrey Unique EvangelistaAinda não há avaliações
- Sex ManualDocumento14 páginasSex ManualCally LiueAinda não há avaliações
- Sitagliptin Slide Set Specialist - 1Documento31 páginasSitagliptin Slide Set Specialist - 1Fannia Setiani100% (1)
- CHF CSDocumento4 páginasCHF CSLaren CyrAinda não há avaliações
- Vital Signs Vital Signs: Importance: ImportanceDocumento6 páginasVital Signs Vital Signs: Importance: ImportanceTyron KristianAinda não há avaliações
- Legal MedicineDocumento7 páginasLegal Medicinecha chaAinda não há avaliações
- TLX Technique GuideDocumento28 páginasTLX Technique Guidejerry rice100% (2)
- S/N Description UnitDocumento16 páginasS/N Description UnitPeccamb SurgicalAinda não há avaliações
- A) Long-Term Follow-Up of Patients With Migrainous Infarction - Accepted and Final Publication From Elsevier1-s2.0-S030384671730344X-mainDocumento3 páginasA) Long-Term Follow-Up of Patients With Migrainous Infarction - Accepted and Final Publication From Elsevier1-s2.0-S030384671730344X-mainRodrigo Uribe PachecoAinda não há avaliações
- Pastel Green and Yellow Interior Designer Modern Resume 3Documento2 páginasPastel Green and Yellow Interior Designer Modern Resume 3api-482978808Ainda não há avaliações
- MycetomaDocumento26 páginasMycetomaTummalapalli Venkateswara RaoAinda não há avaliações
- Evidence-Based Care SheetDocumento6 páginasEvidence-Based Care SheetTITINAinda não há avaliações
- Jadwal Praktek Dokter Spesialis Baru 1akreditasi AllDocumento8 páginasJadwal Praktek Dokter Spesialis Baru 1akreditasi Alldonny suryaAinda não há avaliações
- Princples of Drug AdministrationDocumento90 páginasPrincples of Drug Administrationcoosa liquorsAinda não há avaliações
- Brain DeathDocumento24 páginasBrain DeathKawaljit KaurAinda não há avaliações
- Lefort FractureDocumento90 páginasLefort FractureRiya CorreaAinda não há avaliações
- Female Hot Spots Extragenital Erogenous Zones.4Documento8 páginasFemale Hot Spots Extragenital Erogenous Zones.4Shilpa VijeeshAinda não há avaliações
- Setup Rak ObatDocumento161 páginasSetup Rak Obatmuna barajaAinda não há avaliações
- Ilovepdf Merged PDFDocumento134 páginasIlovepdf Merged PDFhelalAinda não há avaliações
- Application Form: Institution Name Institution Location Degree Name From (MM/YY) To (MM/YY) Degree Received (Y/N)Documento6 páginasApplication Form: Institution Name Institution Location Degree Name From (MM/YY) To (MM/YY) Degree Received (Y/N)SalwiyadiAinda não há avaliações
- Electrical SafetyDocumento43 páginasElectrical SafetyVer BautistaAinda não há avaliações
- 2nd Grading Test Science 5Documento7 páginas2nd Grading Test Science 5LeonorBagnisonAinda não há avaliações
- Ast (Sgot) ColorDocumento2 páginasAst (Sgot) ColorShribagla MukhiAinda não há avaliações
- Parts of A Tracheostomy TubeDocumento3 páginasParts of A Tracheostomy TubeBal GieAinda não há avaliações