Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Essential Calculus Skills Practice Workbook With Full SolutionsDocumento528 páginasEssential Calculus Skills Practice Workbook With Full SolutionsGerardo Navarro Sánchez94% (65)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Joby Aviation - Analyst Day PresentationDocumento100 páginasJoby Aviation - Analyst Day PresentationIan TanAinda não há avaliações
- Critical Analysis of W.H Auden Poems The PDFDocumento8 páginasCritical Analysis of W.H Auden Poems The PDFMöĤämmĔd äĹ-ŚäÁdï100% (1)
- Times Square C2C Cardigan: Finished Measurements NotionsDocumento8 páginasTimes Square C2C Cardigan: Finished Measurements Notionsdiana.alyAinda não há avaliações
- Synthesis Essay Coming To Grips With GenesisDocumento11 páginasSynthesis Essay Coming To Grips With Genesisapi-259381516Ainda não há avaliações
- New Bon-NleDocumento3 páginasNew Bon-NleCristina L. JaysonAinda não há avaliações
- HAAD ReviewerDocumento35 páginasHAAD ReviewerSydRey92% (24)
- Gaffin, Biblical Theology and Westminster StandardsDocumento16 páginasGaffin, Biblical Theology and Westminster StandardstheoarticlesAinda não há avaliações
- Rachel Joyce - A Snow Garden and Other Stories PDFDocumento118 páginasRachel Joyce - A Snow Garden and Other Stories PDFИгорь ЯковлевAinda não há avaliações
- Iodide and Bromide Ions in Brackish Water, Seawater, and Brines D 3869 - 04Documento12 páginasIodide and Bromide Ions in Brackish Water, Seawater, and Brines D 3869 - 04stevgonAinda não há avaliações
- OooDocumento1 páginaOooCristina L. JaysonAinda não há avaliações
- Individual Therapy Key PointsDocumento9 páginasIndividual Therapy Key PointsCristina L. JaysonAinda não há avaliações
- Mindanao Sanitarium & Hospital College: D.R. Form Actual Delivery FormDocumento1 páginaMindanao Sanitarium & Hospital College: D.R. Form Actual Delivery FormCristina L. JaysonAinda não há avaliações
- 3 RDDocumento1 página3 RDCristina L. JaysonAinda não há avaliações
- 1 STPRCDocumento1 página1 STPRCCristina L. JaysonAinda não há avaliações
- HelloDocumento1 páginaHelloCristina L. JaysonAinda não há avaliações
- PRC TinaDocumento4 páginasPRC TinaCristina L. JaysonAinda não há avaliações
- BibliographyDocumento1 páginaBibliographyCristina L. JaysonAinda não há avaliações
- May 2014 NLE Rooms CDODocumento71 páginasMay 2014 NLE Rooms CDOCoolbuster.NetAinda não há avaliações
- Grand Case Presentation InformationDocumento7 páginasGrand Case Presentation InformationCristina L. JaysonAinda não há avaliações
- FBDocumento1 páginaFBCristina L. JaysonAinda não há avaliações
- CorrectionsDocumento4 páginasCorrectionsCristina L. JaysonAinda não há avaliações
- 634379489751247500Documento32 páginas634379489751247500Cristina L. JaysonAinda não há avaliações
- Nursing HistoryDocumento1 páginaNursing HistoryCristina L. JaysonAinda não há avaliações
- Normal Anatomy and PhysiologyDocumento8 páginasNormal Anatomy and PhysiologyCristina L. JaysonAinda não há avaliações
- NCPDocumento10 páginasNCPCristina L. JaysonAinda não há avaliações
- Diagnostic TestsDocumento11 páginasDiagnostic TestsCristina L. JaysonAinda não há avaliações
- Diagnostic TestsDocumento11 páginasDiagnostic TestsCristina L. JaysonAinda não há avaliações
- GordonsDocumento3 páginasGordonsCristina L. JaysonAinda não há avaliações
- IrisDocumento4 páginasIrisYazmin Vasquez BarreraAinda não há avaliações
- PerosDocumento5 páginasPerosCristina L. JaysonAinda não há avaliações
- References For Drug Study and Diagnostic TestsDocumento2 páginasReferences For Drug Study and Diagnostic TestsCristina L. JaysonAinda não há avaliações
- 1st Phase ReportDocumento42 páginas1st Phase ReportCristina L. JaysonAinda não há avaliações
