Você também pode gostar
- Usmle Surgery Mcqs PDFDocumento2 páginasUsmle Surgery Mcqs PDFGhadeer Ebraheem75% (4)
- English Time 3Documento79 páginasEnglish Time 3Ghadeer Ebraheem100% (2)
- HIV and HIV CounsellingDocumento12 páginasHIV and HIV CounsellingGhadeer EbraheemAinda não há avaliações
- Leach and Lily Stanley - Last Updated On: Edit This Article View RevisionsDocumento7 páginasLeach and Lily Stanley - Last Updated On: Edit This Article View RevisionsGhadeer EbraheemAinda não há avaliações
- ATLS DRDocumento45 páginasATLS DRNeNeei HenNieAinda não há avaliações
- Antibody Tests Reveal Red Blood Cell AntibodiesDocumento2 páginasAntibody Tests Reveal Red Blood Cell AntibodiesGhadeer EbraheemAinda não há avaliações
- Myotomes of The Upper LimbDocumento2 páginasMyotomes of The Upper LimbGhadeer Ebraheem0% (1)
- One Hundred YearsDocumento18 páginasOne Hundred YearsolziichAinda não há avaliações
- GcsDocumento1 páginaGcsGhadeer EbraheemAinda não há avaliações
- Mansmed Surgery QbankDocumento7 páginasMansmed Surgery QbankGhadeer EbraheemAinda não há avaliações
- Medical Therapies for Antibody DeficienciesDocumento5 páginasMedical Therapies for Antibody DeficienciesGhadeer EbraheemAinda não há avaliações
- Leach and Lily Stanley - Last Updated On: Edit This Article View RevisionsDocumento7 páginasLeach and Lily Stanley - Last Updated On: Edit This Article View RevisionsGhadeer EbraheemAinda não há avaliações
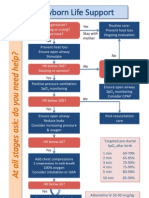
- Arc Neonatal FlowchartDocumento1 páginaArc Neonatal FlowchartChander KantaAinda não há avaliações
- HIV and HIV CounsellingDocumento12 páginasHIV and HIV CounsellingGhadeer EbraheemAinda não há avaliações
- Neuro ExaminationDocumento82 páginasNeuro ExaminationGhadeer Ebraheem100% (1)
- Acid Base PhysiologyDocumento4 páginasAcid Base PhysiologyGhadeer EbraheemAinda não há avaliações
- RicketsDocumento7 páginasRicketsGhadeer EbraheemAinda não há avaliações
- PalsDocumento12 páginasPalsGhadeer EbraheemAinda não há avaliações
- 5 - Health Care System Awad Etc 2009Documento11 páginas5 - Health Care System Awad Etc 2009Ghadeer EbraheemAinda não há avaliações
- Inflamatory Bowel Disease: Dr. Samir IsmailDocumento82 páginasInflamatory Bowel Disease: Dr. Samir IsmailGhadeer EbraheemAinda não há avaliações
- Drugs Causing HirsutismDocumento1 páginaDrugs Causing HirsutismGhadeer EbraheemAinda não há avaliações
- Anatomy 2 MnemonicsDocumento46 páginasAnatomy 2 MnemonicsGhadeer EbraheemAinda não há avaliações
- Drugs Causing HirsutismDocumento1 páginaDrugs Causing HirsutismGhadeer EbraheemAinda não há avaliações
- Nephrotic SyndromeDocumento1 páginaNephrotic SyndromeGhadeer EbraheemAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Nicotine-Induced Conditioned Place Preference and Conditioned Place Aversion in MiceDocumento5 páginasNicotine-Induced Conditioned Place Preference and Conditioned Place Aversion in MiceAulas EspañolAinda não há avaliações
- Nicotine Replacement Therapy A Friend or FoeDocumento6 páginasNicotine Replacement Therapy A Friend or FoeVsh SngAinda não há avaliações
- Nicotine Dependence SyndromeDocumento51 páginasNicotine Dependence SyndromeTesitaAinda não há avaliações
