Você também pode gostar
- Is COVID-19 a Bioweapon?: A Scientific and Forensic InvestigationNo EverandIs COVID-19 a Bioweapon?: A Scientific and Forensic InvestigationNota: 5 de 5 estrelas5/5 (3)
- Getting Risk Right: Understanding the Science of Elusive Health RisksNo EverandGetting Risk Right: Understanding the Science of Elusive Health RisksAinda não há avaliações
- New Microsoft Word DocumentDocumento6 páginasNew Microsoft Word DocumentRaymala RamanAinda não há avaliações
- Statistical Analysis Linking U.S. AIDS Outbreak To Hepatitis ExperimentsDocumento65 páginasStatistical Analysis Linking U.S. AIDS Outbreak To Hepatitis Experimentsst_spyridonAinda não há avaliações
- Retributivism and Over-Punishment Douglas HusakDocumento22 páginasRetributivism and Over-Punishment Douglas HusakIana Solange Ingrid MarinaAinda não há avaliações
- COVID-19 and Public Health Totalitarianism DR BREGGINDocumento204 páginasCOVID-19 and Public Health Totalitarianism DR BREGGINJade LaceyAinda não há avaliações
- Statistical Ethics in Medical Research A Narrative ReviewDocumento10 páginasStatistical Ethics in Medical Research A Narrative ReviewAthenaeum Scientific PublishersAinda não há avaliações
- Fabrication, Falsification and PlagiarismDocumento2 páginasFabrication, Falsification and PlagiarismCARDIO 2019Ainda não há avaliações
- White Paper Track OnDocumento7 páginasWhite Paper Track Onapi-665597421Ainda não há avaliações
- Misinformation About COVID-19: Evidence For Differential Latent Profiles and A Strong Association With Trust in ScienceDocumento12 páginasMisinformation About COVID-19: Evidence For Differential Latent Profiles and A Strong Association With Trust in SciencegamerriddlesAinda não há avaliações
- Victimless Crime, Rightfully Illegal?Documento64 páginasVictimless Crime, Rightfully Illegal?ben_thomas_salmonAinda não há avaliações
- English 1a - Research ProposalDocumento3 páginasEnglish 1a - Research Proposalapi-302515969Ainda não há avaliações
- Agar - Drugmart - Heroin Epidemics As Complex Adaptative SystemsDocumento9 páginasAgar - Drugmart - Heroin Epidemics As Complex Adaptative SystemscgfelicianoAinda não há avaliações
- Mike Yeadon May21Documento19 páginasMike Yeadon May21martinscodellerAinda não há avaliações
- Int. J. Epidemiol. 2009 Cornfield 1175 91Documento17 páginasInt. J. Epidemiol. 2009 Cornfield 1175 91winardi rAinda não há avaliações
- Bioethics On The Couch: PerspectivesDocumento9 páginasBioethics On The Couch: PerspectivesdocsincloudAinda não há avaliações
- Bichara2021 Article WhatDoCOVID-19TweetsRevealAbouDocumento31 páginasBichara2021 Article WhatDoCOVID-19TweetsRevealAbouGabi FPAinda não há avaliações
- Literature Review On Tuberculosis in PrisonsDocumento6 páginasLiterature Review On Tuberculosis in Prisonsaflskkcez100% (1)
- Boda - Paradoxes of Populism - Intersections2021Documento8 páginasBoda - Paradoxes of Populism - Intersections2021Zsolt BodaAinda não há avaliações
- Systematic Review and Meta-Analysis of Prevalence Studies in TranssexualismDocumento39 páginasSystematic Review and Meta-Analysis of Prevalence Studies in Transsexualismtafazzal.eduAinda não há avaliações
