Você também pode gostar
- Basic Approach To Application of Liposomes PDFDocumento9 páginasBasic Approach To Application of Liposomes PDFalfox2000Ainda não há avaliações
- Cardiac Profiles of Liposomal Anthracyclines PDFDocumento12 páginasCardiac Profiles of Liposomal Anthracyclines PDFalfox2000Ainda não há avaliações
- Analytical Pharmacology PDFDocumento42 páginasAnalytical Pharmacology PDFalfox2000Ainda não há avaliações
- Irrational Use of Antibiotics and Role of The Pharmacist - An Insight From A Qualitative Study in New Delhi, India PDFDocumento6 páginasIrrational Use of Antibiotics and Role of The Pharmacist - An Insight From A Qualitative Study in New Delhi, India PDFalfox2000Ainda não há avaliações
- The Pharmacist - S Role in Preventing Antibiotic Resistance PDFDocumento8 páginasThe Pharmacist - S Role in Preventing Antibiotic Resistance PDFalfox2000Ainda não há avaliações
- Canadian Journal of DiabetesDocumento227 páginasCanadian Journal of DiabetesAnatolia MaresAinda não há avaliações
- Muscle Spasm Treatments PDFDocumento1 páginaMuscle Spasm Treatments PDFalfox2000Ainda não há avaliações
- Nab Technology PDFDocumento8 páginasNab Technology PDFalfox2000Ainda não há avaliações
- Ramadan DMDocumento7 páginasRamadan DMapi-3773951Ainda não há avaliações
- INTERNATIONAL NONPROPRIETARY For Biological and Biotechnological Products PDFDocumento35 páginasINTERNATIONAL NONPROPRIETARY For Biological and Biotechnological Products PDFalfox2000Ainda não há avaliações
- Emetogenic Potential of Antineoplastic Agents PDFDocumento1 páginaEmetogenic Potential of Antineoplastic Agents PDFalfox2000Ainda não há avaliações
- Dipeptidyl Peptidase Inhibits Malignant Phenotype of Prostate PDFDocumento11 páginasDipeptidyl Peptidase Inhibits Malignant Phenotype of Prostate PDFalfox2000Ainda não há avaliações
- Blood Glucose Monitors For Diabetes PDFDocumento2 páginasBlood Glucose Monitors For Diabetes PDFalfox2000Ainda não há avaliações
- CD26 Dipeptidyl Peptidase IV and Its Role in Cancer PDFDocumento7 páginasCD26 Dipeptidyl Peptidase IV and Its Role in Cancer PDFalfox2000Ainda não há avaliações
- Drug Disposal 0411Documento2 páginasDrug Disposal 0411i-callAinda não há avaliações
- Guidelines For Tablet Crushing and Administration Via Enteral Feeding Tubes PDFDocumento13 páginasGuidelines For Tablet Crushing and Administration Via Enteral Feeding Tubes PDFalfox2000Ainda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- End of Life Care IssuesDocumento4 páginasEnd of Life Care IssuesKAMAL ALSOFIANYAinda não há avaliações
- Mechanical Ventilator CareDocumento9 páginasMechanical Ventilator CareAnusha Verghese100% (2)
- Affordable medicines and medical suppliesDocumento12 páginasAffordable medicines and medical suppliesTrie Gusti linglingAinda não há avaliações
- Airway Management in The Critically Ill: ReviewDocumento9 páginasAirway Management in The Critically Ill: ReviewQuarmina HesseAinda não há avaliações
- Paracetamol - Drug StudyDocumento1 páginaParacetamol - Drug StudyPatricia Reese YutiamcoAinda não há avaliações
- Pharma CompaniesDocumento23 páginasPharma CompaniesSameer PawarAinda não há avaliações
- Data Obat PC 11022019Documento23 páginasData Obat PC 11022019Panji Novantara100% (1)
