Você também pode gostar
- Proses Persalinan Dan Konsep DasarDocumento31 páginasProses Persalinan Dan Konsep DasarShella Ramashanti100% (1)
- CBD Hiperemis GravidarumDocumento32 páginasCBD Hiperemis GravidarumFifit SiePutry BintaNgnya KudaciAinda não há avaliações
- Refreshing Inersia UteriDocumento31 páginasRefreshing Inersia UteriDera Seta SaputriAinda não há avaliações
- Dasar-Dasar Obstetrik: Tjokorda Gde Agung SuwardewaDocumento36 páginasDasar-Dasar Obstetrik: Tjokorda Gde Agung SuwardewaD'nesh ReYyAinda não há avaliações
- The Occiput Posterior Fetus: Oleh: Wiliyanto. Wijaya Pembimbing: Dr. Ims Murah Manoe, Spog (K)Documento24 páginasThe Occiput Posterior Fetus: Oleh: Wiliyanto. Wijaya Pembimbing: Dr. Ims Murah Manoe, Spog (K)Eka KurniatiAinda não há avaliações
- KB HormonalDocumento65 páginasKB Hormonaljessica_siahaan_1Ainda não há avaliações
- PartografDocumento31 páginasPartografrovi wilmanAinda não há avaliações
- Solusio Plasenta: M.Thamrin TanjungDocumento20 páginasSolusio Plasenta: M.Thamrin Tanjungashry909Ainda não há avaliações
- Recurrent Pregnancy LossDocumento19 páginasRecurrent Pregnancy LossSean NamAinda não há avaliações
- Amenorea Primer: A.A.N AnantasikaDocumento49 páginasAmenorea Primer: A.A.N AnantasikaninachayankAinda não há avaliações
- Physiology of Labor: Ribkhi Amalia Putri Ganot SumulyoDocumento48 páginasPhysiology of Labor: Ribkhi Amalia Putri Ganot SumulyoImelda AtikaAinda não há avaliações
- Mnemonic Vacum Dan Forcep NewDocumento2 páginasMnemonic Vacum Dan Forcep NewsinggehAinda não há avaliações
- Janica E. Walden, MD Neuroradiology University of North CarolinaDocumento21 páginasJanica E. Walden, MD Neuroradiology University of North CarolinaBilly ChietraAinda não há avaliações
- Adri - Pertumbuhan Janin TerhambatDocumento38 páginasAdri - Pertumbuhan Janin TerhambatMedika PutriAinda não há avaliações
- Tugas SC Vs Histerotomi Vs Laparotomi Ambil Anak Aji PatriajatiDocumento3 páginasTugas SC Vs Histerotomi Vs Laparotomi Ambil Anak Aji PatriajatiAji PatriajatiAinda não há avaliações
- Amnioinfusion - LEODocumento16 páginasAmnioinfusion - LEOtapayanaAinda não há avaliações
- Referat ObsgynDocumento15 páginasReferat ObsgynDevi Melissa RiupassaAinda não há avaliações
- Lapkas Hymen ImperforataDocumento27 páginasLapkas Hymen ImperforataKhairida Hafni LbsAinda não há avaliações
- Gannguan PubertasDocumento56 páginasGannguan PubertasAde Yosdi PutraAinda não há avaliações
- Sectio CaesareaDocumento13 páginasSectio CaesareaDavid ZamrilAinda não há avaliações
- Overview Antenatal CareDocumento54 páginasOverview Antenatal CareRizky Dwidya AmirtasariAinda não há avaliações
- 7.ketuban Pecah Dini-PromDocumento21 páginas7.ketuban Pecah Dini-PromabcdshAinda não há avaliações
- Fisiologi Siklus Haid (DR - Kanadi SumaprajaDocumento70 páginasFisiologi Siklus Haid (DR - Kanadi SumaprajaIntan DhyaksariAinda não há avaliações
- Amenore PrimerDocumento40 páginasAmenore PrimerMaksum Pandelima0% (1)
- Perdarahan Pasca Persalinan: Sources: William, Obstetrics Illustrated, Buku Merah, Panduan Pelayanan IbuDocumento25 páginasPerdarahan Pasca Persalinan: Sources: William, Obstetrics Illustrated, Buku Merah, Panduan Pelayanan IbuFirdinia Gafuri DohamidAinda não há avaliações
- Dr. Ilham - AFLP - ISSHP 2017 BandungDocumento40 páginasDr. Ilham - AFLP - ISSHP 2017 BandungMegaSariDewiAinda não há avaliações
- Anatomy of The Lower Urinary TractDocumento24 páginasAnatomy of The Lower Urinary Tractمحمد حميدانAinda não há avaliações
- Anatomi PanggulDocumento34 páginasAnatomi PanggulKhodijahAinda não há avaliações
