Você também pode gostar
- Resources To Guide Exercise Specialists Managing Adults With DiabetesDocumento11 páginasResources To Guide Exercise Specialists Managing Adults With DiabetesArie AnggaAinda não há avaliações
- Resources To Guide Exercise Specialists Managing Adults With DiabetesDocumento13 páginasResources To Guide Exercise Specialists Managing Adults With Diabeteslaura valentina ochoa ordoñezAinda não há avaliações
- Carboidrato No Contexto Do Exercício Físico em Diabéticos Tipo 1Documento21 páginasCarboidrato No Contexto Do Exercício Físico em Diabéticos Tipo 1Duda FranchiAinda não há avaliações
- The Essential Role of Exercise in The Management of Type 2 DiabetesDocumento11 páginasThe Essential Role of Exercise in The Management of Type 2 DiabetesRadu MaricicaAinda não há avaliações
- JFMK 05 00070 v2Documento11 páginasJFMK 05 00070 v2Santy OktavianiAinda não há avaliações
- Editorial Article Exercise and Diabetes Mellitus: Polikandrioti MDocumento2 páginasEditorial Article Exercise and Diabetes Mellitus: Polikandrioti Mladawantham_58372076Ainda não há avaliações
- Management of Competitive Athletes With Diabetes: in BriefDocumento6 páginasManagement of Competitive Athletes With Diabetes: in BriefDeritanti Fitria RiskianaAinda não há avaliações
- Research Article: Acute Whole Body Vibration Decreases The Glucose Levels in Elderly Diabetic WomenDocumento8 páginasResearch Article: Acute Whole Body Vibration Decreases The Glucose Levels in Elderly Diabetic WomenStefanny AmahorsejaAinda não há avaliações
- Exercise and Type 1 Diabetes (T1DM)Documento28 páginasExercise and Type 1 Diabetes (T1DM)pb.nakulaAinda não há avaliações
- Clinical Aspects of Physical Exercise For Diabetes/metabolic SyndromeDocumento5 páginasClinical Aspects of Physical Exercise For Diabetes/metabolic SyndromecokimasterAinda não há avaliações
- Diabetes in SportsDocumento11 páginasDiabetes in SportsstefanAinda não há avaliações
- Exercise and Type 2 Diabetes: Molecular Mechanisms Regulating Glucose Uptake in Skeletal MuscleDocumento7 páginasExercise and Type 2 Diabetes: Molecular Mechanisms Regulating Glucose Uptake in Skeletal MuscleArie AnggaAinda não há avaliações
- Colberg 2009 2511457365Documento8 páginasColberg 2009 2511457365fedelarru9Ainda não há avaliações
- Exercise and Diabetes: A Clinician's Guide to Prescribing Physical ActivityNo EverandExercise and Diabetes: A Clinician's Guide to Prescribing Physical ActivityAinda não há avaliações
- MISS. MODERATE. Superior Quanto Á Insulina. The Effect of Vigorous - Versus Moderate-Intensity Aerobic Exercise On Insulin Action. Mcgarrah2016Documento6 páginasMISS. MODERATE. Superior Quanto Á Insulina. The Effect of Vigorous - Versus Moderate-Intensity Aerobic Exercise On Insulin Action. Mcgarrah2016Paolo AltoéAinda não há avaliações
- Exercise - Physical Activity in Individuals With Type 2 Diabet... - Medicine & Science in Sports & ExerciseDocumento51 páginasExercise - Physical Activity in Individuals With Type 2 Diabet... - Medicine & Science in Sports & ExerciseRicardo Arellano GarcíaAinda não há avaliações
- Diabetes Physical Actvity RecommendationDocumento61 páginasDiabetes Physical Actvity RecommendationMai GaberAinda não há avaliações
