Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Cambridge Igcse Literature in English Teacher S Resource CD Rom Cambridge Education Cambridge U Samples PDFDocumento14 páginasCambridge Igcse Literature in English Teacher S Resource CD Rom Cambridge Education Cambridge U Samples PDFMorshedHumayunAinda não há avaliações
- Lesson Plan 1 (Types of Industries)Documento3 páginasLesson Plan 1 (Types of Industries)Chonie VillanuevaAinda não há avaliações
- Motor-Catalog English 2013 PDFDocumento80 páginasMotor-Catalog English 2013 PDFILham Dwi PutraAinda não há avaliações
- Rebrand and Relaunch Hydrox CookiesDocumento9 páginasRebrand and Relaunch Hydrox CookiesAruba KhanAinda não há avaliações
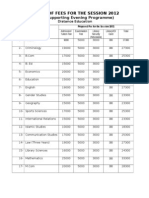
- Detail of Fees For The Session 2012 FinalDocumento3 páginasDetail of Fees For The Session 2012 FinalcfmbaimsAinda não há avaliações
- 2010-11 Annual ReportDG CEMENTDocumento115 páginas2010-11 Annual ReportDG CEMENTBashar AliAinda não há avaliações
- CapitalDocumento25 páginasCapitalcfmbaimsAinda não há avaliações
- Study of Ibrahim Group of CompaniesDocumento29 páginasStudy of Ibrahim Group of CompaniescfmbaimsAinda não há avaliações
- Internship ReportDocumento64 páginasInternship ReportIram Aziz ShahAinda não há avaliações
- XXXXXDocumento38 páginasXXXXXGarrett HughesAinda não há avaliações
- Am No. 98-5-01-SC, Nov 9 1998 in Re Hon Mateo ValenzuelaDocumento9 páginasAm No. 98-5-01-SC, Nov 9 1998 in Re Hon Mateo Valenzuelaian clark MarinduqueAinda não há avaliações
- Wavelets and Signal ProcessingDocumento193 páginasWavelets and Signal ProcessingAlbeno Saleh AhmadAinda não há avaliações
- Daftar PustakaDocumento2 páginasDaftar PustakaBang UsopAinda não há avaliações
- Holly Rayner - The Prince S Real Fake BrideDocumento239 páginasHolly Rayner - The Prince S Real Fake BrideAbbyMac BAinda não há avaliações
- M.Vikram: Department of Electronics and Communication EngineeringDocumento26 páginasM.Vikram: Department of Electronics and Communication EngineeringSyed AmaanAinda não há avaliações
- Note 1-Estate Under AdministrationDocumento8 páginasNote 1-Estate Under AdministrationNur Dina AbsbAinda não há avaliações
- Ad3na0ab (COMBI NACCO-ing)Documento30 páginasAd3na0ab (COMBI NACCO-ing)Kaique MelloAinda não há avaliações
- Real Estate in IndiaDocumento6 páginasReal Estate in IndiaVikrant KarhadkarAinda não há avaliações
- 002 SM MP4054Documento2.009 páginas002 SM MP4054tranquangthuanAinda não há avaliações
- Take The MMPI Test Online For Free: Hypnosis Articles and InformationDocumento14 páginasTake The MMPI Test Online For Free: Hypnosis Articles and InformationUMINAH0% (1)
- Rudolf Steiner - The Gospel of ST MarkDocumento218 páginasRudolf Steiner - The Gospel of ST Markhumblejoe100% (9)
- Narrations - Direct and Indirect SpeehesDocumento6 páginasNarrations - Direct and Indirect Speehesskitteringkite100% (1)
- Pamantasan NG Lungsod NG Valenzuela: Poblacion II, Malinta, Valenzuela CityDocumento4 páginasPamantasan NG Lungsod NG Valenzuela: Poblacion II, Malinta, Valenzuela CityAnne BustilloAinda não há avaliações
- Class ProgramsDocumento30 páginasClass Programsludivino escardaAinda não há avaliações
- Cesc Modules 8Documento6 páginasCesc Modules 8kiethly juanitezAinda não há avaliações
- 50 Questions and Answers About Tasawwuf (English) - by Ameer Maulana Akram Awan (MZA)Documento26 páginas50 Questions and Answers About Tasawwuf (English) - by Ameer Maulana Akram Awan (MZA)Azim KhanAinda não há avaliações
- A Multivariate Model For Analyzing Crime Scene InformationDocumento26 páginasA Multivariate Model For Analyzing Crime Scene InformationNorberth Ioan OkrosAinda não há avaliações
- Perfumery in Ancient IndiaDocumento9 páginasPerfumery in Ancient IndiaRachel ChittilapillyAinda não há avaliações
- Essentials or Legal Rules As To ProposalDocumento7 páginasEssentials or Legal Rules As To ProposalmasoodAinda não há avaliações
- Set 1 Questions 1-20Documento10 páginasSet 1 Questions 1-20aeda80Ainda não há avaliações
- Java Programming - Module2021Documento10 páginasJava Programming - Module2021steven hernandezAinda não há avaliações
- Canada's Top 50 FinTech CompaniesDocumento16 páginasCanada's Top 50 FinTech CompaniesTina SmithAinda não há avaliações
- 2001OxfEnc - Oxford Encyclopaedia of Ancient EgyptDocumento13 páginas2001OxfEnc - Oxford Encyclopaedia of Ancient EgyptDorrcolacAinda não há avaliações
- FSR 3.0 Frame Generation Mod Test Status (By LukeFZ)Documento10 páginasFSR 3.0 Frame Generation Mod Test Status (By LukeFZ)Gabriel GonçalvesAinda não há avaliações
- Principles of DTP Design NotesDocumento11 páginasPrinciples of DTP Design NotesSHADRACK KIRIMIAinda não há avaliações