- Kehamilan MultifetusDocumento29 páginasKehamilan MultifetusintanpurnAinda não há avaliações
- Induction of Labor With Oxytocin - UpToDateDocumento54 páginasInduction of Labor With Oxytocin - UpToDateJhoseline CamposAinda não há avaliações
- Weekly Report 13 - 19 2017Documento11 páginasWeekly Report 13 - 19 2017Sitha MahendrataAinda não há avaliações
- Kista BartoliniDocumento24 páginasKista BartoliniTri HariadyAinda não há avaliações
- Trial of Labor After Cesarean (TOLAC)Documento16 páginasTrial of Labor After Cesarean (TOLAC)Ricko Handen UriaAinda não há avaliações
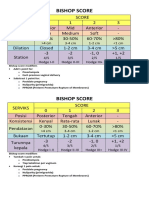
- Bishop ScoreDocumento2 páginasBishop ScoreRskia Sadewwa Yogyakarta100% (1)
- Anatomi Panggul, Sistem Hormonal Dan Konsepsi: Ns. Dina Mariyana.,S.KepDocumento56 páginasAnatomi Panggul, Sistem Hormonal Dan Konsepsi: Ns. Dina Mariyana.,S.KepAna KareniaAinda não há avaliações
- Referat Persalinan Preterm - Hendri AntoniusDocumento31 páginasReferat Persalinan Preterm - Hendri AntoniusHendri Antonius100% (1)
- Anindya Widhi C Abses BartholiniDocumento28 páginasAnindya Widhi C Abses BartholiniAnindya Widhi CantikaAinda não há avaliações
- Perdarahan Uterus AbnormalDocumento15 páginasPerdarahan Uterus Abnormalarfiah100% (1)
- Penelitian Urogin AGENESIS VAGINADocumento29 páginasPenelitian Urogin AGENESIS VAGINAyulipongaAinda não há avaliações
- Pengantar Keganasan Ginekologi DR Hardjono SpogDocumento47 páginasPengantar Keganasan Ginekologi DR Hardjono SpogMuhammad SidiqAinda não há avaliações
- Placental PathologyDocumento465 páginasPlacental PathologyOana Roxana PuscasAinda não há avaliações
- Skor Bishop, Profil Biofisik Janin, Dan Tanda Kehamilan Post-TermDocumento9 páginasSkor Bishop, Profil Biofisik Janin, Dan Tanda Kehamilan Post-TermMuhammad KhoiruddinAinda não há avaliações
- Materi Dr. DalimanDocumento54 páginasMateri Dr. DalimanSamuel Xaverius ChristyantAinda não há avaliações
- B Lynch SutureDocumento20 páginasB Lynch SutureRyan Ilham100% (1)
- Omphalocele Omphalocele: Perceptor: DR. AMRAN SINAGA, SP.B AUTHOR: Ida Ayu Ratna W, S.Ked (G1A214018)Documento17 páginasOmphalocele Omphalocele: Perceptor: DR. AMRAN SINAGA, SP.B AUTHOR: Ida Ayu Ratna W, S.Ked (G1A214018)Rully Riyan DikaAinda não há avaliações
- 04 Kelainan Bawaan Kasus Uroginekologi Dan Pengobatan SaatDocumento23 páginas04 Kelainan Bawaan Kasus Uroginekologi Dan Pengobatan SaatHerdinda Erudite Rizkinya100% (1)
- Mioma UteriDocumento6 páginasMioma UteriVina Hardianti100% (1)
- Implantation and Development Placenta Part 2Documento36 páginasImplantation and Development Placenta Part 2Tengku Chairannisa PutriAinda não há avaliações
- HELLP and AFLP PDFDocumento5 páginasHELLP and AFLP PDFDesyHandayaniAinda não há avaliações
- Bedah ObstetriDocumento21 páginasBedah ObstetriWinda LiraAinda não há avaliações
- Compound Presentation: Asheber Gaym M.D. January 2009Documento6 páginasCompound Presentation: Asheber Gaym M.D. January 2009Israel WoseneAinda não há avaliações
- CH 5 Implantation, Placental Dev (Part1)Documento36 páginasCH 5 Implantation, Placental Dev (Part1)Tengku Chairannisa PutriAinda não há avaliações
- REFERAT - Ppt.solusio Plasenta ItaDocumento18 páginasREFERAT - Ppt.solusio Plasenta ItaMochammad Adam EldiAinda não há avaliações
- Mola Hidatidosa1 PDFDocumento8 páginasMola Hidatidosa1 PDFKoas PatoAinda não há avaliações
- Acute Abdominal Pain in Pregnancy: Diagnosis and Management Conservative vs. SurgicalDocumento73 páginasAcute Abdominal Pain in Pregnancy: Diagnosis and Management Conservative vs. SurgicalIgnatov OanaAinda não há avaliações
- OBGYN Vaginal Delivery DikaDocumento10 páginasOBGYN Vaginal Delivery DikaOnyedika EgbujoAinda não há avaliações