- 673 FullDocumento4 páginas673 FullIba SuprasabaAinda não há avaliações
- dc11-1655 Full PDFDocumento7 páginasdc11-1655 Full PDFhfathiardiAinda não há avaliações
- Clinical Aspects of Physical Exercise For Diabetes/metabolic SyndromeDocumento5 páginasClinical Aspects of Physical Exercise For Diabetes/metabolic Syndromeprofesi nersAinda não há avaliações
- Diabetes No Atleta CompetitivoDocumento7 páginasDiabetes No Atleta CompetitivojosiAinda não há avaliações
- 126 MG DL DL 200 MG DLDocumento16 páginas126 MG DL DL 200 MG DLDaian Cruz DiasAinda não há avaliações
- Abastecendo o Atleta Com Diabetes Tipo 1Documento7 páginasAbastecendo o Atleta Com Diabetes Tipo 1josiAinda não há avaliações
- Resistance Training For Diabetes Prevention and Therapy - Experimental Findings and Molecular Mechanisms (Strasser & Pesta, 2012)Documento8 páginasResistance Training For Diabetes Prevention and Therapy - Experimental Findings and Molecular Mechanisms (Strasser & Pesta, 2012)Gonzalo GonzalesAinda não há avaliações
- Low-Volume High-Intensity Interval Training Reduces Hyperglycemia and Increases Muscle Mitochondrial Capacity in Patients With Type 2 DiabetesDocumento7 páginasLow-Volume High-Intensity Interval Training Reduces Hyperglycemia and Increases Muscle Mitochondrial Capacity in Patients With Type 2 DiabetesSafira Ridha UlyaAinda não há avaliações
- Effectiveness and Safety of High-Intensity Interval Training in Patients With Type 2 DiabetesDocumento6 páginasEffectiveness and Safety of High-Intensity Interval Training in Patients With Type 2 DiabetesMumtaz Maulana HidayatAinda não há avaliações
- Pe 07010Documento12 páginasPe 07010Arie AnggaAinda não há avaliações
- Exercise in ObesityDocumento8 páginasExercise in ObesitywidyaAinda não há avaliações
- Example 6Documento4 páginasExample 6Tutor BlairAinda não há avaliações
- Lakka 2007Documento13 páginasLakka 2007Neha RauhilaAinda não há avaliações
- Diet and TherapyDocumento3 páginasDiet and TherapyKatty AlevonAinda não há avaliações
- Nutrition For Endurance Sports: Marathon, Triathlon, and Road CyclingDocumento9 páginasNutrition For Endurance Sports: Marathon, Triathlon, and Road CyclingcakebakeshakeAinda não há avaliações
- Exercise and Adlib Eating in Obese Individuals Med Sci Sports Med Nov 2010Documento8 páginasExercise and Adlib Eating in Obese Individuals Med Sci Sports Med Nov 2010Andrew OgundeleAinda não há avaliações
- Diabetes GuidelineDocumento4 páginasDiabetes GuidelinenetoAinda não há avaliações
- Exercises For DiabetesDocumento25 páginasExercises For DiabetesrichaAinda não há avaliações
- Exercise and DiabetesDocumento4 páginasExercise and DiabetesImmanuel LashleyAinda não há avaliações
- 516 Physical Activity and Exercise and Diabetes MellitusDocumento5 páginas516 Physical Activity and Exercise and Diabetes MellituslaurentiaoktaviaAinda não há avaliações
- Physiotherapy DiabetesDocumento5 páginasPhysiotherapy DiabetessalmanmohammedAinda não há avaliações
- Hansen 2016 Impact of Endurance Exercise Training in The Fasted StateDocumento14 páginasHansen 2016 Impact of Endurance Exercise Training in The Fasted StateYo Vivo Fit Pablo y KarlaAinda não há avaliações
- Physical Activity, Sport, and Pediatric Diabetes: Review ArticleDocumento11 páginasPhysical Activity, Sport, and Pediatric Diabetes: Review ArticleNicole GreeneAinda não há avaliações