- ARGUEDAS Et Al. - Echo Chambers Filter Bubbles and Polarisation A Literature ReviewDocumento42 páginasARGUEDAS Et Al. - Echo Chambers Filter Bubbles and Polarisation A Literature ReviewLeonardo MonteiroAinda não há avaliações
- The Marijuana Smokers - Erich GoodeDocumento321 páginasThe Marijuana Smokers - Erich GoodeEdwin Solano ReyesAinda não há avaliações
- In Defense of The Right To Life Analyzing Factors Affecting Filipino-CompressedDocumento42 páginasIn Defense of The Right To Life Analyzing Factors Affecting Filipino-CompressedEva montañoAinda não há avaliações
- The Anthropology of Public Health: Journal of Biosocial Science February 2006Documento6 páginasThe Anthropology of Public Health: Journal of Biosocial Science February 2006sugamilasAinda não há avaliações
- Hostile Fantasy-World of Zbigniew BrzezinskiDocumento77 páginasHostile Fantasy-World of Zbigniew BrzezinskiMichael BrownAinda não há avaliações
- Ethics PaperDocumento6 páginasEthics PaperTina BayAinda não há avaliações
- Global Health and Scientific Research (Flory, 2004)Documento30 páginasGlobal Health and Scientific Research (Flory, 2004)Faz RahmanAinda não há avaliações
- Analytic Thinking Predicts Hoax Beliefs and Helping Behaviors in Response To The COVID 19 PandemicDocumento15 páginasAnalytic Thinking Predicts Hoax Beliefs and Helping Behaviors in Response To The COVID 19 PandemicAchilleasAinda não há avaliações
- Book - Science in Social Context-5Documento30 páginasBook - Science in Social Context-5Deklin FrantiusAinda não há avaliações
- Action-Items CXVII (Fascism, Gun-Control, Internet, First Amendment, NSA, GOP's POTUS-'16, Jonah Goldberg, Wendy Davis)Documento15 páginasAction-Items CXVII (Fascism, Gun-Control, Internet, First Amendment, NSA, GOP's POTUS-'16, Jonah Goldberg, Wendy Davis)Robert B. SklaroffAinda não há avaliações
- The Infodemic' of COVID-19 Misinformation, ExplainedDocumento4 páginasThe Infodemic' of COVID-19 Misinformation, Explainedcharanmann9165Ainda não há avaliações
- Phil Final PaperDocumento4 páginasPhil Final PaperHarry PotplantAinda não há avaliações
- Mental Hygiene & Soc. EnvDocumento22 páginasMental Hygiene & Soc. Envandi lilisAinda não há avaliações
- Manuscript 4Documento37 páginasManuscript 4M.J. ConawayAinda não há avaliações
- How To Talk To Coronavirus Skeptics The New Yorker 23III2020Documento9 páginasHow To Talk To Coronavirus Skeptics The New Yorker 23III2020LuisMiguelTrejoAinda não há avaliações
- HIV and AIDSDocumento27 páginasHIV and AIDSSankhadeep MaitiAinda não há avaliações
- Dissertation Victimless CrimeDocumento65 páginasDissertation Victimless CrimeBenjamin SalmonAinda não há avaliações
- Pathologies of PowerDocumento11 páginasPathologies of PowermikejablonskiAinda não há avaliações
- Research Paper On CDCDocumento8 páginasResearch Paper On CDCacpjxhznd100% (1)
- The Corona Lie - unmasked: Evidence, facts, backgroundsNo EverandThe Corona Lie - unmasked: Evidence, facts, backgroundsAinda não há avaliações
- Turning Science Into Junk: - The Tobacco Industry's Research On Passive Smoking (2001)Documento3 páginasTurning Science Into Junk: - The Tobacco Industry's Research On Passive Smoking (2001)EMFsafetyAinda não há avaliações
- Research On CancerDocumento11 páginasResearch On Cancerrubyshah886Ainda não há avaliações
- The Quick OverviewDocumento8 páginasThe Quick OverviewketaAinda não há avaliações
