Você também pode gostar
- The Predominantly Plant-Based Pregnancy GuideDocumento179 páginasThe Predominantly Plant-Based Pregnancy GuidePriscila Tobar Alcántar100% (1)
- Ajuste de Dosis de Medicamentos en Paciente RenalDocumento46 páginasAjuste de Dosis de Medicamentos en Paciente RenalThelma Cantillo RochaAinda não há avaliações
- La Teta Cansada - Montserrat Reverte PDFDocumento4 páginasLa Teta Cansada - Montserrat Reverte PDFIpAinda não há avaliações
- HGO Aplicaciones Clinicas JamaDocumento4 páginasHGO Aplicaciones Clinicas JamaPriscila Tobar AlcántarAinda não há avaliações
- Breastfeeding Medicine Protocol on GalactogoguesDocumento8 páginasBreastfeeding Medicine Protocol on GalactogoguespaulinaovAinda não há avaliações
- Diabetic KetoacidosisDocumento16 páginasDiabetic Ketoacidosisdrtpk100% (2)
- Hiper Hipoparatir NejmDocumento13 páginasHiper Hipoparatir NejmPriscila Tobar AlcántarAinda não há avaliações
- MayoClinProc Anemia in Adults A Contemporary Approach To DiagnosisDocumento7 páginasMayoClinProc Anemia in Adults A Contemporary Approach To DiagnosisBarbarita Alvarado CamposAinda não há avaliações
- Acute Appendicitis in AdultsDocumento20 páginasAcute Appendicitis in AdultsPriscila Tobar AlcántarAinda não há avaliações
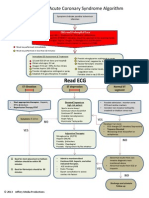
- ACS Algorithm DiagramDocumento1 páginaACS Algorithm DiagramPriscila Tobar Alcántar100% (1)
- Acute Appendicitis in Adults ManagementDocumento16 páginasAcute Appendicitis in Adults ManagementPriscila Tobar AlcántarAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Case NoDocumento13 páginasCase NoLaurente JessicaAinda não há avaliações
- Rozgar Sutra EnglishDocumento105 páginasRozgar Sutra EnglishRisingsun PradhanAinda não há avaliações
- 45 - Altivar 61 Plus Variable Speed DrivesDocumento130 páginas45 - Altivar 61 Plus Variable Speed Drivesabdul aziz alfiAinda não há avaliações
- Method Statement Pressure TestingDocumento15 páginasMethod Statement Pressure TestingAkmaldeen AhamedAinda não há avaliações
- 09 Lift Cylinder Drift (Bulldozer) - CheckDocumento2 páginas09 Lift Cylinder Drift (Bulldozer) - CheckFredy Manrique AstoAinda não há avaliações
- Entrepreneurial Intentions of Cavite Business StudentsDocumento12 páginasEntrepreneurial Intentions of Cavite Business StudentsKevin Pereña GuinsisanaAinda não há avaliações
- The NicotinaDocumento8 páginasThe Nicotinab0beiiiAinda não há avaliações
- Dinflo DFCSDocumento2 páginasDinflo DFCSvictorharijantoAinda não há avaliações
- Attribute Achievement FormDocumento15 páginasAttribute Achievement FormMiguel MenesesAinda não há avaliações
- Facebook Facing Off Againt TencentDocumento6 páginasFacebook Facing Off Againt TencentWai Shan Lee0% (1)
- Isaac Asimov - "Nightfall"Documento20 páginasIsaac Asimov - "Nightfall"Aditya Sharma100% (1)
- India's 1991 Economic ReformsDocumento5 páginasIndia's 1991 Economic ReformsLive AspireAinda não há avaliações
- Subtracting-Fractions-Unlike DenominatorsDocumento2 páginasSubtracting-Fractions-Unlike Denominatorsapi-3953531900% (1)
- On-Chip ESD Protection Design For IcsDocumento14 páginasOn-Chip ESD Protection Design For IcsMK BricksAinda não há avaliações
- The English Center Articulation AgreementDocumento9 páginasThe English Center Articulation AgreementJose CabreraAinda não há avaliações
- Asset Valuation: Debt Investments: Analysis and Valuation: 1 2 N M 1 2 N MDocumento23 páginasAsset Valuation: Debt Investments: Analysis and Valuation: 1 2 N M 1 2 N MSirSmirkAinda não há avaliações
- Ecma L1221BR3 PD02 05172016Documento2 páginasEcma L1221BR3 PD02 05172016Anil JindalAinda não há avaliações
- EMC Design Guide For PCBDocumento78 páginasEMC Design Guide For PCBFaruq AhmedAinda não há avaliações
- Regional Office X: Republic of The PhilippinesDocumento2 páginasRegional Office X: Republic of The PhilippinesCoreine Imee ValledorAinda não há avaliações
- Physics Force and BuoyancyDocumento28 páginasPhysics Force and BuoyancySohan PattanayakAinda não há avaliações
- Valhalla Repair ManualDocumento8 páginasValhalla Repair ManualKirby AllenAinda não há avaliações
- Site AnalysisDocumento15 páginasSite Analysismaanik005Ainda não há avaliações
- XLVI ESAN INTERNATIONAL WEEK (MBA Only - July 2023)Documento38 páginasXLVI ESAN INTERNATIONAL WEEK (MBA Only - July 2023)Juan Diego Fernández CastilloAinda não há avaliações
- Securing Obligations Through Pledge and MortgageDocumento4 páginasSecuring Obligations Through Pledge and MortgagePrincessAngelaDeLeon100% (1)
- Protección Fuego MetalDocumento16 páginasProtección Fuego MetalTracy Mora ChAinda não há avaliações
- Flexural Analysis of Beams (Part 2)Documento7 páginasFlexural Analysis of Beams (Part 2)Johnnette Nafuerza AggabaoAinda não há avaliações
- TheSun 2008-11-04 Page16 Asian Stocks Rally Continues On Policy HopesDocumento1 páginaTheSun 2008-11-04 Page16 Asian Stocks Rally Continues On Policy HopesImpulsive collectorAinda não há avaliações
- NYU Stern Evaluation NewsletterDocumento25 páginasNYU Stern Evaluation NewsletterCanadianValueAinda não há avaliações
- Anna University CTDocumento3 páginasAnna University CTprayog8Ainda não há avaliações
- VNACS Final Case ReportDocumento9 páginasVNACS Final Case ReportVikram Singh TomarAinda não há avaliações