Você também pode gostar
- Leukemia: Candra WibowoDocumento89 páginasLeukemia: Candra WibowoputusanggraAinda não há avaliações
- Aplastic AnemiaDocumento7 páginasAplastic Anemianeil052288% (8)
- Immune System Docs 2019Documento13 páginasImmune System Docs 2019David DavidAinda não há avaliações
- ChemotherapyDocumento30 páginasChemotherapyHealth Education Library for People100% (3)
- Luther's Ninety Five ThesesDocumento2 páginasLuther's Ninety Five Thesesadrianna.ilyAinda não há avaliações
- Genes For All DisordersDocumento86 páginasGenes For All Disordersvenkyreddy97Ainda não há avaliações
- Anatomy and Physiology of PlacentaDocumento5 páginasAnatomy and Physiology of PlacentaAmuAinda não há avaliações
- Chromosome Abnormalities and Sex DeterminationDocumento43 páginasChromosome Abnormalities and Sex DeterminationprasadbheemAinda não há avaliações
- Immune System Review QuestionsDocumento2 páginasImmune System Review Questionsapi-524061079Ainda não há avaliações
- Abdominal Wall DefectsDocumento8 páginasAbdominal Wall Defectsهلا دلبحAinda não há avaliações
- FMS 1 - Week 7 Tutorial 1 LO PDFDocumento17 páginasFMS 1 - Week 7 Tutorial 1 LO PDFAprillia AlmaasAinda não há avaliações
- Medcosmos Surgery: Spleen MCQDocumento19 páginasMedcosmos Surgery: Spleen MCQSajag GuptaAinda não há avaliações
- Blood DisordersDocumento72 páginasBlood DisordersAngel Bar100% (1)
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocumento27 páginasHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanAinda não há avaliações
- 1st Trimester BleedingDocumento67 páginas1st Trimester BleedingRaiden VizcondeAinda não há avaliações
- Transfusion For ChildrenDocumento5 páginasTransfusion For ChildrenKristine Mae AbrasaldoAinda não há avaliações
- LeukemiaDocumento51 páginasLeukemiaCres Padua QuinzonAinda não há avaliações
- EndocrinologyDocumento37 páginasEndocrinologyKochaMsangiAinda não há avaliações
- Hisprung DiseaseDocumento12 páginasHisprung DiseaseEky Madyaning NastitiAinda não há avaliações
- Hirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshDocumento48 páginasHirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshArchana Mahata100% (1)
- Embryo Lab Exercise 1Documento7 páginasEmbryo Lab Exercise 1Karmina Santos100% (1)
- 5 - Tissue Healing and RepairDocumento56 páginas5 - Tissue Healing and Repairzlaticab4246Ainda não há avaliações
- 01 - Signs and Symptoms of Git DisordersDocumento51 páginas01 - Signs and Symptoms of Git DisordersRere AnugrahAinda não há avaliações
- Breast Disorder: by DR - Wael MetwalyDocumento7 páginasBreast Disorder: by DR - Wael MetwalyhasebeAinda não há avaliações
- Male Hypogonadism - Jarunee - ppt2085280427Documento27 páginasMale Hypogonadism - Jarunee - ppt2085280427Melissa Aina Mohd YusofAinda não há avaliações
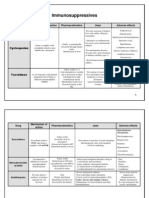
- 1 - Immuno Tables1Documento4 páginas1 - Immuno Tables1Urugonda VenumadhavAinda não há avaliações
- The HeartDocumento42 páginasThe HeartJerilee SoCute WattsAinda não há avaliações