- The Quick Fix: Why Fad Psychology Can't Cure Our Social IllsNo EverandThe Quick Fix: Why Fad Psychology Can't Cure Our Social IllsNota: 4 de 5 estrelas4/5 (6)
- Report On The State of Health + Urbanism: A CritiqueDocumento15 páginasReport On The State of Health + Urbanism: A Critiquearchitectmag100% (1)
- DraftDocumento7 páginasDraftapi-302322358Ainda não há avaliações
- Human Challenge Vaccine TrialsDocumento4 páginasHuman Challenge Vaccine TrialsToby GriffithsAinda não há avaliações
- Draft With CommentsDocumento7 páginasDraft With Commentsapi-302322358Ainda não há avaliações
- Researcharticle Open AccessDocumento14 páginasResearcharticle Open AccessHIV Justice NetworkAinda não há avaliações
- Handbook On Ethical Issues in Anthropology - Case 23 - Slow CodeDocumento4 páginasHandbook On Ethical Issues in Anthropology - Case 23 - Slow CodeSerena SunAinda não há avaliações
- Noam Chomsky On Drugs: A Little Insite On The Hypocrisy of It AllDocumento52 páginasNoam Chomsky On Drugs: A Little Insite On The Hypocrisy of It AllMano RatyiAinda não há avaliações
- Race in The NewsDocumento4 páginasRace in The NewsKashémAinda não há avaliações
- Assessing Evidence Assessing EvidenceDocumento9 páginasAssessing Evidence Assessing Evidencetulus setiawanAinda não há avaliações
- Daston ZiFPandemicMay2020Documento6 páginasDaston ZiFPandemicMay2020swapnajit mukherjeeAinda não há avaliações
- Cultivation TheoryDocumento13 páginasCultivation TheoryNur' Ain ZamriAinda não há avaliações
- Media Influence: Nature Versus Nurture?Documento7 páginasMedia Influence: Nature Versus Nurture?nii_naiAinda não há avaliações
- How Malleable Are Attitudes To Crime andDocumento20 páginasHow Malleable Are Attitudes To Crime andIoana ChișcaruAinda não há avaliações
- 【公报】美国传播学研究 批判视角Documento7 páginas【公报】美国传播学研究 批判视角yi linAinda não há avaliações
- Studies in Forensic Psychiatry by Glueck, Bernard, 1883Documento132 páginasStudies in Forensic Psychiatry by Glueck, Bernard, 1883Gutenberg.orgAinda não há avaliações
- Topics in Contemporary EthicsDocumento10 páginasTopics in Contemporary Ethicshutten7Ainda não há avaliações
- Unemployment Rate, UK, Age 16+Documento1 páginaUnemployment Rate, UK, Age 16+jodyaberdeinAinda não há avaliações
- Ratio Price To DemandDocumento1 páginaRatio Price To DemandjodyaberdeinAinda não há avaliações
- Interest PDFDocumento1 páginaInterest PDFjodyaberdeinAinda não há avaliações
- House PricesDocumento1 páginaHouse PricesjodyaberdeinAinda não há avaliações
- House Prices Vs DemandDocumento1 páginaHouse Prices Vs DemandjodyaberdeinAinda não há avaliações
- Deerfield - 2016Documento265 páginasDeerfield - 2016DJ EntropyAinda não há avaliações
- Reading IDocumento7 páginasReading ITimur TkachenkoAinda não há avaliações
- Obligations Part 1Documento2 páginasObligations Part 1Wawex DavisAinda não há avaliações
- ER Ejercito vs. ComelecDocumento3 páginasER Ejercito vs. ComeleckristinevillanuevaAinda não há avaliações
- SR No. Organization Name Designation Telephone NoDocumento110 páginasSR No. Organization Name Designation Telephone No3J Solutions BDAinda não há avaliações
- Duties of Seamen in ShipDocumento6 páginasDuties of Seamen in ShipRicardo Garate100% (1)