- Dexamethasone Drug LiteratureDocumento1 páginaDexamethasone Drug LiteratureOneForAll :Ainda não há avaliações
- SacubitrilValsartan (Entresto) For Heart FailureDocumento2 páginasSacubitrilValsartan (Entresto) For Heart FailureWatchara TansiriAinda não há avaliações
- CovidDocumento110 páginasCovidHendhy WaluyoAinda não há avaliações
- Clinical Pharmacy - Introduction - : Prepared By: Dr. C. Suhas ReddyDocumento20 páginasClinical Pharmacy - Introduction - : Prepared By: Dr. C. Suhas Reddysuhas reddyAinda não há avaliações
- GINA Publications 2009Documento26 páginasGINA Publications 2009Jesus Alonso Hernandez AAinda não há avaliações
- Thesis On Topical Drug Delivery SystemDocumento7 páginasThesis On Topical Drug Delivery Systemjuliemoralesomaha100% (2)
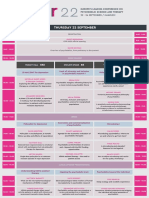
- Europe's Leading Conference on Psychedelic ScienceDocumento6 páginasEurope's Leading Conference on Psychedelic ScienceAndrei GeorgescuAinda não há avaliações
- JPMorgan 2021 Day 1Documento124 páginasJPMorgan 2021 Day 1Watson TianAinda não há avaliações
- Discharge Planning FinalDocumento3 páginasDischarge Planning FinalRae Marie AquinoAinda não há avaliações
- East Africa University Faculty of Health ScienceDocumento16 páginasEast Africa University Faculty of Health ScienceÆßdüllãhi Môhâmëd ÆbdíAinda não há avaliações
- Daftar Harga 11 September 2023Documento58 páginasDaftar Harga 11 September 2023Apotek Ibnu RusydAinda não há avaliações
- Personal View: Mark Abie Horowitz, David TaylorDocumento9 páginasPersonal View: Mark Abie Horowitz, David TaylorNoel Saúl Argüello SánchezAinda não há avaliações
- MMP Handy Chart October 2011 V2Documento37 páginasMMP Handy Chart October 2011 V2ColonAinda não há avaliações
- Instructions - For - Use ValtocoDocumento2 páginasInstructions - For - Use Valtocofreebass08Ainda não há avaliações
- Role of Lithium Augmentation in The Management of Major Depressive DisorderDocumento12 páginasRole of Lithium Augmentation in The Management of Major Depressive Disorderdanilomarandola100% (1)
- Phenylephrine: Pilar D'Ocon, Universidad de Valencia, Valencia, SpainDocumento6 páginasPhenylephrine: Pilar D'Ocon, Universidad de Valencia, Valencia, Spainarief budiman1Ainda não há avaliações
- Islamabad. Up-Gradation of Official WebsiteDocumento4 páginasIslamabad. Up-Gradation of Official WebsiteAli RizviAinda não há avaliações
- Ezetimibe (Zetia)Documento1 páginaEzetimibe (Zetia)E100% (1)
- Bioequivalence Study of Carbamazepine Tablets in Vitro in Vivo CorrelationDocumento8 páginasBioequivalence Study of Carbamazepine Tablets in Vitro in Vivo CorrelationFriska Aprianti100% (1)
- Dosage Calculations/Formulas For Nursing StudentsDocumento10 páginasDosage Calculations/Formulas For Nursing Studentsnalonso4908100% (1)
- Haloperidol Drug StudyDocumento3 páginasHaloperidol Drug StudyAysaaa DCAinda não há avaliações
- NAC Asthma COPD Medications Chart 2022 - A4 - WebDocumento1 páginaNAC Asthma COPD Medications Chart 2022 - A4 - WebkanemuraaAinda não há avaliações
- Intraosseous Infusion: Lizlin Noemi Bajada Pedia Department 8/27/2021Documento18 páginasIntraosseous Infusion: Lizlin Noemi Bajada Pedia Department 8/27/2021Lizlin Noemi BajadaAinda não há avaliações