- Cirrhosis of The LiverDocumento4 páginasCirrhosis of The LiverDaphineAinda não há avaliações
- 5 Acute Cholecystitis - Libre PathologyDocumento5 páginas5 Acute Cholecystitis - Libre Pathologyfado100% (1)
- Kaposi SarcomaDocumento34 páginasKaposi SarcomaDerri HafaAinda não há avaliações
- Anaemia PDFDocumento105 páginasAnaemia PDFzafar iqbalAinda não há avaliações
- Gametogenesis and Fertilization - Bio 30 PDFDocumento2 páginasGametogenesis and Fertilization - Bio 30 PDFJoseph Paguio100% (1)
- Intestinal Obstruction in Paediatrics - James GathogoDocumento21 páginasIntestinal Obstruction in Paediatrics - James GathogoMalueth Angui100% (1)
- Leukemia (Suzy)Documento23 páginasLeukemia (Suzy)medo2002alfadaliAinda não há avaliações
- P2 Myeloproliferative Disorders (AML, CML, and ALL)Documento8 páginasP2 Myeloproliferative Disorders (AML, CML, and ALL)rixibi1180Ainda não há avaliações
- Week 05. Acute LeukemiasDocumento26 páginasWeek 05. Acute LeukemiasAshley ArnoldAinda não há avaliações
- Hematology Review 2021-2Documento142 páginasHematology Review 2021-2Maram AbdullahAinda não há avaliações
- Keganasan HematologiDocumento26 páginasKeganasan HematologiRizzal Selviyana SuhardiAinda não há avaliações
- Pathology Lecture 2nd CourseDocumento128 páginasPathology Lecture 2nd CourseAbdullah EssaAinda não há avaliações
- Haematopathology 3:: Leucocytosis/LeucopeniaDocumento113 páginasHaematopathology 3:: Leucocytosis/LeucopeniaarwaAinda não há avaliações
- WaloDocumento67 páginasWaloyepAinda não há avaliações
- Leukocyte Total and Differential CountDocumento37 páginasLeukocyte Total and Differential CountHend HamedAinda não há avaliações
- Acute Myeloblastic Leukemia AML: Dr. Amged H.AbdelrhmanDocumento23 páginasAcute Myeloblastic Leukemia AML: Dr. Amged H.Abdelrhmanد. أمجد حسين عبد الرحمنAinda não há avaliações
- Acute Leukemia: Thirunavukkarasu MurugappanDocumento22 páginasAcute Leukemia: Thirunavukkarasu MurugappanFelix Allen100% (1)
- 01 Hemotological MalignaciesDocumento92 páginas01 Hemotological MalignaciesmarrymbigiAinda não há avaliações
- Leukaemia: Definition: Leukemia Is A Malignant Disease of The Hematopoietic System (Blood Forming Cells)Documento16 páginasLeukaemia: Definition: Leukemia Is A Malignant Disease of The Hematopoietic System (Blood Forming Cells)Arnab Ghosh100% (1)
- ML: AML Without Maturation M2: AML With Maturation M3: M4: M5: M6Documento8 páginasML: AML Without Maturation M2: AML With Maturation M3: M4: M5: M6Isak ShatikaAinda não há avaliações
- Myeloproliferative DisorderDocumento36 páginasMyeloproliferative DisorderKalpana ShahAinda não há avaliações
- 4b TUMOR JAR RetikuloendotelialAAADocumento98 páginas4b TUMOR JAR RetikuloendotelialAAARyo RyozAinda não há avaliações
- CML, CLLDocumento118 páginasCML, CLLMunesh SherawatAinda não há avaliações
- Acute and Chronic Leukemia FinalDocumento68 páginasAcute and Chronic Leukemia FinalHannah LeiAinda não há avaliações