- Obgyn SL1Documento39 páginasObgyn SL1mustafe omarAinda não há avaliações
- Management of LabourDocumento16 páginasManagement of LabourAlbert MusinguziAinda não há avaliações
- Stages of Labor NSG MGTDocumento3 páginasStages of Labor NSG MGTMelDred Cajes BolandoAinda não há avaliações
- Stages of LaborDocumento5 páginasStages of LaborL Rean Carmelle MAGALLONES100% (1)
- Pedoman DMDocumento32 páginasPedoman DMPon_Zi_cuteAinda não há avaliações
- 5f97a6778781eDocumento1 página5f97a6778781eAhmed MawardiAinda não há avaliações
- Ahmed MawardiDocumento1 páginaAhmed MawardiAhmed MawardiAinda não há avaliações
- Embedded and Impacted TeethDocumento2 páginasEmbedded and Impacted TeethAhmed MawardiAinda não há avaliações
- Pedoman DMDocumento32 páginasPedoman DMPon_Zi_cuteAinda não há avaliações
- 5f97a6778781eDocumento1 página5f97a6778781eAhmed MawardiAinda não há avaliações
- CHT Hfa Boys P 2 5Documento1 páginaCHT Hfa Boys P 2 5Dillon WilsonAinda não há avaliações
- Presentation 1Documento2 páginasPresentation 1Ahmed MawardiAinda não há avaliações
- Ahmed Mawardi: ObjectiveDocumento1 páginaAhmed Mawardi: ObjectiveAhmed MawardiAinda não há avaliações
- Treatment of Seborrheic Dermatitis PDFDocumento7 páginasTreatment of Seborrheic Dermatitis PDFAhmed MawardiAinda não há avaliações
- Billing Statement 1Documento3 páginasBilling Statement 1Ahmed MawardiAinda não há avaliações
- Japanese EncephalitisDocumento9 páginasJapanese EncephalitisAhmed Mawardi0% (1)
- Toefl Answer Sheet For Free Test: NoteDocumento4 páginasToefl Answer Sheet For Free Test: NoteAhmed MawardiAinda não há avaliações
- Treatment of Seborrheic Dermatitis PDFDocumento7 páginasTreatment of Seborrheic Dermatitis PDFAhmed MawardiAinda não há avaliações
- Three Etiologic Facets of Dandruff and Seborrheic Dermatitis: Malassezia Fungi, Sebaceous Lipids, and Individual SensitivityDocumento3 páginasThree Etiologic Facets of Dandruff and Seborrheic Dermatitis: Malassezia Fungi, Sebaceous Lipids, and Individual SensitivityAhmed MawardiAinda não há avaliações
- ADocumento5 páginasAAhmed MawardiAinda não há avaliações
- A Practical Guide To Scalp DisorderDocumento5 páginasA Practical Guide To Scalp DisorderAhmed MawardiAinda não há avaliações
- ADocumento4 páginasAAhmed MawardiAinda não há avaliações
- 21 PDFDocumento39 páginas21 PDFAhmed MawardiAinda não há avaliações
- 21 PDFDocumento39 páginas21 PDFAhmed MawardiAinda não há avaliações
- A Comparison of Hair Quality and Cosmetic AcceptanceDocumento4 páginasA Comparison of Hair Quality and Cosmetic AcceptanceAhmed MawardiAinda não há avaliações
- Dandruff Has An Altered Stratum CorneumDocumento7 páginasDandruff Has An Altered Stratum CorneumAhmed MawardiAinda não há avaliações
- Emd166 Slide Shock-1Documento53 páginasEmd166 Slide Shock-1THuthi MUktiAinda não há avaliações
- 2086 Genome FinalDocumento1 página2086 Genome FinalAhmed MawardiAinda não há avaliações
- ADocumento5 páginasAAhmed MawardiAinda não há avaliações
- Scaling Up Nutrition A Framework For ActionDocumento1 páginaScaling Up Nutrition A Framework For ActionAhmed MawardiAinda não há avaliações
- Katz and Fischer - The Revised International Health RegulationsDocumento18 páginasKatz and Fischer - The Revised International Health RegulationsAhmed MawardiAinda não há avaliações
- Cancer Epidemiology: Hematology Oncology Division Child Health Departement - Universty of Sumatera UtaraDocumento27 páginasCancer Epidemiology: Hematology Oncology Division Child Health Departement - Universty of Sumatera Utaraparik2321Ainda não há avaliações
