Você também pode gostar
- Cold Shock ResponseDocumento2 páginasCold Shock ResponsezxczxzczxAinda não há avaliações
- CookieDocumento5 páginasCookiezxczxzczxAinda não há avaliações
- GastritisDocumento6 páginasGastritiszxczxzczxAinda não há avaliações
- NMAT - 2007: Top Careers & YouDocumento8 páginasNMAT - 2007: Top Careers & YouzxczxzczxAinda não há avaliações
- Blood DifferentialsDocumento3 páginasBlood DifferentialsJustin EduardoAinda não há avaliações
- Latin America Neo-Colonialism and OverpopulationDocumento7 páginasLatin America Neo-Colonialism and OverpopulationzxczxzczxAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- MegabacteriaDocumento2 páginasMegabacteriaapi-245199183Ainda não há avaliações
- Qualis Medicina Veterinaria 2023 Classificacao de Periodicos Quadrienio 2017 2020Documento66 páginasQualis Medicina Veterinaria 2023 Classificacao de Periodicos Quadrienio 2017 2020bruno silvaAinda não há avaliações
- Khan Academy Notes - Biomolecules For MCATDocumento50 páginasKhan Academy Notes - Biomolecules For MCATJuanAinda não há avaliações
- 012 Analysis of Reticulocyte Parameters On The Sysmex XEDocumento8 páginas012 Analysis of Reticulocyte Parameters On The Sysmex XEblanket_thAinda não há avaliações
- Hershey ChaseDocumento1 páginaHershey Chasemkohli64Ainda não há avaliações
- Genetics Extra CreditDocumento3 páginasGenetics Extra CreditNicole Leigh KleinasAinda não há avaliações
- Application of The Bethesda Classification For Thyroid FNABDocumento12 páginasApplication of The Bethesda Classification For Thyroid FNABJudrelle Krizia MarianoAinda não há avaliações
- c20 Microbiology Tortora TestbankDocumento19 páginasc20 Microbiology Tortora Testbankwhitewave25100% (1)
- 神经生物学Documento58 páginas神经生物学jdskydtAinda não há avaliações
- Chemotherapy: Chemotherapy, in Its Most General Sense, Refers To Treatment of Disease byDocumento42 páginasChemotherapy: Chemotherapy, in Its Most General Sense, Refers To Treatment of Disease byMalueth AnguiAinda não há avaliações
- Essential, Trace, and Nonessential Ions-1Documento3 páginasEssential, Trace, and Nonessential Ions-1John AndanAinda não há avaliações
- Drosophila MelanogasterDocumento13 páginasDrosophila MelanogasterDavid MorganAinda não há avaliações
- Midline DiastemaDocumento4 páginasMidline DiastemasmritiAinda não há avaliações
- Chapter 4 Drug MetabolismDocumento14 páginasChapter 4 Drug MetabolismNicole AguilarAinda não há avaliações
- SCE Practicaldiabetes - ElzohryDocumento107 páginasSCE Practicaldiabetes - ElzohryAE67% (3)
- Chapter 6: Physiology Questionbank Summary: Enzym E Source Optimum PH Substrate ProductsDocumento3 páginasChapter 6: Physiology Questionbank Summary: Enzym E Source Optimum PH Substrate ProductsAshmita KumarAinda não há avaliações
- Recent Advances in The Research of Milbemycin Biosynthesis and Regulation As Well As Strategies For Strain ImprovementDocumento9 páginasRecent Advances in The Research of Milbemycin Biosynthesis and Regulation As Well As Strategies For Strain Improvementneo.mx8Ainda não há avaliações
- Examiners' Report June 2011 GCE Biology 6BI05 01Documento36 páginasExaminers' Report June 2011 GCE Biology 6BI05 01Annie FrancesAinda não há avaliações
- Animal Cloning PDFDocumento6 páginasAnimal Cloning PDFDaniAinda não há avaliações
- Incomplete Abortion MINI CASE STUDY Group 3Documento23 páginasIncomplete Abortion MINI CASE STUDY Group 3Katrina TinapianAinda não há avaliações
- Cartilage: Ethel Marie M. Mangada, RMTDocumento34 páginasCartilage: Ethel Marie M. Mangada, RMTAesthetics MinAinda não há avaliações
- Blood Banking and Serology and Immunology - Refresher Exam With AnswersDocumento8 páginasBlood Banking and Serology and Immunology - Refresher Exam With AnswersPaul Espinosa88% (25)
- Restriction EndonucleaseDocumento4 páginasRestriction EndonucleaseGaurav PandeyAinda não há avaliações
- General Pharmacology MCQs PDFDocumento41 páginasGeneral Pharmacology MCQs PDFTaonga Zulu90% (21)
- Cancer Cell Structures, Carcinogens and Genomic Instability (Leon P. Bignold 2006)Documento376 páginasCancer Cell Structures, Carcinogens and Genomic Instability (Leon P. Bignold 2006)Raihan UchihaAinda não há avaliações
- Thyroid WorkbookDocumento17 páginasThyroid Workbookpinkyhead99100% (1)
- Quiz 1A Hema LecDocumento17 páginasQuiz 1A Hema LecAngela ReyesAinda não há avaliações
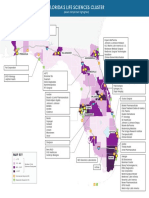
- (Select Companies Highlighted) : Tallahassee Jacksonville PensacolaDocumento1 página(Select Companies Highlighted) : Tallahassee Jacksonville PensacolaCocoAinda não há avaliações
- Cognitive Performance After Postoperative Pituitary Radiotherapy: A Dosimetric Study of The Hippocampus and The Prefrontal CortexDocumento9 páginasCognitive Performance After Postoperative Pituitary Radiotherapy: A Dosimetric Study of The Hippocampus and The Prefrontal CortexManishKondapuramAinda não há avaliações