Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Plutonium Nitricum M R7C8Documento4 páginasPlutonium Nitricum M R7C8nitkolAinda não há avaliações
- Ultrasonic Examination Report: Wayland EngineeringDocumento1 páginaUltrasonic Examination Report: Wayland EngineeringDeepak100% (1)
- API 580 Questions ModDocumento18 páginasAPI 580 Questions ModDeepak100% (1)
- Vinod Final Polyplex-1Documento103 páginasVinod Final Polyplex-1Fan of carry minatiAinda não há avaliações
- IEEE Power and Energy Magazine Volume 9 Issue 3 2011 (Doi 10.1109/mpe.2011.940579) Katiraei, K.F. Agüero, J.R. - Solar PV Integration ChallengesDocumento10 páginasIEEE Power and Energy Magazine Volume 9 Issue 3 2011 (Doi 10.1109/mpe.2011.940579) Katiraei, K.F. Agüero, J.R. - Solar PV Integration Challengesjagadeeshkumar116100% (1)
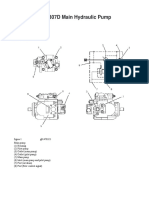
- Cat 307D Main Pump OperationDocumento3 páginasCat 307D Main Pump Operationkahandawala100% (1)
- Mechanis Quizbee in Math and ScienceDocumento4 páginasMechanis Quizbee in Math and ScienceChristine De San Jose80% (5)
- Get Big Stay LeanDocumento87 páginasGet Big Stay LeanMatheus Buniotto100% (1)
- 29 7 16Cl4EETestPortionDocumento1 página29 7 16Cl4EETestPortionDeepakAinda não há avaliações
- Icml Mla IDocumento3 páginasIcml Mla IDeepak100% (1)
- BS English 17-04-2020Documento10 páginasBS English 17-04-2020DeepakAinda não há avaliações
- Icml Mla IiDocumento3 páginasIcml Mla IiDeepak100% (2)
- CL 4 PPT Animal World For Flipped LearningDocumento7 páginasCL 4 PPT Animal World For Flipped LearningDeepakAinda não há avaliações
- 5 8 16Cl4MathsTestportionDocumento1 página5 8 16Cl4MathsTestportionDeepakAinda não há avaliações
- Syllabus Barc Rtl2 160714Documento7 páginasSyllabus Barc Rtl2 160714DeepakAinda não há avaliações
- FortiGate 30DDocumento4 páginasFortiGate 30DIulianAinda não há avaliações
- Subject - Hindi Class IV Date of Test: 08-07-16 TopicDocumento1 páginaSubject - Hindi Class IV Date of Test: 08-07-16 TopicDeepakAinda não há avaliações
- The School Is The Temple of LearningDocumento2 páginasThe School Is The Temple of LearningDeepakAinda não há avaliações
- XL Go Data SheetDocumento4 páginasXL Go Data SheetDeepakAinda não há avaliações
- Here Is The MoonDocumento2 páginasHere Is The MoonDeepakAinda não há avaliações
- Q.1) Pick Out Three Adjectives and Write Them in The Place Given BelowDocumento2 páginasQ.1) Pick Out Three Adjectives and Write Them in The Place Given BelowDeepakAinda não há avaliações
- NDT Methods AvailableDocumento1 páginaNDT Methods AvailableDeepakAinda não há avaliações
- Tripride 1 Equivalent PDFDocumento4 páginasTripride 1 Equivalent PDFDeepakAinda não há avaliações
- Welding Procedure Specification: Technip KT India LimitedDocumento5 páginasWelding Procedure Specification: Technip KT India LimitedDeepak100% (1)
- Nozzle Location Plate Identification Thickness Location E W N SDocumento9 páginasNozzle Location Plate Identification Thickness Location E W N SDeepakAinda não há avaliações
- Survey Form: Delhi Public School, Bopal, Ahmedabad Topic: Water, Water Everywhere Conservation of WaterDocumento2 páginasSurvey Form: Delhi Public School, Bopal, Ahmedabad Topic: Water, Water Everywhere Conservation of WaterDeepakAinda não há avaliações
- TR200Documento3 páginasTR200DeepakAinda não há avaliações
- TR210Documento2 páginasTR210DeepakAinda não há avaliações
- Life Without LimitsDocumento31 páginasLife Without LimitsDeepakAinda não há avaliações
- Surface Roughness Tester TR100: Technical SpecificationsDocumento1 páginaSurface Roughness Tester TR100: Technical SpecificationsDeepakAinda não há avaliações
- Surface Roughness Tester TR110: Technical Specifications Standard DeliveryDocumento1 páginaSurface Roughness Tester TR110: Technical Specifications Standard DeliveryDeepakAinda não há avaliações