- ' / 5 Introduction of LeukemiasaDocumento37 páginas' / 5 Introduction of LeukemiasashaikhaboausaibaAinda não há avaliações
- The LeukemiasDocumento52 páginasThe Leukemiasمصطفي خندقاوي100% (1)
- Acute Leukemia: DR Rosline Hassan Hematology Department School of Medical Sciences USMDocumento52 páginasAcute Leukemia: DR Rosline Hassan Hematology Department School of Medical Sciences USMJamilAinda não há avaliações
- Hematologic Pathology p65-87Documento23 páginasHematologic Pathology p65-87zeroun24100% (1)
- Chronic Myeloid LeukaemiaDocumento27 páginasChronic Myeloid Leukaemiaنواف الزهرانيAinda não há avaliações
- Hematology IIDocumento26 páginasHematology IIpieterinpretoria391Ainda não há avaliações
- Acute Leukemia: David Lee, MD, FRCPCDocumento31 páginasAcute Leukemia: David Lee, MD, FRCPCfranzzjosefAinda não há avaliações
- Acute Leukemia: Thuvija Darshini Govindev 0902005194Documento16 páginasAcute Leukemia: Thuvija Darshini Govindev 0902005194Thuvija DarshiniAinda não há avaliações
- HemoglobinopathiesDocumento10 páginasHemoglobinopathiespriscillaAinda não há avaliações
- Key Topics ENTDocumento375 páginasKey Topics ENTanas_marzoukAinda não há avaliações
- Anesthesia MedicationsDocumento1 páginaAnesthesia MedicationsMedShare0% (1)
- ENTDocumento40 páginasENTwhoosh2008Ainda não há avaliações
- Twinning HandbookDocumento11 páginasTwinning HandbookpriscillaAinda não há avaliações
- Obstetrics Last Moment RevisionsDocumento9 páginasObstetrics Last Moment RevisionspriscillaAinda não há avaliações
- Essential Surface & Related Anatomy For Clinical Practice: Compiled by DR Robert Whitaker & DR Jessica WhiteDocumento18 páginasEssential Surface & Related Anatomy For Clinical Practice: Compiled by DR Robert Whitaker & DR Jessica WhiteabinthevarmadomAinda não há avaliações
- °Âõπ∑Ÿ¡∫√‘‡«≥™Àõß∑Âõß °"√Æ‘‡§√"-Àåªí≠À"°Âõπ∑Ÿ¡∫√‘‡«≥™Àõß∑Âõß„Π‡¥Á° ·Π«∑"ß°"√´-°ª√-«-Μ‘·≈-Μ√«®√À"ß°"¬ ‡§√◊Ëõß¡◊Õ ◊∫§Âπ∑"ß√-ß '«‘∑¬"·≈-‡«™»" Μ√Å𑫇§≈'¬√Å Tumor Markers °"√¬◊Π¬-Π°"√«‘Π‘®©-¬¢-Èπ Ÿ¥∑Â"¬Documento40 páginas°Âõπ∑Ÿ¡∫√‘‡«≥™Àõß∑Âõß °"√Æ‘‡§√"-Àåªí≠À"°Âõπ∑Ÿ¡∫√‘‡«≥™Àõß∑Âõß„Π‡¥Á° ·Π«∑"ß°"√´-°ª√-«-Μ‘·≈-Μ√«®√À"ß°"¬ ‡§√◊Ëõß¡◊Õ ◊∫§Âπ∑"ß√-ß '«‘∑¬"·≈-‡«™»" Μ√Å𑫇§≈'¬√Å Tumor Markers °"√¬◊Π¬-Π°"√«‘Π‘®©-¬¢-Èπ Ÿ¥∑Â"¬priscillaAinda não há avaliações
- Hematopoietic+Stem Cell+TransplantationDocumento14 páginasHematopoietic+Stem Cell+TransplantationFabLab EIUAinda não há avaliações
- Kriteria Remisi AmlDocumento6 páginasKriteria Remisi AmldjebrutAinda não há avaliações
- 04.analysis of GATA1 Mutations and Leukemogenesis in Newborns With Down SyndromeDocumento9 páginas04.analysis of GATA1 Mutations and Leukemogenesis in Newborns With Down SyndromeCristi Daniel NeagoeAinda não há avaliações
- GSIS Case DigestDocumento17 páginasGSIS Case DigestMaria Cristina Martinez100% (1)
- Wood-2016-Cytometry Part B: Clinical CytometryDocumento7 páginasWood-2016-Cytometry Part B: Clinical CytometryWalter Jhon Delgadillo AroneAinda não há avaliações
- BloodDocumento142 páginasBloodChelleyOllitroAinda não há avaliações