- African American Studies Thesis TopicsDocumento4 páginasAfrican American Studies Thesis Topicstarahardinhuntsville100% (2)
- Tamil Nadu Occupants of Kudiyiruppu (Protection From Eviction) Re PDFDocumento3 páginasTamil Nadu Occupants of Kudiyiruppu (Protection From Eviction) Re PDFLatest Laws TeamAinda não há avaliações
- Shahidur Rahman - MedicalDocumento2 páginasShahidur Rahman - MedicalMd Aminul AlamAinda não há avaliações
- Abacus Real Estate Development v. Manila Banking Corporation, G.R. No. 162270, April 6, 2005Documento2 páginasAbacus Real Estate Development v. Manila Banking Corporation, G.R. No. 162270, April 6, 2005Metsuyo BariteAinda não há avaliações
- Management of Benzodiazepine Misuse and Dependence: Jonathan Brett Bridin MurnionDocumento4 páginasManagement of Benzodiazepine Misuse and Dependence: Jonathan Brett Bridin MurnionLucius MarpleAinda não há avaliações
- People Vs BayotasDocumento1 páginaPeople Vs BayotasAffle John Leonor100% (1)
- Villanueva v. VelascoDocumento6 páginasVillanueva v. Velascored gynAinda não há avaliações
- Tafsir Surah Hashr Verse 10 - Tayseer Al-Kareem Ar-Rahman - Shaykh 'Abdur Rahman As Sa'diDocumento4 páginasTafsir Surah Hashr Verse 10 - Tayseer Al-Kareem Ar-Rahman - Shaykh 'Abdur Rahman As Sa'diMountainofknowledgeAinda não há avaliações
- Burke, Williams & Sorensen, LLP Proposal - RedactedDocumento19 páginasBurke, Williams & Sorensen, LLP Proposal - RedactedL. A. PatersonAinda não há avaliações
- Bullying Among Malaysian Elementary School ChildrenDocumento6 páginasBullying Among Malaysian Elementary School ChildrenPerantau KayAinda não há avaliações
- Views & Suggestions of Participants National Youth Parliament Festival 2019Documento547 páginasViews & Suggestions of Participants National Youth Parliament Festival 2019vaibhav yadavAinda não há avaliações
- Regional Trial Court Branch 51: Rtc2sor051@judiciary - Gov.phDocumento4 páginasRegional Trial Court Branch 51: Rtc2sor051@judiciary - Gov.phMaricrisAinda não há avaliações
- Laoang, Northern SamarDocumento2 páginasLaoang, Northern SamarSunStar Philippine NewsAinda não há avaliações
- Life in Sparta PDFDocumento2 páginasLife in Sparta PDFGabriel BispoAinda não há avaliações
- Les 1965Documento104 páginasLes 1965sureshAinda não há avaliações
- Ap 1Documento9 páginasAp 1RaviKiran AvulaAinda não há avaliações
- Victoria BC Current Waterfront Homes For SaleDocumento4 páginasVictoria BC Current Waterfront Homes For SaleFred Carver100% (1)
- Money Claim FormDocumento3 páginasMoney Claim FormHihiAinda não há avaliações
- Kramer - KronstadtDocumento5 páginasKramer - KronstadtRohitAinda não há avaliações
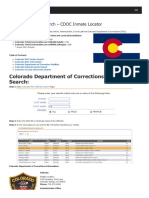
- Colorado Inmate Search Department of Corrections LookupDocumento9 páginasColorado Inmate Search Department of Corrections LookupinmatesearchinfoAinda não há avaliações
- Rizal 1Documento14 páginasRizal 1LokomokoAinda não há avaliações
- INTRODUCTION TO NURISTANI TRIBES, LANGUAGES AND DILECTS - DotxDocumento11 páginasINTRODUCTION TO NURISTANI TRIBES, LANGUAGES AND DILECTS - DotxAhmadAinda não há avaliações
- Robbery and DacoityDocumento21 páginasRobbery and DacoitySiddhant SodhiaAinda não há avaliações
- Appendix 9 Contract TermsDocumento12 páginasAppendix 9 Contract TermsNadir ShahAinda não há avaliações