Você também pode gostar
- Fixed Orthodontic Appliances: A Practical GuideNo EverandFixed Orthodontic Appliances: A Practical GuideNota: 1 de 5 estrelas1/5 (1)
- Case Report - Complete Denture - 2Documento4 páginasCase Report - Complete Denture - 2Astri Ggamjong Xiao LuAinda não há avaliações
- Case Report Fissure SealantDocumento8 páginasCase Report Fissure SealantrespikAinda não há avaliações
- Black Pigmentation in Primary Dentition Case Report and Literature ReviewDocumento5 páginasBlack Pigmentation in Primary Dentition Case Report and Literature ReviewlaloAinda não há avaliações
- Oral Wound Healing: Cell Biology and Clinical ManagementNo EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaAinda não há avaliações
- Old Age Psychiatry LectureDocumento38 páginasOld Age Psychiatry LectureMo 'Fishpondz' IsmailAinda não há avaliações
- Deleuze - Critical and ClinicalDocumento139 páginasDeleuze - Critical and Clinicalbornon8thofjulyAinda não há avaliações
- Termometro ManualDocumento14 páginasTermometro ManualSteve SanzAinda não há avaliações
- Extrinsic Stains and Deposits On TeethDocumento9 páginasExtrinsic Stains and Deposits On TeethFredie Jun Onio100% (1)
- Penggunaan Polyethylene Fiber-Reinforced Composite Resin Sebagai Short Post Dan Inti Pada Gigi Anterior Sulung Dengan Karies Yang Luas Laporan KasusDocumento14 páginasPenggunaan Polyethylene Fiber-Reinforced Composite Resin Sebagai Short Post Dan Inti Pada Gigi Anterior Sulung Dengan Karies Yang Luas Laporan Kasusfebriani serojaAinda não há avaliações
- Adhesive BridgesDocumento9 páginasAdhesive BridgesShilpa ShrivastavaAinda não há avaliações
- Guided Tissue RegenerationDocumento4 páginasGuided Tissue RegenerationNicoleta MarcuAinda não há avaliações
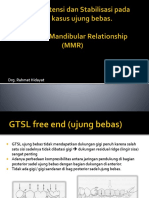
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDocumento53 páginasDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarAinda não há avaliações
- Crenated Tongue 2Documento5 páginasCrenated Tongue 2Utami MayasariAinda não há avaliações
- Classification System For Full EdentulismDocumento4 páginasClassification System For Full EdentulismmandakinimohanAinda não há avaliações
- Bedah Buku Prosto FixDocumento22 páginasBedah Buku Prosto FixLeliAinda não há avaliações
- Predictable Diastema Closure Using An Innovative Indirect Mock Up TechniqueDocumento4 páginasPredictable Diastema Closure Using An Innovative Indirect Mock Up TechniqueJane JaneeAinda não há avaliações
- Developmental DefectsDocumento29 páginasDevelopmental DefectsPrince AhmedAinda não há avaliações
- Comparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudyDocumento132 páginasComparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudySkAliHassanAinda não há avaliações
- Clinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFDocumento6 páginasClinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFZita AprilliaAinda não há avaliações
- Dental StainsDocumento30 páginasDental StainsArtur Radvanszki100% (1)
- 40 130 1 PBDocumento4 páginas40 130 1 PBrinaaa2000Ainda não há avaliações
- Modified Bluegrass Appliance PDFDocumento4 páginasModified Bluegrass Appliance PDFRenieKumalaAinda não há avaliações
- JurnalDocumento10 páginasJurnalFranciscoXavierAinda não há avaliações
- Space RegainerDocumento7 páginasSpace RegainerdelfAinda não há avaliações
- Pengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG DenpasarDocumento11 páginasPengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG DenpasarZaenuriAinda não há avaliações
- Hemiseksi Akar Distal Molar Kedua Rahang BawahDocumento5 páginasHemiseksi Akar Distal Molar Kedua Rahang BawahAhmad Willy AntonAinda não há avaliações
- An Improved Glass Ionomer Restorative System - Stress-Bearing Class I and II Indications - Dentistry TodayDocumento7 páginasAn Improved Glass Ionomer Restorative System - Stress-Bearing Class I and II Indications - Dentistry TodayKranti PrajapatiAinda não há avaliações
- Periodontics: Treatment Planning For Patients With Periodontal DiseasesDocumento17 páginasPeriodontics: Treatment Planning For Patients With Periodontal Diseasesفاطمة فالح ضايف مزعلAinda não há avaliações