- Accounting EstimatesniceDocumento34 páginasAccounting EstimatesniceAnthony Tunying MantuhacAinda não há avaliações
- Bio Investigatory ProjectDocumento16 páginasBio Investigatory Projectprism1702Ainda não há avaliações
- Alcohol and Tobacco AddictionDocumento6 páginasAlcohol and Tobacco AddictionVijayAinda não há avaliações
- Gateway Drugs: The Dangers of Cigarette SmokingDocumento20 páginasGateway Drugs: The Dangers of Cigarette SmokingAllorasaxAinda não há avaliações
- Forced Smoking Stories I'Ve CollectedDocumento241 páginasForced Smoking Stories I'Ve CollectedErnesto PazAinda não há avaliações
- Grade 9 IGCSE DRUGS ResourceDocumento18 páginasGrade 9 IGCSE DRUGS ResourceAnushka YadavAinda não há avaliações
- Vaping Effects and StatisticsDocumento5 páginasVaping Effects and StatisticsKanmaneAinda não há avaliações
- Principles of Drug Use During LactationDocumento18 páginasPrinciples of Drug Use During LactationMade SuryaAinda não há avaliações
- Quit SmokingDocumento44 páginasQuit SmokingTbwc UmiAinda não há avaliações
- Alkaloids Physiological EffectsDocumento25 páginasAlkaloids Physiological EffectsGiang Lam100% (1)
- Project Report On Drugs AddictionDocumento6 páginasProject Report On Drugs Addictionapi-246586162Ainda não há avaliações
- Cigarette Smoking Outline and EssayDocumento2 páginasCigarette Smoking Outline and Essaygie100% (1)
- Signals 2020 Tabex Update 02Documento5 páginasSignals 2020 Tabex Update 02Na MoAinda não há avaliações
- Tobacco and Vaping WorksheetDocumento8 páginasTobacco and Vaping Worksheetyork.yfzhouAinda não há avaliações
- Gangguan Yang Berhubungan Dengan Zat (Substance Abuse)Documento44 páginasGangguan Yang Berhubungan Dengan Zat (Substance Abuse)Mohamad Arifudin syahAinda não há avaliações
- Takashi NagaiDocumento11 páginasTakashi Nagaierni pabateAinda não há avaliações
- Bupropion and Other Non-Nicotine PharmacotherapiesDocumento3 páginasBupropion and Other Non-Nicotine PharmacotherapiesEstigma Universidad Del RosarioAinda não há avaliações
- Bidee Vs CigaretteDocumento6 páginasBidee Vs Cigarettescribd_427Ainda não há avaliações
- Botanical Pesticidesand Their Modeof ActionDocumento28 páginasBotanical Pesticidesand Their Modeof ActionChileshe SimonAinda não há avaliações
- Big Picture: AddictionDocumento16 páginasBig Picture: AddictionWellcome Trust100% (1)
- Nicotine and Its Overdose EffectsDocumento4 páginasNicotine and Its Overdose EffectsahmedaliAinda não há avaliações
- 2011 Mini Mock Trial Materials - FinalDocumento59 páginas2011 Mini Mock Trial Materials - FinalJacob Van BaalenAinda não há avaliações
- E-Cigarettes A 1-Way Street To Traditional Smoking and Nicotine Addiction For YouthDocumento4 páginasE-Cigarettes A 1-Way Street To Traditional Smoking and Nicotine Addiction For YouthAsd EfgAinda não há avaliações
- Drug Addiction: Biology ProjectDocumento9 páginasDrug Addiction: Biology Projectalan spacaerAinda não há avaliações
- Smoking EffectsDocumento7 páginasSmoking EffectstsikiAinda não há avaliações
- Effects of Tobacco Smoking and AlcoholDocumento13 páginasEffects of Tobacco Smoking and AlcoholRubiya TufailAinda não há avaliações
- Ieltsfever Academic Reading Practice Test 3 PDFDocumento10 páginasIeltsfever Academic Reading Practice Test 3 PDFchandaAinda não há avaliações