- Phytoplankton Data DipsinDocumento125 páginasPhytoplankton Data DipsinCristina L. JaysonAinda não há avaliações
- Final DefenseDocumento16 páginasFinal DefenseCristina L. JaysonAinda não há avaliações
- Project Contract For Phyto Ra-2Documento1 páginaProject Contract For Phyto Ra-2Cristina L. JaysonAinda não há avaliações
- Project Contract For Phyto Ra-2Documento1 páginaProject Contract For Phyto Ra-2Cristina L. JaysonAinda não há avaliações
- 3vital Information: Year) - BSED BioDocumento3 páginas3vital Information: Year) - BSED BioCristina L. JaysonAinda não há avaliações
- CS402 Mcqs MidTerm by Vu Topper RMDocumento50 páginasCS402 Mcqs MidTerm by Vu Topper RMM. KhizarAinda não há avaliações
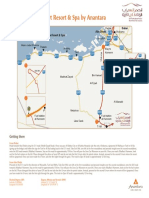
- Qasr Al Sarab Desert Resort Location Map June2012Documento1 páginaQasr Al Sarab Desert Resort Location Map June2012Anant GârgAinda não há avaliações
- Usp Description and SolubilityDocumento1 páginaUsp Description and SolubilityvafaashkAinda não há avaliações
- Ict 2120 Animation NC Ii Week 11 20 by Francis Isaac 1Documento14 páginasIct 2120 Animation NC Ii Week 11 20 by Francis Isaac 1Chiropractic Marketing NowAinda não há avaliações
- Paper-Czechowski-Slow-strain-rate Stress Corrosion Testing of Welded Joints of Al-Mg AlloysDocumento4 páginasPaper-Czechowski-Slow-strain-rate Stress Corrosion Testing of Welded Joints of Al-Mg Alloysjavo0128Ainda não há avaliações
- Line Differential Protection Red670Documento8 páginasLine Differential Protection Red670igorsfaceAinda não há avaliações
- WeeklyDocumento8 páginasWeeklyivaldeztAinda não há avaliações
- W0L0XCF0866101640 (2006 Opel Corsa) PDFDocumento7 páginasW0L0XCF0866101640 (2006 Opel Corsa) PDFgianyAinda não há avaliações
- Region 1 - Concreting Works Materials Prices - PHILCON PRICESDocumento9 páginasRegion 1 - Concreting Works Materials Prices - PHILCON PRICESMark Gregory RimandoAinda não há avaliações
- MA 106: Linear Algebra Tutorial 1: Prof. B.V. Limaye IIT DharwadDocumento4 páginasMA 106: Linear Algebra Tutorial 1: Prof. B.V. Limaye IIT Dharwadamar BaroniaAinda não há avaliações
- Atomic St. Package PDFDocumento28 páginasAtomic St. Package PDFSatvik RaoAinda não há avaliações
- Armadio Presentation-2019Documento45 páginasArmadio Presentation-2019Subhash Singh TomarAinda não há avaliações
- Manuscript FsDocumento76 páginasManuscript FsRalph HumpaAinda não há avaliações
- Badminton ReviewerDocumento10 páginasBadminton ReviewerHailsey WinterAinda não há avaliações
- Kelas ChondrichtyesDocumento15 páginasKelas ChondrichtyesanitagustinawatiAinda não há avaliações
- Optik: Original Research ArticleDocumento6 páginasOptik: Original Research ArticlesimarpreetAinda não há avaliações
- Minimalist KWL Graphic OrganizerDocumento2 páginasMinimalist KWL Graphic OrganizerIrish Nicole AlanoAinda não há avaliações
- Physics Unit 11 NotesDocumento26 páginasPhysics Unit 11 Notesp.salise352Ainda não há avaliações
- 2017 Classification of Periodontal and Peri-Implant Diseases and Conditions. Decision Making Algorithms For Clinical PracticeDocumento40 páginas2017 Classification of Periodontal and Peri-Implant Diseases and Conditions. Decision Making Algorithms For Clinical PracticebbAinda não há avaliações
- Azure Machine Learning StudioDocumento17 páginasAzure Machine Learning StudioNurain IsmailAinda não há avaliações
- Clinical Reviews: The Management of Children With Gastroenteritis and Dehydration in The Emergency DepartmentDocumento13 páginasClinical Reviews: The Management of Children With Gastroenteritis and Dehydration in The Emergency DepartmentRina Dewi AnggraeniAinda não há avaliações
- Esterification Oil of WintergreenDocumento8 páginasEsterification Oil of WintergreenMaria MahusayAinda não há avaliações