- Coronoplasty 2Documento4 páginasCoronoplasty 2Befalia Aisarahmadani100% (1)
- Majalah IKORTI Desember 2015 PDFDocumento56 páginasMajalah IKORTI Desember 2015 PDFAbdi utomoAinda não há avaliações
- Space Regainers in Pediatric DentistryDocumento6 páginasSpace Regainers in Pediatric DentistryFayiz SäbAinda não há avaliações
- 1.1 Endodontik: HealingDocumento52 páginas1.1 Endodontik: HealingARINA KHAQ100% (1)
- Bulk Fill Resin RestorationDocumento18 páginasBulk Fill Resin RestorationNuningK93Ainda não há avaliações
- 14 - Perawatan Endodontic Gigi Molar Dengan Perforasi BifurkasiDocumento5 páginas14 - Perawatan Endodontic Gigi Molar Dengan Perforasi Bifurkasisarah hanifahAinda não há avaliações
- Radiografi Fraktur Kedokteran GigiDocumento16 páginasRadiografi Fraktur Kedokteran GigiFatimah Az-ZahrahAinda não há avaliações
- Gigi Tiruan Jembatan (Fixed Partial Denture) PDFDocumento25 páginasGigi Tiruan Jembatan (Fixed Partial Denture) PDFKyrkAinda não há avaliações
- Pdi Partial EdentulismDocumento67 páginasPdi Partial EdentulismAnkeeta ShuklaAinda não há avaliações
- Preparasi Gigi AbutmentDocumento15 páginasPreparasi Gigi AbutmentFransiskus Xaverius DoddieAinda não há avaliações
- Pre-Prosthetic Treatment and Tooth PreparationDocumento45 páginasPre-Prosthetic Treatment and Tooth PreparationJody JodzAinda não há avaliações
- Jurnal Mounting Articulator PDFDocumento6 páginasJurnal Mounting Articulator PDFKhaleda ShafiraAinda não há avaliações
- Dense Bone Island: Temuan Insidental Pada Radiograf PanoramikDocumento4 páginasDense Bone Island: Temuan Insidental Pada Radiograf PanoramikFransiski HoAinda não há avaliações
- A Physiologic Impression Technique For Resorbed Mandibular Ridges PDFDocumento3 páginasA Physiologic Impression Technique For Resorbed Mandibular Ridges PDFJyoti VermaAinda não há avaliações
- Cara Penggunaaan DevitalDocumento2 páginasCara Penggunaaan DevitalKrisbudiSetyawanAinda não há avaliações
- Brochure-Gc Fuji ViiDocumento16 páginasBrochure-Gc Fuji ViiZulfahmi NurdinAinda não há avaliações
- A Comparison of The Index of Complexity Outcome and Need (ICON) With The Peer Assessment Rating (PAR) and The Index of Orthodontic Treatment Need (IOTN)Documento6 páginasA Comparison of The Index of Complexity Outcome and Need (ICON) With The Peer Assessment Rating (PAR) and The Index of Orthodontic Treatment Need (IOTN)Pattrisha RaeAinda não há avaliações
- Clinical Evaluation Between Zirconia Crowns and Stainless Steel Crowns in Primary Molars TeethDocumento7 páginasClinical Evaluation Between Zirconia Crowns and Stainless Steel Crowns in Primary Molars TeethninisskyAinda não há avaliações
- Perawatan Saluran AkarDocumento19 páginasPerawatan Saluran AkarBunga Erlita RosaliaAinda não há avaliações
- FINAL SplintingDocumento46 páginasFINAL SplintingDilmohit SinghAinda não há avaliações
- Studi Literatur Terhadap Kebersihan Gigi Dan Mulut Pada Gen ZDocumento8 páginasStudi Literatur Terhadap Kebersihan Gigi Dan Mulut Pada Gen ZDaffa GemineoAinda não há avaliações
- Pengukuran Risiko Karies Gigi Dengan Kulitas SalivaDocumento25 páginasPengukuran Risiko Karies Gigi Dengan Kulitas Salivafrancisco xavier100% (1)
- Tabel IotnDocumento3 páginasTabel IotnPuspita PutriAinda não há avaliações
- Total-Etch vs. Self-Etch AdhesiveDocumento10 páginasTotal-Etch vs. Self-Etch AdhesiveCatalina MateiAinda não há avaliações
- Swing Lock Partial Denture SOWMYADocumento22 páginasSwing Lock Partial Denture SOWMYASanAinda não há avaliações
- Swing Lock Partial DentureDocumento22 páginasSwing Lock Partial DentureSanAinda não há avaliações
- Stainless Steel CrownnDocumento9 páginasStainless Steel CrownnAseelAinda não há avaliações
- Crowns Used in Pediatric DentistrDocumento85 páginasCrowns Used in Pediatric DentistrShahid Shaikh100% (1)
- Cavitypreparation 130320103634 Phpapp01Documento60 páginasCavitypreparation 130320103634 Phpapp01Sumit BediAinda não há avaliações
- CG A013 04 Stainless Steel Crowns in Deciduous MolarsDocumento5 páginasCG A013 04 Stainless Steel Crowns in Deciduous MolarsmahmoudAinda não há avaliações