- Vibration Tester TV110: Technical SpecificationsDocumento1 páginaVibration Tester TV110: Technical SpecificationsDeepakAinda não há avaliações
- Vibration Pen TV200/220/260: Technical SpecificationsDocumento1 páginaVibration Pen TV200/220/260: Technical SpecificationsDeepakAinda não há avaliações
- PPEA-WI-016 Management of ChangeDocumento3 páginasPPEA-WI-016 Management of ChangeDeepakAinda não há avaliações
- PPEA-WI-016 Management of ChangeDocumento3 páginasPPEA-WI-016 Management of ChangeDeepakAinda não há avaliações
- PPEA-WI-012 - B Consultation and Communication at SiteDocumento6 páginasPPEA-WI-012 - B Consultation and Communication at SiteDeepakAinda não há avaliações
- Deck Cranes PDFDocumento7 páginasDeck Cranes PDFIndra Ranu KusumaAinda não há avaliações
- TALAT Lecture 1253: CreepDocumento26 páginasTALAT Lecture 1253: CreepCORE Materials100% (1)
- Fundamentals of Radiologic Physics Course OutlineDocumento7 páginasFundamentals of Radiologic Physics Course OutlineJustin Zeus Operio100% (1)
- Manjung 4 Malaysia Ultra Supercritical Coal PlantDocumento2 páginasManjung 4 Malaysia Ultra Supercritical Coal PlantAlanSoo100% (1)
- Decarbonization MagazineDocumento86 páginasDecarbonization MagazineSynergy IndustriesAinda não há avaliações
- UL Cyber ParkDocumento9 páginasUL Cyber ParkGeet RangAinda não há avaliações
- CALEFACCION Combitronic - 22297Documento20 páginasCALEFACCION Combitronic - 22297AlbertoAinda não há avaliações
- PV Cell CharaDocumento40 páginasPV Cell CharaBlessy JoyAinda não há avaliações
- Detailed CalculationsDocumento14 páginasDetailed CalculationsrozAinda não há avaliações
- 7W Amplifier Circuit TDA2003Documento7 páginas7W Amplifier Circuit TDA2003Mar EscAinda não há avaliações
- SMK0765FJ: Switching Regulator ApplicationsDocumento8 páginasSMK0765FJ: Switching Regulator ApplicationsranaateeqAinda não há avaliações
- RFP Iecc KochiDocumento73 páginasRFP Iecc KochiCUBE ProjectsAinda não há avaliações
- A New Development in Completion Methods - The Limited Entry TechniqueDocumento8 páginasA New Development in Completion Methods - The Limited Entry TechniqueJosé TimanáAinda não há avaliações
- Jurong Junior College: Preliminary Examination 2008Documento13 páginasJurong Junior College: Preliminary Examination 2008Ronald McdonaldAinda não há avaliações
- For Less: Stack MoreDocumento12 páginasFor Less: Stack MoreKshitiz MittalAinda não há avaliações
- Accident Prevention Program: Thunderstorms - Don't Flirt ... Skirt'EmDocumento5 páginasAccident Prevention Program: Thunderstorms - Don't Flirt ... Skirt'EmLohrasp SuraliwalaAinda não há avaliações
- UT Dallas Syllabus For Phys3341.001.11f Taught by Mark Lee (mxl101000)Documento5 páginasUT Dallas Syllabus For Phys3341.001.11f Taught by Mark Lee (mxl101000)UT Dallas Provost's Technology GroupAinda não há avaliações
- Unit 1 Solar EnergyDocumento176 páginasUnit 1 Solar EnergyAkhil Dayalu100% (1)
- Header SizeDocumento1 páginaHeader SizeNaufal HadiAinda não há avaliações
- Air Circuit Breakers For The 21st Century: Catalogue No.'00-P55EDocumento4 páginasAir Circuit Breakers For The 21st Century: Catalogue No.'00-P55EAsif ShahAinda não há avaliações
- National Electrical Safety Code OverviewDocumento15 páginasNational Electrical Safety Code OverviewLuis MurilloAinda não há avaliações
- Design HydSysDocumento1 páginaDesign HydSysManikandan RamalingamAinda não há avaliações
- NSGAFÖU 1,8/3 KV: Product InformationDocumento3 páginasNSGAFÖU 1,8/3 KV: Product InformationAttila HorvathAinda não há avaliações
- High Pressure Drilling Hoses: Fleximak Industrial CatalogueDocumento5 páginasHigh Pressure Drilling Hoses: Fleximak Industrial CatalogueitangAinda não há avaliações