- Proceeding Ilmu KesehatanDocumento183 páginasProceeding Ilmu KesehatanIim Rimba100% (1)
- Germany CancerDocumento6 páginasGermany CancerDaniel VenablesAinda não há avaliações
- Safety Data Sheet: Chevron (Malaysia) Unleaded GasolineDocumento12 páginasSafety Data Sheet: Chevron (Malaysia) Unleaded GasolineaminAinda não há avaliações
- CR1 Natharina Yolanda 27.01Documento48 páginasCR1 Natharina Yolanda 27.01sugarp_3Ainda não há avaliações
- Myeloproliferative DisorderDocumento36 páginasMyeloproliferative DisorderKalpana ShahAinda não há avaliações
- Leukemia PDFDocumento63 páginasLeukemia PDFErfan Syahid AzhariAinda não há avaliações
- Olfu Finals BSN ReviewerDocumento101 páginasOlfu Finals BSN ReviewerEdnalyn QuimboAinda não há avaliações
- Case Report: A Child With Acute Lymphocytic Leukaemia: R Bonanthaya, L.Appaji and K.C.LakshmaiahDocumento2 páginasCase Report: A Child With Acute Lymphocytic Leukaemia: R Bonanthaya, L.Appaji and K.C.LakshmaiahKAREN YULIETH ANDRADE RAMÍREZAinda não há avaliações
- CALGB Schema FinalDocumento1 páginaCALGB Schema FinalMohamed MahmoudAinda não há avaliações
- AML Landscape in Asia-Pacific - 2021Documento9 páginasAML Landscape in Asia-Pacific - 2021fikriafisAinda não há avaliações
- Chemotherapy-Induced Secondary MalignanciesDocumento9 páginasChemotherapy-Induced Secondary MalignanciesSupandy HasanAinda não há avaliações
- Seminar: Florent Malard, Mohamad MohtyDocumento17 páginasSeminar: Florent Malard, Mohamad MohtyStephania SandovalAinda não há avaliações
- MRCP 2 Practice Questions Book.3Documento166 páginasMRCP 2 Practice Questions Book.3iban100% (1)
- April 20, 2015 - RATIODocumento23 páginasApril 20, 2015 - RATIOLouie BelloAinda não há avaliações
- Medical Abbreviations GlossaryDocumento15 páginasMedical Abbreviations Glossarydbryant0101100% (9)
- CMML Final 1Documento39 páginasCMML Final 1lakshmi krishnaAinda não há avaliações
- 200 Articles Ebook Thecureforcancer-Min PDFDocumento439 páginas200 Articles Ebook Thecureforcancer-Min PDFVictor DaetAinda não há avaliações
- Hematological Disorders in Geriatric PatientsDocumento15 páginasHematological Disorders in Geriatric PatientsChompz MuMu PhantarsAinda não há avaliações
- The Electronic Version of The Virtual Community by Howard RheingoldDocumento272 páginasThe Electronic Version of The Virtual Community by Howard RheingoldMárcia Hellen SantosAinda não há avaliações
- 06 Clinical Pathology MCQs With Answers 1Documento29 páginas06 Clinical Pathology MCQs With Answers 1Habib UllahAinda não há avaliações
- Oncology and Hematology Cheat SheetDocumento4 páginasOncology and Hematology Cheat Sheetpieterinpretoria391100% (1)
- Lorenzo VS Gsis and DepedDocumento28 páginasLorenzo VS Gsis and DepedViolet BlueAinda não há avaliações
- Blood and Clotting FactorsDocumento34 páginasBlood and Clotting FactorsAnand KasiAinda não há avaliações
- White Blood Cell DisordersDocumento9 páginasWhite Blood Cell DisordersDocAxi Maximo Jr AxibalAinda não há avaliações