- The Importance of Exercise For Glycemic Control in Type 2 DiabetesDocumento10 páginasThe Importance of Exercise For Glycemic Control in Type 2 DiabetesAhmed AmerAinda não há avaliações
- Ketogenic Diet IF-Philippine Lipid Society Consensus-Statement-20191108v4Documento21 páginasKetogenic Diet IF-Philippine Lipid Society Consensus-Statement-20191108v4donmd98Ainda não há avaliações
- Diabetes Type TwoDocumento6 páginasDiabetes Type TwoDismas OdhiamboAinda não há avaliações
- Exercise and Type 2 DiabetesDocumento15 páginasExercise and Type 2 Diabetespb.nakulaAinda não há avaliações
- Exercise in Children and Adolescents With Diabetes: ISPAD Clinical Practice Consensus Guidelines 2009 CompendiumDocumento15 páginasExercise in Children and Adolescents With Diabetes: ISPAD Clinical Practice Consensus Guidelines 2009 CompendiumAzul MarinoAinda não há avaliações
- 5 ArticuloDocumento3 páginas5 ArticuloKarina AngelAinda não há avaliações
- InglesDocumento6 páginasInglesKuroKy KrausserAinda não há avaliações
- DefaultDocumento43 páginasDefaultKassandra EggersAinda não há avaliações
- Sindrom Metabolik Alwi ShahabDocumento10 páginasSindrom Metabolik Alwi ShahabIndah Hime AzzahraAinda não há avaliações
- Lifestyle Modification: Weight Control, Exercise, and Smoking CessationDocumento12 páginasLifestyle Modification: Weight Control, Exercise, and Smoking CessationsenthilAinda não há avaliações
- Diabetes and Physical ActivityDocumento6 páginasDiabetes and Physical ActivityFahmi Fauzi SugandiAinda não há avaliações
- Sindrom MetabolikDocumento9 páginasSindrom MetabolikUlquiorra SchifferAinda não há avaliações
- Menopause ExerciseDocumento8 páginasMenopause ExerciseWittapong SinsoongsudAinda não há avaliações
- Pag 10Documento11 páginasPag 10Jesús Adolfo Alarcón GómezAinda não há avaliações
- The Power Of Intermittent Fasting: How To Lose Weight And Improve Your HealthNo EverandThe Power Of Intermittent Fasting: How To Lose Weight And Improve Your HealthAinda não há avaliações
- Type 2 Diabetes Mellitus (Article) Author United States Department of Veterans AffairsDocumento9 páginasType 2 Diabetes Mellitus (Article) Author United States Department of Veterans Affairsnaljnaby9Ainda não há avaliações
- Exercise Intervention Under Hypoxic Condition As A New TherapeuticDocumento14 páginasExercise Intervention Under Hypoxic Condition As A New TherapeuticnorazmiAinda não há avaliações
- Rehabilitation in Diabetic Patients.: PmidDocumento3 páginasRehabilitation in Diabetic Patients.: PmidIoana PiticarAinda não há avaliações
- Alphatrak 2 User GuideDocumento23 páginasAlphatrak 2 User GuideGlenn MartynAinda não há avaliações
- CBG RetdemDocumento7 páginasCBG Retdemadd.bdrcAinda não há avaliações
- A Review On Antidiabetic Plants Used by The People of Manipur Charactirized by Hypoglycemic ActivityDocumento9 páginasA Review On Antidiabetic Plants Used by The People of Manipur Charactirized by Hypoglycemic ActivityHemant MahaleAinda não há avaliações
- Megha Jain's ReportDocumento26 páginasMegha Jain's Reportmegha jainAinda não há avaliações
- US Army Medical Course MD0863-200 - Clinical Chemistry IIDocumento98 páginasUS Army Medical Course MD0863-200 - Clinical Chemistry IIGeorgesAinda não há avaliações