- 10 .Principles of Tooth PreparationDocumento72 páginas10 .Principles of Tooth PreparationDr Tejashree CAinda não há avaliações
- FemaraDocumento2 páginasFemaraMyraIntisarAinda não há avaliações
- Chapter 1Documento20 páginasChapter 1luiperdvrouAinda não há avaliações
- ID Regulasi Keamanan Hayati Produk Rekayasa PDFDocumento18 páginasID Regulasi Keamanan Hayati Produk Rekayasa PDFPangihutan manaluAinda não há avaliações
- ENT/2CD Supplement: Notes On The Essential Newcomers Techniques CDDocumento8 páginasENT/2CD Supplement: Notes On The Essential Newcomers Techniques CDParfluf Remisenor100% (1)
- Crossmatching, Types, Principle, Procedure and InterpretationDocumento5 páginasCrossmatching, Types, Principle, Procedure and InterpretationMerhan FoudaAinda não há avaliações
- Otorhinolaryngology, Head & Neck Surgery Department Cornwall Regional Hospital (W.R.H.A)Documento1 páginaOtorhinolaryngology, Head & Neck Surgery Department Cornwall Regional Hospital (W.R.H.A)Giovanni HenryAinda não há avaliações
- Overview of Selected Family Therapy ModelsDocumento5 páginasOverview of Selected Family Therapy ModelsErin Richardson100% (1)
- Periodontal Ligament: Ganesh Ganji 2 Year PGDocumento34 páginasPeriodontal Ligament: Ganesh Ganji 2 Year PGNareshAinda não há avaliações
- Compliance Program Guidance Manual 7341.002 PDFDocumento45 páginasCompliance Program Guidance Manual 7341.002 PDFpopatlilo2Ainda não há avaliações
- Leave and Joining Time Rules: National Seeds Corporation Limited (A Government of India Undertaking)Documento26 páginasLeave and Joining Time Rules: National Seeds Corporation Limited (A Government of India Undertaking)Rojan MathewAinda não há avaliações
- High Res.Documento162 páginasHigh Res.Nando93100% (1)
- MCAT SecretsDocumento32 páginasMCAT SecretsTunde Ipaye100% (2)
- Postglacial Foraging in The Forests of EuropeDocumento13 páginasPostglacial Foraging in The Forests of EuropeShreyashi KashyapAinda não há avaliações
- Sun Salutations Yoga Lesson PlanDocumento8 páginasSun Salutations Yoga Lesson PlanErica Harris100% (1)
- (Metals and Related Substances in Drinking Water Research Rep) M. Ferrante, G. Oliveri Conti, Z. Rasic-Milutinovic-Health Effects of Metals and Related Substances in Drinking Water-IWA Publishing (201Documento150 páginas(Metals and Related Substances in Drinking Water Research Rep) M. Ferrante, G. Oliveri Conti, Z. Rasic-Milutinovic-Health Effects of Metals and Related Substances in Drinking Water-IWA Publishing (201franklinAinda não há avaliações
- Episodic Migraine Surveillance Report 3Documento79 páginasEpisodic Migraine Surveillance Report 3AudryaAinda não há avaliações
- Presentasi Bio-Strath 2016Documento28 páginasPresentasi Bio-Strath 2016Imanluves Amel100% (1)
- 18 Vessels and Flow DynamicsDocumento57 páginas18 Vessels and Flow Dynamicsraanja2Ainda não há avaliações
- Andrew Austin - IEMT & Long Term Anxiety - DVD Cover PDFDocumento2 páginasAndrew Austin - IEMT & Long Term Anxiety - DVD Cover PDFMichael CliftonAinda não há avaliações
- Medications For Primary ComplexDocumento8 páginasMedications For Primary ComplexMary CruzAinda não há avaliações
- Ross Rabindranath Mission Issue-2Documento24 páginasRoss Rabindranath Mission Issue-2RanenDasguptaAinda não há avaliações
- Handbook of PEDIATRIC SURGERY PDFDocumento43 páginasHandbook of PEDIATRIC SURGERY PDFPETERAinda não há avaliações
- Influencia de La Postura Del Pie en El Mecanismo de Windlass, Ensayo ClinicoDocumento20 páginasInfluencia de La Postura Del Pie en El Mecanismo de Windlass, Ensayo ClinicoAlberto Jesús CamposAinda não há avaliações
- CL November2016Documento24 páginasCL November2016patruoxAinda não há avaliações
- Dentists in LimassolDocumento26 páginasDentists in LimassolANDREASBOULAinda não há avaliações
- 4 671945747968557164Documento67 páginas4 671945747968557164McMillanAinda não há avaliações
- ADHD: Clinical Practice Guideline For The Diagnosis, Evaluation, and TreatmentDocumento18 páginasADHD: Clinical Practice Guideline For The Diagnosis, Evaluation, and TreatmentBen CulpepperAinda não há avaliações