- Presentation 1Documento4 páginasPresentation 1Ahmed MawardiAinda não há avaliações
- FM k36 Prenatal CareDocumento33 páginasFM k36 Prenatal CareAhmed MawardiAinda não há avaliações
- Postpartal CareDocumento48 páginasPostpartal CareGladys YaresAinda não há avaliações
- Review Research Paper Medico-Legal Aspect of Pregnancy and Delivery: A Critical Case ReviewDocumento7 páginasReview Research Paper Medico-Legal Aspect of Pregnancy and Delivery: A Critical Case ReviewVlynAinda não há avaliações
- Sentinel Event PolicyDocumento6 páginasSentinel Event PolicyAnne Marjorie Futalan100% (1)
- Singapore Airlines V NLRCDocumento4 páginasSingapore Airlines V NLRCBandar TingaoAinda não há avaliações
- Process Analysis at Arnold Palmer Hospital PDFDocumento2 páginasProcess Analysis at Arnold Palmer Hospital PDFxander syAinda não há avaliações
- Bayrampour HamidehDocumento267 páginasBayrampour HamidehRohamonangan TheresiaAinda não há avaliações
- Technical Notes Community Health NursingDocumento8 páginasTechnical Notes Community Health NursingMary JoyAinda não há avaliações
- 2015 Article 779Documento8 páginas2015 Article 779Eriekafebriayana RAinda não há avaliações
- IUFDDocumento33 páginasIUFDIrwin FitriansyahAinda não há avaliações
- CG237 2011-04 Common Ground MagazineDocumento44 páginasCG237 2011-04 Common Ground MagazineCommonGroundBCAinda não há avaliações
- Manual For Documenting Diagnosis in Per-Pd 301 - 2013 PDFDocumento33 páginasManual For Documenting Diagnosis in Per-Pd 301 - 2013 PDFNeeta AnandaAinda não há avaliações
- RRLDocumento4 páginasRRLGlessySeguillaBumanglagAinda não há avaliações
- Sample Case StudyDocumento31 páginasSample Case StudyMary Grace Mas50% (2)
- Biophysical ProfileDocumento26 páginasBiophysical ProfilePatricia Ysabelle Ledesma100% (1)
- (Augmentation) Medical and SurgicalDocumento17 páginas(Augmentation) Medical and SurgicalNadiya RashidAinda não há avaliações
- Poster Abstract Book PDFDocumento804 páginasPoster Abstract Book PDFRyan Michael OducadoAinda não há avaliações
- Birth AnatomyDocumento10 páginasBirth Anatomyelly fadhliahAinda não há avaliações
- Case Scenario Midterm (Mirul)Documento4 páginasCase Scenario Midterm (Mirul)NMDNMSSDAinda não há avaliações
- 9 Health Benefits of Eating Plums During PregnancyDocumento7 páginas9 Health Benefits of Eating Plums During PregnancyJulie MerrillAinda não há avaliações
- Web KFOG-jan-11Documento16 páginasWeb KFOG-jan-11kutra3000Ainda não há avaliações
- Community Health Nursing ExamsDocumento13 páginasCommunity Health Nursing ExamsAhrisJeannine EscuadroAinda não há avaliações
- 8 DoctorsorderDocumento5 páginas8 DoctorsorderErick SumicadAinda não há avaliações
- MaduraiDocumento108 páginasMaduraivelxerox4123Ainda não há avaliações
- Amniotic Fluid DisordersDocumento22 páginasAmniotic Fluid Disordersvictor onapaAinda não há avaliações
- Insulin Pumps and Pregnancy: ReviewDocumento5 páginasInsulin Pumps and Pregnancy: Reviewshona SharupaniAinda não há avaliações
- Il Effects of Dai Treatment FinalDocumento96 páginasIl Effects of Dai Treatment FinalDr SadiaAinda não há avaliações
- Postpartum Complications: Ahmed AliDocumento36 páginasPostpartum Complications: Ahmed AliPeter Osundwa KitekiAinda não há avaliações
- Massage Therapy EffectsDocumento12 páginasMassage Therapy EffectsEkalevi FahlepieAinda não há avaliações
- The Real Life Scenario Survival HandbookDocumento176 páginasThe Real Life Scenario Survival HandbookCubby ClubAinda não há avaliações
- 2009 HESI Practice - Comprehensive ExamDocumento26 páginas2009 HESI Practice - Comprehensive ExamQueennitaAinda não há avaliações