- So What Is Juvenile DiabetesDocumento6 páginasSo What Is Juvenile Diabetesapi-274083684Ainda não há avaliações
- Protocolo Da BombaDocumento52 páginasProtocolo Da BombaEmerson SaAinda não há avaliações
- CBT - Pharmacology EditedDocumento27 páginasCBT - Pharmacology EditedReshma BhogalAinda não há avaliações
- Endocrine Problems of The Adult ClientDocumento18 páginasEndocrine Problems of The Adult ClientMarylle AntonioAinda não há avaliações
- Hypoglycemia UMYDocumento60 páginasHypoglycemia UMYTommy AkromaAinda não há avaliações
- Natural Medicines Used in The Traditional Chinese Medical System For Therapy of Diabetes MellitusDocumento21 páginasNatural Medicines Used in The Traditional Chinese Medical System For Therapy of Diabetes MellitusparibashaiAinda não há avaliações
- Journal of Ethnopharmacology: Trilobata (L.) Pruski Flower in RatsDocumento7 páginasJournal of Ethnopharmacology: Trilobata (L.) Pruski Flower in RatsHeriansyah S1 FarmasiAinda não há avaliações
- Clinical and Biochemical Characteristics of High-Intensity Functional Training (HIFT) and Overtraining Syndrome PDFDocumento12 páginasClinical and Biochemical Characteristics of High-Intensity Functional Training (HIFT) and Overtraining Syndrome PDFElaine CspAinda não há avaliações
- Iron PoisoningDocumento10 páginasIron PoisoningOoi Ah Guan100% (1)
- Pharmacological Activities of BioactiveDocumento24 páginasPharmacological Activities of BioactiveDe'Uma Beiby SwettyAinda não há avaliações
- DM and PregnancyDocumento71 páginasDM and PregnancyBrex Supp50% (2)
- Fenugreek On DiabetesDocumento3 páginasFenugreek On DiabetesDr Dushyant Kamal DhariAinda não há avaliações
- Intermittent Fasting Cheat Sheet PDFDocumento30 páginasIntermittent Fasting Cheat Sheet PDFjong bariquit89% (9)
- Today's Dietitian - August 2014Documento68 páginasToday's Dietitian - August 2014japanka11Ainda não há avaliações
- Endocrine SystemDocumento41 páginasEndocrine SystemMerrin EncarnacionAinda não há avaliações
- Updated For Diabetes Mellitus: Krairat Komdee, MD. Department of Internal Medicine Phayao HospitalDocumento47 páginasUpdated For Diabetes Mellitus: Krairat Komdee, MD. Department of Internal Medicine Phayao HospitalKrairat KomdeeAinda não há avaliações
- UltraMetabolism Guide PDFDocumento108 páginasUltraMetabolism Guide PDFMihaela Cristina Munteanu100% (1)
- Glicosimetro - FreeStyle OptiumH - ART20287 - Rev-BDocumento29 páginasGlicosimetro - FreeStyle OptiumH - ART20287 - Rev-BAdriano MartinsAinda não há avaliações
- EndoquestionssolvedDocumento14 páginasEndoquestionssolvedPuteri Nursyamimi Mohd SabilanAinda não há avaliações
- Glucose HK PDFDocumento3 páginasGlucose HK PDFاختصاص سريريةAinda não há avaliações
- Inborn Errors or MetabolismDocumento21 páginasInborn Errors or Metabolismsaleema11Ainda não há avaliações
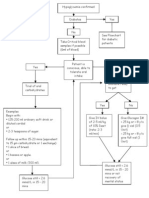
- Hypoglycaemia FlowchartDocumento1 páginaHypoglycaemia FlowchartMohammad SultanAinda não há avaliações
- Health Tips For Ramad - 1Documento9 páginasHealth Tips For Ramad - 1Syahrizul Fadly MadelliAinda não há avaliações
- Intermittent FastingDocumento14 páginasIntermittent FastingchloevagyokAinda não há avaliações