Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Otoacoustic Emissions From MedscapeDocumento5 páginasOtoacoustic Emissions From MedscapeMin-Joo Esther ParkAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Schizophrenia Overview: Irving Kuo, M.D. Central Arkansas Veterans Healthcare SystemDocumento31 páginasSchizophrenia Overview: Irving Kuo, M.D. Central Arkansas Veterans Healthcare SystemMin-Joo Esther ParkAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- ShockDocumento36 páginasShockMin-Joo Esther ParkAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Iv. Pathophysiology 1. Schematic Diagram Book Based Pathophysiology: Precipitating/Modifiable Factors Non Modifiable / Predisposing FactorsDocumento2 páginasIv. Pathophysiology 1. Schematic Diagram Book Based Pathophysiology: Precipitating/Modifiable Factors Non Modifiable / Predisposing Factorsikemas67% (6)
- Best Study Guide For ObgynDocumento38 páginasBest Study Guide For ObgynMin-Joo Esther Park100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- AAP Webinar UTI Roberts FinalDocumento44 páginasAAP Webinar UTI Roberts FinalMin-Joo Esther ParkAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Iv. Pathophysiology 1. Schematic Diagram Book Based Pathophysiology: Precipitating/Modifiable Factors Non Modifiable / Predisposing FactorsDocumento2 páginasIv. Pathophysiology 1. Schematic Diagram Book Based Pathophysiology: Precipitating/Modifiable Factors Non Modifiable / Predisposing Factorsikemas67% (6)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Treatment of Children: With Acute Amoebic DysenteryDocumento3 páginasTreatment of Children: With Acute Amoebic DysenteryMin-Joo Esther ParkAinda não há avaliações
- Salivary Gland PathologyDocumento29 páginasSalivary Gland PathologyDhina IrhazAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Neonatal Sepsis and Recent Challenges: Mohammad Khasswneh, MD Assistant Professor of Pediatrics JustDocumento47 páginasNeonatal Sepsis and Recent Challenges: Mohammad Khasswneh, MD Assistant Professor of Pediatrics JustMin-Joo Esther ParkAinda não há avaliações
- Fever: Pathogenesis and TreatmentDocumento31 páginasFever: Pathogenesis and TreatmentMin-Joo Esther ParkAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- General Nursing Science 1 2020 PDFDocumento95 páginasGeneral Nursing Science 1 2020 PDFRicardo DomingosAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Hypertension Clinical Study PDFDocumento42 páginasHypertension Clinical Study PDFsertti23Ainda não há avaliações
- Risk Factors Pathophysiology and Management of HypertensionDocumento13 páginasRisk Factors Pathophysiology and Management of HypertensionDominggas RusunwullyAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Overview of Hypertension in AdultsDocumento27 páginasOverview of Hypertension in AdultsMedByteAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Nutrition Care Process Related To HypertensionDocumento22 páginasThe Nutrition Care Process Related To HypertensionLARAIB SAJIDAinda não há avaliações
- Seminar On Nightingales Theory Subject ADocumento7 páginasSeminar On Nightingales Theory Subject AShubhankar KatariyaAinda não há avaliações
- Case Study 2 2018Documento6 páginasCase Study 2 2018jigsawAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Evaluation of The Effects of Music Therapy Using Todi Raga of Hindustani Classical Music On Blood Pressure, Pulse Rate and Respiratory Rate of Healthy Elderly MenDocumento8 páginasEvaluation of The Effects of Music Therapy Using Todi Raga of Hindustani Classical Music On Blood Pressure, Pulse Rate and Respiratory Rate of Healthy Elderly MenAprilinda SafitriAinda não há avaliações
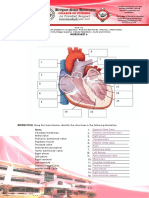
- Cardiovascular WorksheetDocumento9 páginasCardiovascular WorksheetPANGPANGDEO Shanne Delle B.Ainda não há avaliações
- Hypertension PDFDocumento50 páginasHypertension PDFMochamad Ali Rosadi100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- High Blood PressureDocumento9 páginasHigh Blood PressureshashidharanAinda não há avaliações
- NICE CG 127 HypertensionDocumento328 páginasNICE CG 127 Hypertensionreiv4xAinda não há avaliações
- CVD Case StudyDocumento9 páginasCVD Case Studyapi-346620455100% (3)
- Cardiac Output, Blood Flow, and Blood PressureDocumento69 páginasCardiac Output, Blood Flow, and Blood PressureUzma KhanAinda não há avaliações
- Specific Diseases: Special PathologyDocumento19 páginasSpecific Diseases: Special Pathologyhumag143Ainda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- كتاب التمريض الجديد2022Documento206 páginasكتاب التمريض الجديد2022mohamed mohamedAinda não há avaliações
- Overview of Hypertension in Adults - UpToDate PDFDocumento62 páginasOverview of Hypertension in Adults - UpToDate PDFIzamar RomeroAinda não há avaliações
- Genetics of HypertensionDocumento8 páginasGenetics of HypertensionBounab LyamineAinda não há avaliações
- Project On Exercise and High Blood PressureDocumento22 páginasProject On Exercise and High Blood Pressureneba derrickAinda não há avaliações
- HypertensionDocumento26 páginasHypertensionAhmad Al-SarrafAinda não há avaliações
- Yoga and High Blood Pressure Hypertension 2 AVonCammererDocumento9 páginasYoga and High Blood Pressure Hypertension 2 AVonCammererAndrea Van RankinAinda não há avaliações
- Clinical Pharmacy: 4 ProfessionalDocumento300 páginasClinical Pharmacy: 4 ProfessionalMobeen AhmedAinda não há avaliações
- Metabolic Syndrome DiseasesDocumento8 páginasMetabolic Syndrome DiseasesMahmoud SelimAinda não há avaliações
- Hypertension Case StudyDocumento15 páginasHypertension Case Studyjigsaw100% (1)
- Sodium and Your Health: Rebecca Burson, M.D., M.P.H. Assistant Clinical Faculty at Texas A&M FM ResidencyDocumento39 páginasSodium and Your Health: Rebecca Burson, M.D., M.P.H. Assistant Clinical Faculty at Texas A&M FM ResidencyAshley Judd Mallonga BeranAinda não há avaliações
- HypertensionDocumento217 páginasHypertensionFeli Deanne M. GorechoAinda não há avaliações
- Hypertension in ChildrenDocumento6 páginasHypertension in ChildrenlebellexiAinda não há avaliações
- Wardlaws Perspectives in Nutrition 10Th Ed Edition Byrd Bredbenner All ChapterDocumento67 páginasWardlaws Perspectives in Nutrition 10Th Ed Edition Byrd Bredbenner All Chapterlona.robinson229100% (5)
- Types of Hypertension Pathophysiology Aims and Objectives Drugs Mechanism of Action Literature Review Materials AND MethodsDocumento14 páginasTypes of Hypertension Pathophysiology Aims and Objectives Drugs Mechanism of Action Literature Review Materials AND MethodsMaram RanadeepAinda não há avaliações
- Aha Guidelinedriven Management of Hypertension An Evidencebased UpdateDocumento56 páginasAha Guidelinedriven Management of Hypertension An Evidencebased UpdateNanda Gopal Reddy AnamAinda não há avaliações